Acute GE MANAGEMENT
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have sufficient comprehensive content. Here is the full management guide for Acute Gastroenteritis:
Acute Gastroenteritis (GE) — Management
1. Initial Assessment
History
Key features to elicit:
- Duration of symptoms (diarrhea >14 days = persistent/chronic, not acute)
- Stool character: watery vs. bloody, volume per episode
- Associated symptoms: vomiting, fever, abdominal pain, tenesmus
- Exposure history: foreign travel, raw seafood, undercooked meat, camping/untreated water, recent antibiotics, daycare, outbreaks
Bloody diarrhea + fever + tenesmus → dysentery pattern → suggests invasive organisms (Campylobacter, Shigella) Large volume watery diarrhea → small bowel involvement (viral, cholera) Vomiting predominating, little diarrhea → norovirus or preformed toxin (Staph aureus)
Physical Examination
Focus on:
- Hydration status: dry mucous membranes, decreased skin turgor, sunken eyes (especially in children), reduced urine output
- Vital signs: hypotension + tachycardia → significant dehydration; fever + altered mental status → possible sepsis
- Abdominal exam: hyperactive bowel sounds are typical; focal tenderness, rebound, guarding, distension or rigidity → suspect surgical cause
Differential Diagnoses to Exclude
Small bowel obstruction, appendicitis, diverticulitis, IBD, ischemic bowel, pancreatitis, hepatobiliary pathology, celiac disease, irritable bowel syndrome.
2. Severity / Dehydration Assessment
Use the Clinical Dehydration Score (especially in children):
| Score | General Appearance | Eyes | Oral Mucosa | Tears |
|---|---|---|---|---|
| 0 | Normal | Normal | Moist | Normal |
| 1 | Thirsty, restless, or irritable | Mildly sunken | Sticky | Decreased |
| 2 | Drowsy/non-responsive, limp, cold, diaphoretic | Very sunken | Dry | None |
- Score 0 = no dehydration
- Score 1–4 = some dehydration
- Score ≥5 = moderate–severe dehydration
Dehydration categories:
- Mild (<5% body weight loss): thirsty, normal exam
- Moderate (5–10%): tachycardia, dry mucosae, decreased skin turgor
- Severe (>10%): hypotension, altered mental status, markedly decreased urine output, shock
3. Investigations
| Test | When |
|---|---|
| Serum glucose | All infants/young children (hypoglycemia up to 9% prevalence) |
| Serum electrolytes | Moderate–severe dehydration, prolonged illness, very young infants, IV fluid therapy needed |
| CBC | Ill-appearing patient, bloody diarrhea (identify bacterial enterocolitis, HUS) |
| Stool culture | Bloody diarrhea, fever, travel history, outbreaks, immunocompromised → send for Campylobacter, E. coli O157:H7, Salmonella, Shigella, Yersinia |
| Stool toxin assay | Non-O157:H7 Shiga toxin-producing E. coli |
| C. difficile testing | Recent antibiotics, community-acquired, hospitalised patients |
Note: WBC and CRP are NOT reliable to distinguish viral vs. bacterial gastroenteritis. Stool cultures have a low yield in mild, uncomplicated cases.
4. Rehydration — The Cornerstone of Treatment
Oral Rehydration Therapy (ORT) — First-line for mild–moderate dehydration
ORT is equivalent to IV therapy in children with acute gastroenteritis for rehydration, reduction of subsequent diarrhea episodes, and prevention of complications. It is recommended by the AAP, WHO, and European Society of Pediatric Gastroenterology.
ORS options:
| Solution | Osmolarity |
|---|---|
| Standard WHO ORS | 331 mOsm/kg |
| Reduced osmolarity WHO ORS | 245 mOsm/kg (preferred — less vomiting, less stool output) |
| Pedialyte (children) | 250 mOsm/kg |
In children with mild gastroenteritis and minimal dehydration, dilute apple juice followed by preferred fluids is an acceptable alternative and results in fewer treatment failures than standard ORS.
Protocol:
- Mild dehydration: 50 mL/kg ORS over 4 hours
- Moderate dehydration: 100 mL/kg ORS over 4 hours
- Supplement with 10 mL/kg per liquid stool and 2 mL/kg per vomiting episode
- Give small, frequent sips if vomiting is present
IV Rehydration — for moderate–severe dehydration or ORT failure
- Normal saline (0.9% NaCl) or Lactated Ringer's bolus 20 mL/kg IV, repeat as needed
- Transition to oral rehydration as soon as tolerated
- Reassess hydration status after each bolus
5. Antiemetics
| Drug | Notes |
|---|---|
| Ondansetron (0.15 mg/kg IV/PO; max 4–8 mg) | First-line; reduces vomiting, decreases IV fluid need, improves ORT success; systematic review supports use in pediatric gastroenteritis |
| Metoclopramide | Alternative in adults |
| Promethazine | Avoid in children <2 years (respiratory depression risk) |
6. Antidiarrheals
| Drug | Notes |
|---|---|
| Loperamide | Useful in adults with non-dysenteric traveler's diarrhea; avoid in children, bloody diarrhea, or suspected invasive infection |
| Bismuth subsalicylate | Can reduce stool frequency; caution in children (Reye's syndrome risk) |
Do not use antidiarrheals in dysenteric illness (bloody diarrhea, high fever) — risk of toxic megacolon, worsened HUS.
7. Antibiotics
Most acute gastroenteritis is viral — antibiotics are NOT routinely indicated.
Empiric antibiotics are considered when:
- Severe dysenteric illness (high fever, bloody diarrhea)
- Immunocompromised patient
- Traveler's diarrhea (moderate–severe)
- Suspected cholera
| Organism | Antibiotic of Choice |
|---|---|
| Campylobacter | Azithromycin 500 mg OD × 3 days (or ciprofloxacin, but resistance rising) |
| Shigella | Azithromycin or ciprofloxacin × 3–5 days |
| Salmonella (non-typhoidal) | Usually self-limiting; treat if severe, elderly, immunocompromised → fluoroquinolone or azithromycin |
| Typhoid (Salmonella typhi) | Azithromycin or ceftriaxone |
| C. difficile | Oral vancomycin 125 mg QID × 10 days (preferred); metronidazole if mild |
| Traveler's diarrhea | Azithromycin or rifaximin × 3 days |
| Cholera | Doxycycline 300 mg single dose; azithromycin in children/pregnant |
| E. coli O157:H7 (STEC) | Avoid antibiotics — increases risk of HUS |
| Giardia | Metronidazole 250 mg TID × 7–10 days or tinidazole single dose |
| Cryptosporidium | Nitazoxanide (especially in immunocompromised) |
8. Diet and Feeding
- Early refeeding is encouraged once rehydration is underway — fasting worsens bowel absorptive capacity
- Resume age-appropriate diet as soon as tolerated
- In children, breastfeeding should continue throughout illness
- Avoid: sugary drinks, apple juice (full strength), carbonated beverages (hyperosmolar — worsen diarrhea)
- Lactose restriction is generally not necessary unless clear lactose intolerance
9. Zinc Supplementation (Children)
- WHO recommends zinc 10–20 mg/day × 10–14 days in children <5 years in developing settings
- Reduces severity and duration of diarrhea, decreases risk of future episodes
10. Probiotics
- Some evidence for Lactobacillus rhamnosus GG and Saccharomyces boulardii reducing duration of diarrhea by ~1 day in children
- Not universally recommended in all guidelines but reasonable adjunct
11. Disposition
| Criteria | Disposition |
|---|---|
| Well-appearing, minimal/no dehydration, tolerating ORT | Discharge with return precautions |
| Moderate dehydration responding to IV/ORT | Observe; discharge when tolerating fluids |
| Severe dehydration, persistent vomiting, unable to tolerate ORT | Admit |
| Bloody diarrhea with severe illness, sepsis signs | Admit + urgent investigation |
| Very young infants, elderly, immunocompromised, comorbidities | Lower threshold for admission |
Return precautions — advise to return if:
- No improvement in 48 hours
- Worsening symptoms, inability to keep fluids down
- Bloody stools, high fever
- Signs of worsening dehydration (markedly reduced urine output, extreme lethargy)
Key Pathogens Summary
| Pathogen | Incubation | Duration | Key Feature |
|---|---|---|---|
| Norovirus | 12–48 h | 1–3 days | Explosive vomiting, mild diarrhea, outbreaks |
| Rotavirus | 1–3 days | 3–8 days | Children <5, watery diarrhea |
| Campylobacter | 2–5 days | 5–14 days | Most common bacterial; dysentery, raw poultry |
| Salmonella (NTS) | 12–24 h | 2–7 days | Eggs/poultry; fever + watery diarrhea |
| Shigella | 1–2 days | 2–7 days | Dysentery, toxigenic; person-to-person |
| E. coli O157:H7 | 3–8 days | 5–10 days | Bloody diarrhea, HUS risk; avoid antibiotics |
| Staph aureus | 1–6 h | <24 h | Preformed toxin, rapid onset vomiting |
| C. difficile | Variable | Variable | Recent antibiotics, hospital-acquired |
| Giardia | 1–3 weeks | Weeks | Camping/water, bloating, fatty stools |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9th ed., Ch. 131
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Ch. 80
- Yamada's Textbook of Gastroenterology, 7th ed., Ch. Syndromic Management of Gastroenteritis
CVS examination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
cardiovascular examination JVP jugular venous pulse waveform
I have all the content needed. Let me now compile the comprehensive CVS examination guide.
Cardiovascular System (CVS) Examination
SEQUENCE OF EXAMINATION
General approach: Inspection → Pulse → Blood Pressure → JVP → Precordium (Inspection → Palpation → Auscultation) → Peripheral signs
1. GENERAL INSPECTION
Look for signs from the end of the bed:
Facies & habitus:
- Malar flush (mitral stenosis)
- Pallor (anaemia, low output states)
- Central cyanosis (check tongue and lips — congenital heart disease, Eisenmenger's)
- Peripheral cyanosis (fingers/toes — low output, cold)
- Marfan's syndrome (tall, arachnodactyly, high-arched palate — aortic root disease)
- Turner's syndrome (coarctation of aorta)
- Down's syndrome (ASD, VSD, AV canal defects)
Signs of distress: dyspnoea at rest, orthopnoea (pillows), cachexia (chronic heart failure)
2. HANDS
| Sign | Association |
|---|---|
| Clubbing | Cyanotic congenital heart disease, infective endocarditis |
| Splinter haemorrhages | Infective endocarditis (also trauma) |
| Osler's nodes | Painful, tender nodules on fingertips — infective endocarditis |
| Janeway lesions | Painless haemorrhagic macules on palms — infective endocarditis |
| Koilonychia | Iron deficiency → high-output cardiac failure |
| Peripheral cyanosis / pallor | Poor perfusion |
| Tendon xanthomata | Hypercholesterolaemia → IHD |
Capillary refill time: Normal <2 seconds.
3. RADIAL PULSE
Assess simultaneously at both wrists (radio-radial delay → coarctation of aorta, aortic dissection, subclavian stenosis).
Rate
- Normal: 60–100 bpm
- Bradycardia <60, tachycardia >100
Rhythm
- Regular — sinus rhythm
- Irregularly irregular — atrial fibrillation
- Regularly irregular — ectopics, 2nd degree AV block
Character (best assessed at carotid)
| Pulse | Description | Cause |
|---|---|---|
| Normal | Smooth upstroke, sustained peak | — |
| Slow-rising (pulsus parvus et tardus) | Weak, delayed upstroke | Aortic stenosis |
| Collapsing / water-hammer | Rapid upstroke, quick collapse | Aortic regurgitation |
| Bisferiens | Double-peaked in systole | Severe AR + AS combined |
| Pulsus alternans | Alternating strong and weak beats | Severe LV dysfunction |
| Pulsus paradoxus | Exaggerated fall in systolic BP (>10 mmHg) during inspiration | Cardiac tamponade, severe asthma |
| Pulsus bigeminus | Alternating normal + ectopic beats | Bigeminy |
Volume: Full, normal, or low (reduced → poor output, dehydration, AS)
4. BLOOD PRESSURE
- Measure in both arms (difference >20 mmHg → aortic dissection, subclavian stenosis, coarctation)
- Pulse pressure = systolic − diastolic
- Wide (>60 mmHg): AR, PDA, hyperthyroidism, anaemia, fever
- Narrow (<25 mmHg): AS, cardiac tamponade, severe heart failure
Postural BP: Drop >20 mmHg systolic or >10 mmHg diastolic on standing = orthostatic hypotension
5. JUGULAR VENOUS PRESSURE (JVP)

Technique
- Patient at 30–45° with head slightly rotated to the left
- Use the internal jugular vein (preferred; not valved, directly in line with RA)
- Measure vertical height of pulsation above the sternal angle (angle of Louis)
- Normal: <4.5 cm above sternal angle at 45°
- Pulsations above the clavicle in the sitting position are clearly abnormal (clavicle-to-RA distance ≥10 cm)
JVP vs Carotid Pulse — How to Distinguish
| Feature | JVP | Carotid |
|---|---|---|
| Waveform | Biphasic (two peaks in sinus rhythm) | Monophasic |
| Palpable | Not easily palpable | Easily palpable |
| Obliterable | Obliterated by gentle pressure | Not obliterated |
| Changes with posture | Yes — falls with sitting up | No |
| Changes with inspiration | Falls in inspiration (normally) | No change |
The JVP Waveform
| Component | Timing | Represents |
|---|---|---|
| a wave | Just after P wave, before S1 | Right atrial presystolic contraction |
| c wave | After a wave | Tricuspid valve pushed into RA during early ventricular systole |
| x descent | After a/c waves | Fall in RA pressure after tricuspid opening |
| v wave | During ventricular systole | Atrial filling (venous return against closed tricuspid) |
| y descent | After v wave | Fall in RA pressure as tricuspid opens and RV fills |
Abnormal JVP Waveforms
| Abnormality | Cause |
|---|---|
| Elevated JVP (raised all components) | Right heart failure, tricuspid stenosis, cardiac tamponade, SVC obstruction, fluid overload |
| Giant a wave | Tricuspid stenosis, pulmonary hypertension, RV hypertrophy (reduced RV compliance) |
| Cannon a wave | AV dissociation (RA contracts against closed tricuspid) — confirms ventricular tachycardia |
| Absent a wave | Atrial fibrillation |
| Giant v wave | Tricuspid regurgitation (ventricularnised waveform, steep y descent) |
| Prominent x descent | Cardiac tamponade, constrictive pericarditis |
| Prominent y descent | Constrictive pericarditis, severe TR |
| Kussmaul's sign | JVP rises with inspiration (opposite of normal) — constrictive pericarditis, RV infarct |
| Abdominojugular reflux | Sustained JVP rise >3 cm with abdominal pressure × 10 sec — right heart failure, volume overload |
6. FACE & NECK
- Eyes: corneal arcus (hypercholesterolaemia), xanthelasma (hyperlipidaemia), conjunctival pallor (anaemia)
- Mouth: central cyanosis (tongue), high-arched palate (Marfan's)
- Carotid pulse: character and volume (slow-rising = AS; collapsing = AR)
- Carotid bruits: auscultate over carotids (atherosclerosis, radiation of AS)
7. PRECORDIUM
Inspection
- Chest shape: pectus excavatum, pectus carinatum, kyphoscoliosis (may displace heart, cause murmurs)
- Visible apex beat: normally in 5th ICS, mid-clavicular line
- Scars: midline sternotomy (CABG, valve replacement), left lateral thoracotomy (mitral valvotomy, PDA ligation), pacemaker/ICD pocket (left infraclavicular)
- Prominent pulsations: left parasternal heave, visible apex
Palpation
Apex beat:
- Normally: 5th ICS, mid-clavicular line
- Assess: position, character, and area
| Apex Character | Description | Cause |
|---|---|---|
| Heaving / sustained / pressure-loaded | Forceful, sustained, not displaced | Aortic stenosis, hypertension (LVH) |
| Thrusting / hyperdynamic / volume-loaded | Forceful, may be displaced | Aortic or mitral regurgitation |
| Displaced laterally ± inferiorly | Beyond MCL | LV dilatation (DCM, severe MR, AR) |
| Tapping | Palpable S1 | Mitral stenosis |
| Double impulse | Two pulsations | HOCM, LV aneurysm |
| Impalpable | Obesity, COPD, effusion, dextrocardia | — |
Parasternal heave (left hand over left sternal edge):
- Sustained left parasternal lift → RV hypertrophy / dilatation (pulmonary hypertension, pulmonary stenosis, ASD)
Thrills (palpable murmurs — indicate grade ≥4/6):
- Systolic thrill at aortic area → AS
- Systolic thrill at LSE → VSD, HOCM
- Diastolic thrill at apex → MS
P2 palpability: Palpable P2 at left upper sternal edge → pulmonary hypertension
8. AUSCULTATION
Technique
- Diaphragm: high-frequency sounds (S1, S2, AR murmur, pericardial rub)
- Bell: low-frequency sounds (S3, S4, MS rumble) — use with light pressure
Auscultatory Areas
| Area | Location | Best Hears |
|---|---|---|
| Aortic | 2nd ICS, right sternal edge | AS, AR |
| Pulmonary | 2nd ICS, left sternal edge | PS, pulmonary regurgitation, P2 |
| Tricuspid | Lower left sternal edge (4th/5th ICS) | TR, TS, VSD |
| Mitral (Apex) | 5th ICS, mid-clavicular line | MS, MR, S3, S4 |
Manoeuvres:
- Left lateral decubitus position + bell at apex → best for MS rumble and S3/S4
- Sitting forward, expiration → best for AR early diastolic murmur
- Standing → suppresses most murmurs; HOCM louder, MVP click moves earlier
- Squatting → most murmurs louder; HOCM softer, MVP click moves later
- Valsalva → HOCM louder (decreased preload)
Heart Sounds
S1 (Mitral + Tricuspid Closure)
| S1 Abnormality | Cause |
|---|---|
| Loud S1 | Mitral stenosis (if mobile valve), short PR interval, tachycardia |
| Soft S1 | Long PR interval (1st degree AV block), MR, calcified/immobile mitral valve, poor LV function |
| Variable S1 | AF, complete heart block (cannon a wave), ectopics |
S2 (Aortic + Pulmonary Closure)
- Physiological splitting of S2: heard in inspiration (A2 before P2); splitting widens in inspiration, narrows in expiration
- Wide fixed splitting: ASD (equalization of RA/LA pressures)
- Wide splitting with respiratory variation: RBBB, pulmonary stenosis (delayed P2), pulmonary hypertension with RV failure
- Reversed/paradoxical splitting: LBBB, AS, HOCM (delayed A2; splits on expiration, closes on inspiration)
- Loud A2: systemic hypertension
- Loud P2 (palpable): pulmonary hypertension
- Soft A2: severe AS
S3 (Ventricular Gallop)
- Low-pitched, heard at apex with bell, in early diastole (Ken-tuck-y)
- Physiological in children and young adults (<40 years)
- Pathological in adults → indicates LV failure, dilated cardiomyopathy, severe MR
S4 (Atrial Gallop)
- Low-pitched, heard just before S1 (Ten-nes-see)
- Due to atrial contraction into a stiff, non-compliant ventricle
- Causes: LVH (hypertension, AS, HOCM), acute MI, hypertrophic cardiomyopathy
- Never heard in AF (no atrial contraction)
Opening Snap (OS)
- High-pitched, early diastolic sound after S2
- Mitral stenosis (mobile, non-calcified valve)
- Short S2–OS interval → more severe MS (high LA pressure)
Ejection Click
- High-pitched early systolic click
- Aortic or pulmonary valve stenosis (bicuspid aortic valve, valvular PS)
- Pulmonary ejection click softens with inspiration (unique among right-sided sounds)
Mid-Systolic Click
- Mitral valve prolapse (MVP)
- Moves earlier with standing/Valsalva (reduced preload)
- Moves later with squatting/leg raising (increased preload)
Pericardial Friction Rub
- High-pitched, scratchy, three-component sound (systolic + early diastolic + presystolic)
- Heard best with patient sitting forward, in expiration
- Acute pericarditis, post-MI (Dressler's syndrome), uraemia
Murmurs
Grading (Levine Scale)
| Grade | Description |
|---|---|
| 1/6 | Very faint; heard only with concentration |
| 2/6 | Faint but immediately audible |
| 3/6 | Moderately loud; no thrill |
| 4/6 | Loud; thrill present |
| 5/6 | Very loud; thrill; heard with stethoscope edge |
| 6/6 | Audible without stethoscope |
Systolic Murmurs
| Murmur | Timing | Location | Radiation | Quality | Key Features |
|---|---|---|---|---|---|
| Aortic Stenosis | Ejection systolic (ESM) | Aortic area | Carotids | Harsh, crescendo-decrescendo | Slow-rising pulse, soft A2, S4; radiates to carotids |
| Mitral Regurgitation | Pansystolic | Apex | Axilla | Soft, blowing | Displaced apex, soft S1, S3 |
| Tricuspid Regurgitation | Pansystolic | Lower LSE | No radiation | Blowing | Louder in inspiration (Carvallo's sign), elevated JVP with giant v wave |
| VSD | Pansystolic | Lower LSE | Across precordium | Harsh | Thrill common |
| HOCM | Ejection systolic | LSE/Apex | — | Harsh | Louder with Valsalva/standing; softer with squatting/leg raise |
| Pulmonary Stenosis | Ejection systolic | Pulmonary area | — | Harsh | Ejection click, wide P2 splitting |
| MVP | Late systolic | Apex | — | — | Preceded by mid-systolic click |
Diastolic Murmurs (always pathological)
| Murmur | Timing | Location | Quality | Key Features |
|---|---|---|---|---|
| Aortic Regurgitation | Early diastolic (decrescendo) | LSE (sitting forward, expiration) | Soft, high-pitched, blowing | Collapsing pulse, wide pulse pressure |
| Mitral Stenosis | Mid-diastolic rumble | Apex (LLD, bell) | Low-pitched, rumbling | Loud S1, opening snap; presystolic accentuation in sinus rhythm |
| Pulmonary Regurgitation | Early diastolic | Pulmonary area | Blowing | Graham Steell murmur in pulmonary HTN |
| Tricuspid Stenosis | Mid-diastolic | Lower LSE | Low-pitched | Rare; louder in inspiration |
Continuous Murmurs
- PDA: continuous "machinery" murmur, upper LSE
- AV fistula, coarctation collaterals
9. PERIPHERAL EXAMINATION
- Sacral oedema: pitting, in bedridden patients (right heart failure)
- Ankle/leg oedema: bilateral pitting → right heart failure, hypoalbuminaemia; unilateral → DVT, lymphoedema
- Hepatomegaly: tender, pulsatile in TR; congestive hepatomegaly in RHF
- Splenomegaly: infective endocarditis
- Ascites: severe right heart failure, constrictive pericarditis
- Lung bases: fine end-inspiratory crepitations → pulmonary oedema (LHF)
10. CLOSING THE EXAMINATION
State you would like to:
- Check temperature chart, urine output
- Review ECG, chest X-ray, echocardiogram
- Measure oxygen saturation
- Fundoscopy (hypertensive/diabetic changes, Roth spots in endocarditis)
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed., Ch. 246 — Cardiovascular Examination
- Fuster & Hurst's The Heart, 15th ed. — Clinical Cardiovascular Examination
- Goldman-Cecil Medicine — Physical Examination for Detection of Cardiovascular Disease
Explain with image
Asking for Preferences
Searching Images
cardiovascular examination peripheral signs hands clubbing splinter haemorrhages
Searching Images
precordial palpation apex beat auscultation areas heart sounds murmurs
Searching Images
heart murmurs aortic stenosis mitral regurgitation pulse character collapsing water hammer
Finding Sources
Finding Sources
Loading Image
Loading Image
Loading Image
Here is the full CVS examination explained with images, section by section:
CVS Examination — Illustrated Guide
1. GENERAL INSPECTION & HANDS
Start from the end of the bed — look for dyspnoea, cyanosis, cachexia, abnormal habitus (Marfan's, Down's).
Hands — key signs:
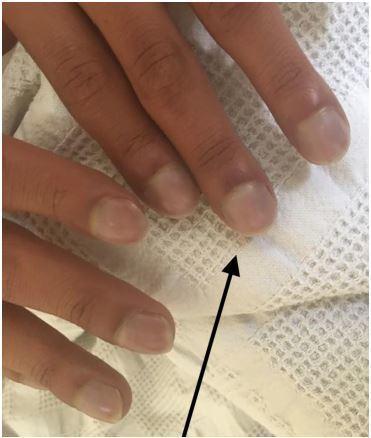

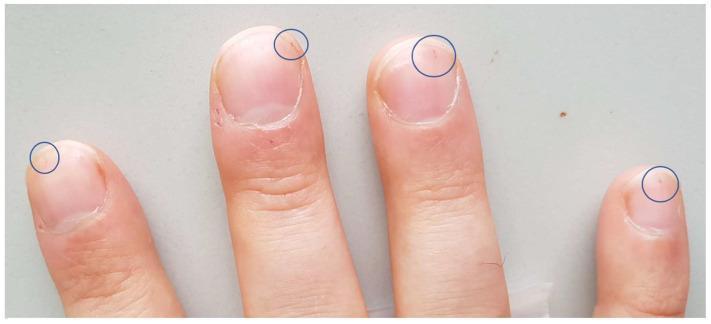
| Sign | Significance |
|---|---|
| Clubbing | Cyanotic CHD, IE |
| Splinter haemorrhages | Infective endocarditis |
| Osler's nodes | Painful fingertip nodules — IE |
| Janeway lesions | Painless palmar macules — IE |
| Xanthomata | Hypercholesterolaemia → IHD |
| Peripheral cyanosis | Low output, poor perfusion |
2. PULSE — Rate, Rhythm, Character
Assess radial pulse for rate and rhythm. Assess character at the carotid (best site).
| Pulse Type | Feel | Cause |
|---|---|---|
| Normal | Smooth upstroke, sustained peak | — |
| Slow-rising (pulsus parvus et tardus) | Weak, delayed, plateau | Aortic stenosis |
| Collapsing (water-hammer) | Rapid upstroke, sudden collapse | Aortic regurgitation |
| Pulsus alternans | Alternating strong/weak beats | Severe LV dysfunction |
| Pulsus paradoxus | Systolic BP falls >10 mmHg on inspiration | Cardiac tamponade |
| Bisferiens | Double peak in systole | Severe AR ± AS, HOCM |
Radio-radial delay (different pulses in each wrist) → coarctation of aorta / aortic dissection Radio-femoral delay → coarctation of aorta
3. BLOOD PRESSURE
- Measure both arms — difference >20 mmHg → aortic dissection, subclavian stenosis
- Wide pulse pressure (>60 mmHg): AR, PDA, thyrotoxicosis, anaemia
- Narrow pulse pressure (<25 mmHg): severe AS, tamponade, heart failure
4. JUGULAR VENOUS PRESSURE (JVP)
Technique — Patient positioning
- Normal: <4.5 cm above sternal angle at 45°
- Pulsation above the clavicle in sitting = always elevated (clavicle–RA distance ≥10 cm)
- Use internal jugular vein (preferred — not valved, directly communicates with RA)
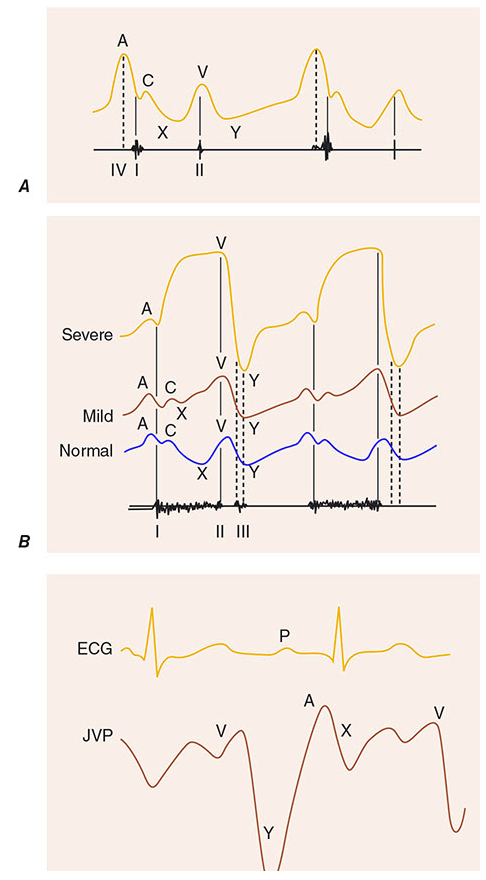
The JVP Waveform
Panel A: Normal JVP waveform showing a, c, x, v, y components. Panel B: Progressive changes in tricuspid regurgitation — giant v wave increasingly dominates and merges with c wave. Panel C: Timing of JVP waveform relative to the ECG — a wave follows the P wave; v wave occurs during ventricular systole.
| Component | Timing | Represents |
|---|---|---|
| a wave | After P wave, before S1 | RA presystolic contraction |
| c wave | Early systole | Tricuspid pushed into RA |
| x descent | After a/c | RA pressure fall |
| v wave | During ventricular systole | Passive atrial filling |
| y descent | After v | Tricuspid opens, RV fills |
Abnormal JVP — Clinical Correlations
| Abnormality | Cause |
|---|---|
| Elevated JVP (all components raised) | RHF, fluid overload, tamponade, SVC obstruction |
| Giant a wave | TS, pulmonary HTN, RVH |
| Cannon a wave | AV dissociation → confirms VT |
| Absent a wave | Atrial fibrillation |
| Giant v wave | Tricuspid regurgitation |
| Prominent x descent | Cardiac tamponade |
| Prominent y descent | Constrictive pericarditis, severe TR |
| Kussmaul's sign | JVP ↑ on inspiration — constrictive pericarditis, RV infarct |
| Abdominojugular reflux | JVP rises >3 cm with sustained abdominal pressure — RHF |
5. PRECORDIUM
Auscultation Areas

| Area | Location | Best hears |
|---|---|---|
| Aortic | 2nd ICS, right sternal edge | AS, AR |
| Pulmonary | 2nd ICS, left sternal edge | PS, P2, PR |
| Tricuspid | 4th–5th ICS, left sternal edge | TR, TS, VSD |
| Mitral (Apex) | 5th ICS, mid-clavicular line | MS, MR, S3, S4 |
Apex Beat Character
| Character | Feel | Cause |
|---|---|---|
| Heaving / pressure-loaded | Sustained, not displaced | AS, hypertension (LVH) |
| Thrusting / volume-loaded | Hyperdynamic, may be displaced | AR, MR |
| Displaced laterally | Beyond MCL | LV dilatation (DCM, severe MR/AR) |
| Tapping | Palpable S1 | Mitral stenosis |
| Double impulse | Two pulsations | HOCM, LV aneurysm |
Left parasternal heave → RV hypertrophy (pulmonary hypertension, ASD, PS)
6. HEART SOUNDS
S1 & S2 — Normal and Abnormal
| Sound | Normal | Abnormal | Cause |
|---|---|---|---|
| S1 | Closure of mitral + tricuspid | Loud S1 | MS (mobile valve), short PR, tachycardia |
| Soft S1 | Long PR (1° HB), calcified MV, poor LV function | ||
| Variable S1 | AF, complete heart block | ||
| S2 | Closure of aortic (A2) + pulmonary (P2) | Wide fixed split | ASD |
| Wide variable split | RBBB, pulmonary stenosis | ||
| Physiological split widens in inspiration | Paradoxical split (widens in expiration) | LBBB, severe AS | |
| Loud P2 (palpable) | Pulmonary hypertension |
S3 and S4
| Extra Sound | Timing | Mnemonic | Significance |
|---|---|---|---|
| S3 (ventricular gallop) | Early diastole (after S2) | Ken-tuck-Y | Pathological in adults → LV failure, DCM, severe MR |
| S4 (atrial gallop) | Late diastole (before S1) | TEN-nes-see | LVH (HTN, AS, HOCM), acute MI; absent in AF |
Use the bell with light pressure at the apex for S3 and S4. Position patient in left lateral decubitus.
Opening Snap, Clicks, Rub
| Sound | Timing | Cause |
|---|---|---|
| Opening snap (high-pitched) | Early diastole after S2 | MS (mobile valve); shorter S2–OS interval = more severe |
| Ejection click (early systolic) | Immediately after S1 | AS (bicuspid valve), PS |
| Mid-systolic click | Mid-systole | MVP — moves earlier with standing/Valsalva |
| Pericardial rub | Scratchy, 3-component | Acute pericarditis, Dressler's, uraemia |
7. MURMURS
Radiation Patterns — AS and MR
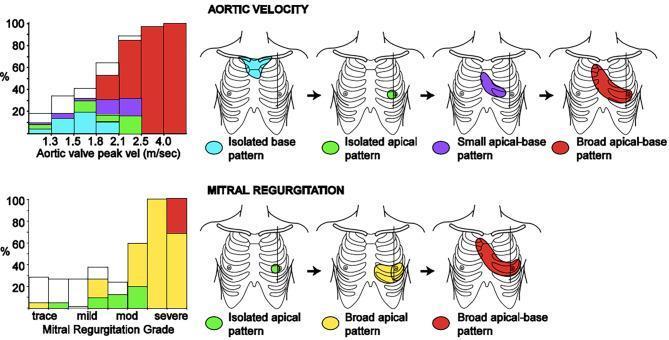
AS murmur: begins isolated at the base, spreads to apical-base distribution as severity increases (radiates to carotids). MR murmur: begins isolated at apex, spreads broadly toward the axilla and base as severity increases.
Systolic Murmurs
| Murmur | Type | Location | Radiation | Key Clues |
|---|---|---|---|---|
| Aortic Stenosis | Ejection systolic (ESM) | Aortic area | Carotids | Slow-rising pulse, soft A2, S4; loudest in expiration |
| Mitral Regurgitation | Pansystolic | Apex | Axilla | Displaced apex, soft S1, S3; loudest in expiration/left lateral |
| Tricuspid Regurgitation | Pansystolic | Lower LSE | — | Louder in inspiration (Carvallo's sign); giant v wave in JVP |
| VSD | Pansystolic | Lower LSE | All over precordium | Loud, thrill common |
| HOCM | ESM | LSE/Apex | — | Louder with Valsalva/standing; softer with squatting |
| Pulmonary Stenosis | ESM | Pulmonary area | — | Ejection click; wide split S2 |
| MVP | Late systolic | Apex | — | Preceded by mid-systolic click |
Diastolic Murmurs (always pathological)
| Murmur | Timing | Location | Key Clues |
|---|---|---|---|
| Aortic Regurgitation | Early diastolic decrescendo | LSE (sitting forward, expiration) | Collapsing pulse, wide PP, displaced apex |
| Mitral Stenosis | Mid-diastolic rumble | Apex (bell, LLD, expiration) | Loud S1, OS, tapping apex; presystolic accentuation in SR |
| Pulmonary Regurgitation | Early diastolic | Pulmonary area | Graham Steell murmur in pulmonary HTN |
Dynamic Manoeuvres
| Manoeuvre | Effect on Preload | HOCM | AS/MR/AR | MVP Click |
|---|---|---|---|---|
| Valsalva / Standing | Decreases | Louder | Softer | Moves earlier |
| Squatting / Leg raise | Increases | Softer | Louder | Moves later |
| Inspiration | Increases RV filling | — | Right-sided murmurs louder | — |
8. PERIPHERAL SIGNS (Complete the Exam)
| Finding | Significance |
|---|---|
| Bilateral ankle/sacral pitting oedema | Right heart failure |
| Tender hepatomegaly | Congestive hepatomegaly (RHF) |
| Pulsatile liver | Tricuspid regurgitation |
| Fine basal crepitations | Pulmonary oedema (LHF) |
| Splenomegaly | Infective endocarditis |
| Xanthelasma / corneal arcus | Hypercholesterolaemia |
| Roth spots (fundoscopy) | Infective endocarditis |
Summary — "What to Say at the End"
"To complete my examination I would like to:
- Check the blood pressure in both arms and lying/standing
- Review the ECG, chest X-ray, and echocardiogram
- Measure oxygen saturation
- Perform fundoscopy (HTN, diabetic, Roth spots)
- Check urine dipstick (haematuria in IE, proteinuria in HTN)"
Sources: Harrison's Principles of Internal Medicine 22nd ed. — Cardiovascular Examination | Fuster & Hurst's The Heart, 15th ed.
This is a shared conversation. Sign in to Orris to start your own chat.