Teach me unipolar vs bipolar disorder and explain all the signs and symptoms
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bipolar disorder" AND "unipolar depression" AND diagnosis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have comprehensive content. Let me compile the full, structured answer.
Unipolar vs. Bipolar Disorder: A Complete Guide
1. The Core Distinction
| Unipolar (Major Depressive Disorder) | Bipolar Disorder | |
|---|---|---|
| Mood episodes | Depression only | Depression + mania (or hypomania) |
| 12-month prevalence | ~7% | ~0.6% |
| Sex ratio | 1.5–2× more common in females | Slightly higher in males |
| Age of onset | Any age; peak in adulthood | Late adolescence / early adulthood |
| Heritability | ~40% genetic | ~50% genetic (stronger genetic contribution) |
| Suicide lifetime risk | ~20% if untreated | Higher (especially in mixed/depressive phases) |
The defining feature: unipolar disorder means episodes travel in only one direction — down. Bipolar disorder means the mood can swing up into mania or hypomania as well.
2. Unipolar Depression (Major Depressive Disorder)
Definition
One or more episodes of major depressive syndrome with no history of mania or hypomania.
DSM-5 Diagnostic Criteria
At least 5 of the following 9 symptoms for ≥2 consecutive weeks, with at least one symptom being either depressed mood or anhedonia:
Mnemonic: SIG: E CAPS (prescribe energy capsules)
| Letter | Symptom |
|---|---|
| S | Sleep change (insomnia or hypersomnia) |
| I | Interests decreased (anhedonia) |
| G | Guilt / worthlessness |
| E | Energy decreased (fatigue/anergia) |
| C | Concentration decreased / indecisiveness |
| A | Appetite/weight change (↑ or ↓) |
| P | Psychomotor agitation or retardation |
| S | Suicidal ideation / thoughts of death |
Plus the anchor symptom: depressed mood (or in children/adolescents: irritable mood)
Full Symptom Breakdown by Domain
🔴 Emotional / Mood
- Persistent sadness, tearfulness
- Irritability (especially prominent in children, adolescents, and the elderly)
- Anxiety (very common comorbid feature)
- Anhedonia — loss of interest or pleasure in previously enjoyed activities
- Feeling "empty" or hopeless
🔵 Ideational (Thought Content)
- Worthlessness / lowered self-esteem
- Excessive or inappropriate guilt
- Hopelessness and nihilism
- Helplessness
- Thoughts of death, dying, or suicide (ranging from passive ideation to active plans)
- Ruminative thinking — dwelling on negative themes
🟡 Somatic / Neurovegetative
- Change in appetite (anorexia or increased appetite)
- Change in sleep (early morning awakening is classic; also hypersomnia)
- Fatigue and loss of energy disproportionate to activity
- Decreased libido
- Psychomotor retardation or agitation (observable by others)
- Diurnal variation — symptoms typically worst in the morning
🟠 Cognitive
- Difficulty concentrating, slowed thinking
- Indecisiveness
- In severe cases: psychotic features — mood-congruent delusions (guilt, punishment, unworthiness) or hallucinations (usually a single derogatory voice)
- In children: school failure, withdrawal from peers, somatic complaints
Subtypes
- With Melancholic Features: profound anhedonia, early morning awakening, marked weight loss, severe guilt ("endogenous depression") — associated with autonomic/endocrine changes
- With Psychotic Features: mood-congruent delusions/hallucinations — severe form, poor prognosis
- With Atypical Features: mood reactivity to positive events, hypersomnia, hyperphagia, leaden paralysis, rejection sensitivity
- Persistent Depressive Disorder (Dysthymia): depressed mood most days for ≥2 years (1 year in children), less severe but chronic
3. Bipolar Disorder
Definition & Types
Characterized by recurrent manic (or hypomanic) episodes, usually interspersed with depressive episodes.
| Type | Episodes Required |
|---|---|
| Bipolar I | ≥1 manic episode (depressive episodes common but not required) |
| Bipolar II | ≥1 hypomanic episode + ≥1 major depressive episode; no full manic episode |
| Cyclothymia | Hypomanic + subthreshold depressive symptoms cycling for ≥2 years |
Manic Episode — DSM-5 Diagnostic Criteria
A distinct period of abnormally, persistently elevated/expansive or irritable mood + increased goal-directed activity/energy, lasting ≥1 week (most of the day, nearly every day), AND 3 or more of the following (4 or more if mood is only irritable):
Mnemonic: DIG FAST
| Symptom | Detail |
|---|---|
| D | Distractibility |
| I | Irresponsibility / Impulsivity (risky activities) |
| G | Grandiosity (inflated self-esteem) |
| F | Flight of ideas / racing thoughts |
| A | Activity increase (goal-directed) / psychomotor Agitation |
| S | Sleep decreased need (not insomnia — they feel rested on 2–3 hrs) |
| T | Talkativeness (pressured speech) |
Full Manic Symptom Breakdown by Domain
🔴 Emotional / Mood
- Euphoria — abnormally elevated, expansive mood
- Irritability — especially when thwarted
- Labile affect — mood shifts rapidly
🔵 Ideational (Thought Content)
- Grandiosity — inflated self-esteem, may believe they have special powers, connections, or identity
- Flight of ideas — rapid jumps from thought to thought
- Racing thoughts — subjective experience of thinking too fast
- In severe cases: psychotic features — delusions (often grandiose or persecutory), hallucinations, loose associations, thought disorganization
🟡 Somatic / Neurovegetative
- Increased energy — boundless, goal-directed activity
- Decreased need for sleep (not insomnia — patients do not feel tired)
- Psychomotor agitation
- Distractibility (easily pulled by irrelevant stimuli)
🟠 Behavioral (the "painful consequences")
- Pressured speech — fast, difficult to interrupt
- Spending sprees, financial recklessness
- Sexual indiscretion
- Gambling
- Reckless driving
- Grandiose business schemes
- Poor judgment leading to lasting adverse consequences
Hypomanic Episode (Bipolar II)
Same qualitative symptoms as mania, but:
- Duration ≥4 days (not ≥7)
- Not severe enough to cause marked functional impairment
- No psychotic features
- No hospitalization required
- Observable by others but the patient may see it as their "best self"
Depressive Phase of Bipolar
Identical in presentation to unipolar MDD symptoms — which is why bipolar disorder is frequently misdiagnosed as unipolar depression when patients first present in the depressed phase. Key clues that depression may be bipolar:
- Family history of bipolar
- Early onset (teens/early 20s)
- Hypersomnia and hyperphagia (atypical features)
- Psychomotor retardation
- Psychotic features
- Prior antidepressant-induced hypomania
- Rapid cycling history
4. Side-by-Side Comparison of Symptom Domains
| Domain | Unipolar Depression | Mania (Bipolar) |
|---|---|---|
| Mood | Sad, tearful, empty | Euphoric, expansive, or irritable |
| Energy | ↓ Fatigue, anergia | ↑ Boundless energy |
| Sleep | Insomnia or hypersomnia | Decreased need for sleep |
| Thought speed | Slowed, ruminative | Racing thoughts, flight of ideas |
| Speech | Slow, quiet | Pressured, rapid, loud |
| Self-esteem | Worthlessness, guilt | Grandiosity, inflated ego |
| Activity | Psychomotor retardation | Goal-directed hyperactivity |
| Appetite/Weight | ↑ or ↓ | Often ↓ (too busy to eat) |
| Judgment | Often intact (except in psychotic subtype) | Markedly impaired |
| Psychosis | Mood-congruent (guilt, punishment themes) | Mood-congruent or mood-incongruent |
| Suicidality | Passive or active | Often during depressed or mixed phases |
5. Pathobiology (Why They Differ)
| Unipolar | Bipolar | |
|---|---|---|
| Heritability | ~40% | ~50% |
| Genetics | Polygenic; mostly unknown loci | Polygenic; stronger genetic load; some specific loci in rare families |
| Neuroimaging | Smaller hippocampal volumes; frontal-striatal hypoactivity | Increased ventricular-brain ratio; frontostriatal dysregulation |
| Neurochemistry | Noradrenergic/serotonergic dysregulation; HPA axis hyperactivity | Circadian rhythm dysregulation prominent — phase advance triggers mania |
| Cognitive model | Negative cognitive triad (self, world, future) | Oscillating extremes of self-evaluation |
| Precipitants | Exit life events (deaths, loss, separations) | Sleep deprivation, psychosocial stress, substances |
6. The Depression Management Pathway
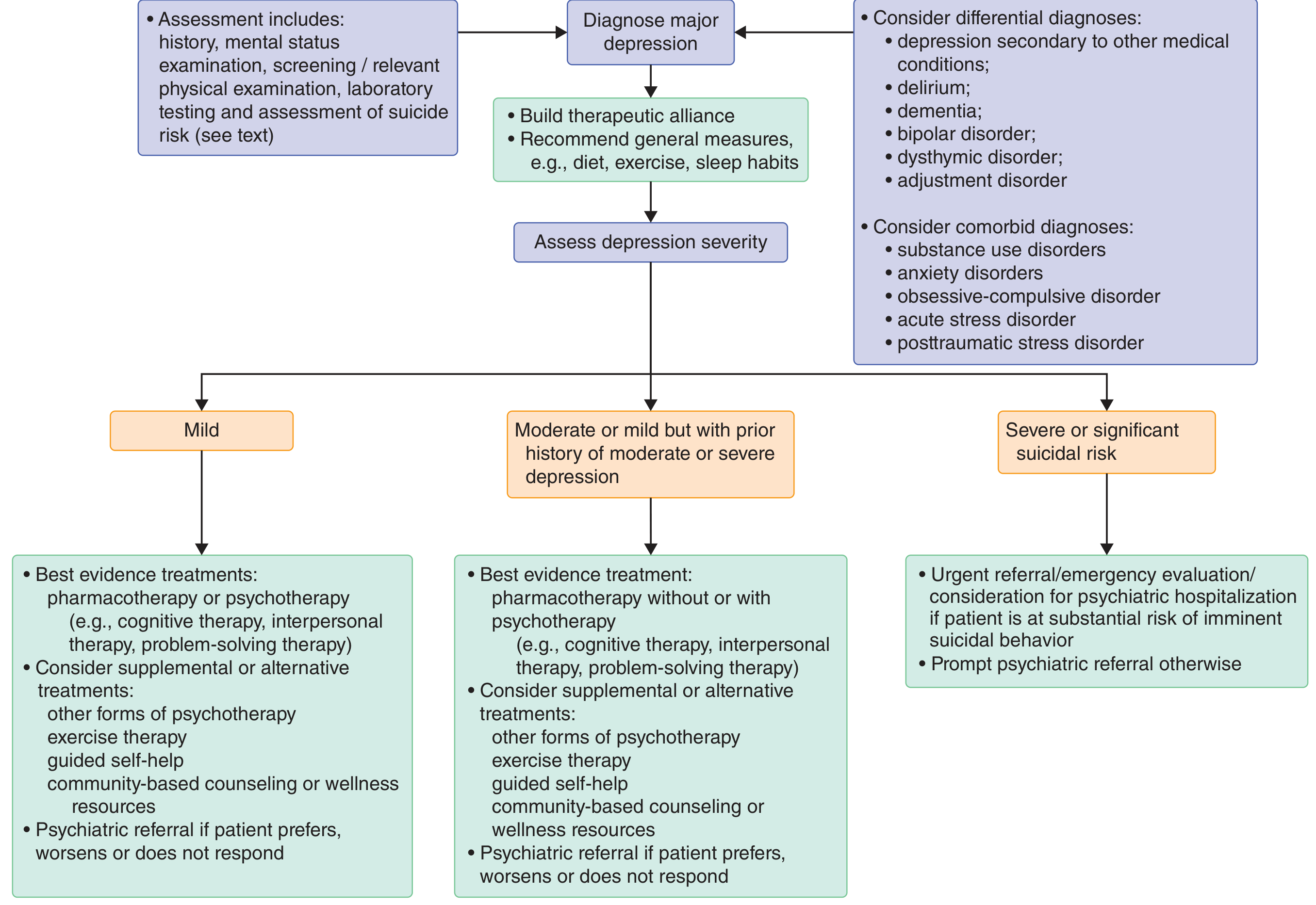
Goldman-Cecil Medicine — Depression severity-based treatment algorithm
Key treatment principle: In unipolar depression, antidepressants are first-line. In bipolar disorder, antidepressants alone can precipitate mania — mood stabilizers (lithium, valproic acid) or atypical antipsychotics are the foundation of treatment.
7. Quick Clinical Pearls
- NEVER start antidepressant monotherapy before ruling out bipolar — it can trigger a manic switch or rapid cycling
- The PHQ-2 screen (anhedonia + depressed mood, scored 0–3 each) — a score ≥3 gives 75% probability of depressive disorder
- Bipolar patients typically first seek care during depressive episodes, making bipolar II especially easy to miss
- Circadian rhythm disruption (jet lag, shift work, sleep deprivation) is a powerful mania trigger in bipolar patients
- Lifetime suicide risk: ~20% for untreated unipolar depression; bipolar carries even higher risk
- Worldwide, <25% of depressed individuals receive adequate treatment
Recent Evidence Note
A 2025 meta-analysis (PMID 39978428) found that objective sleep markers can help differentiate unipolar from bipolar depression — bipolar depression shows more pronounced circadian disruption and different polysomnographic patterns. Digital phenotyping (smartphone-based activity and speech patterns) is also emerging as a discrimination tool (PMID 40408762).
Sources: Goldman-Cecil Medicine, 26th ed. | Kaplan & Sadock's Synopsis of Psychiatry | Kaplan & Sadock's Comprehensive Textbook of Psychiatry | Neuroscience: Exploring the Brain, 5th ed. | Textbook of Family Medicine, 9th ed. — via the medical textbook library
This is a shared conversation. Sign in to Orris to start your own chat.