Respiratory failure detail clinical managemet
Reading File
Finding Sources
Searching PubMed
"respiratory failure" AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full detailed clinical management answer.
Respiratory Failure: Detailed Clinical Management
Classification of respiratory failure - Fishman's Pulmonary Diseases and Disorders
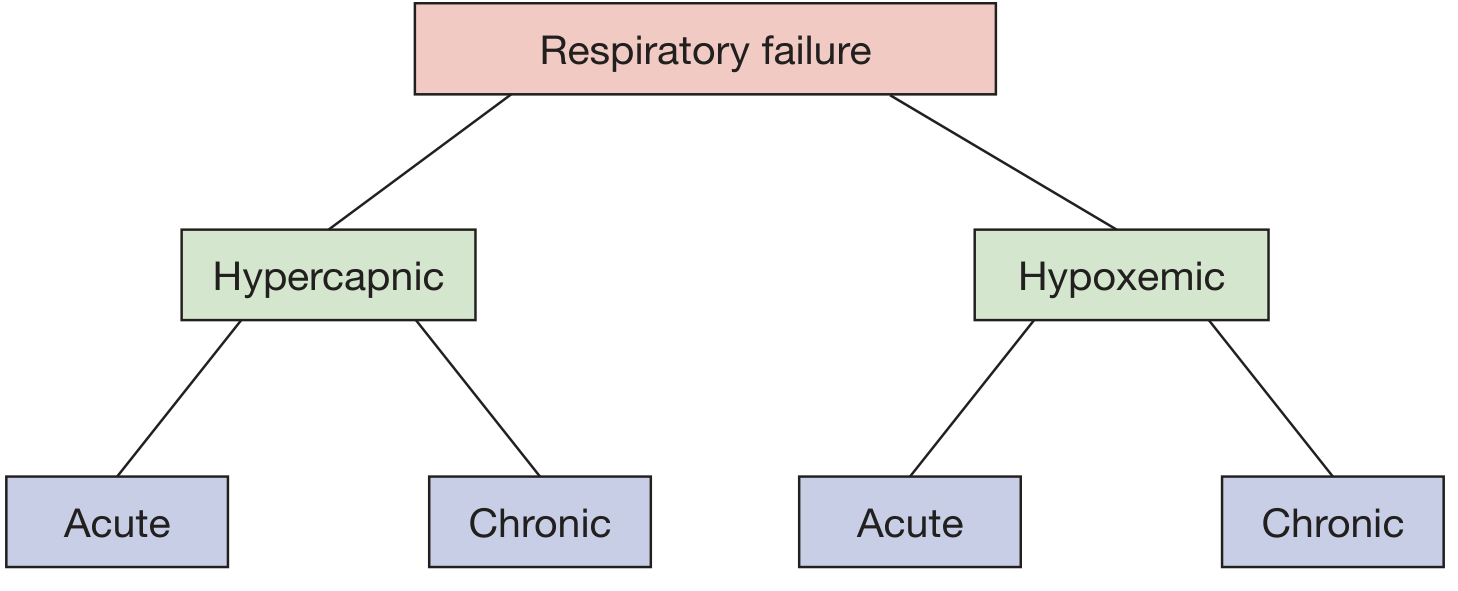
1. Definition and Classification
Respiratory failure is defined as the inability of the respiratory system to maintain adequate gas exchange to meet the metabolic demands of the body. Clinically it is identified by arterial blood gas values:
| Type | Definition | ABG Criteria |
|---|---|---|
| Hypercapnic (Type 2 / "Ventilatory") | Failure of CO2 elimination | PaCO2 >45 mmHg |
| Hypoxemic (Type 1 / "Oxygenation") | Failure of oxygenation | PaO2 <60 mmHg |
| Acute | Rapid onset (minutes to hours) | Acidemia (pH <7.30) in hypercapnic type |
| Chronic | Develops over days or longer | Renal bicarbonate compensation present |
Acute hypercapnic respiratory failure is specifically characterized by PaCO2 >45 mmHg with accompanying acidemia (pH <7.30). In patients with pre-existing chronic hypercapnia (e.g., COPD), a long-standing elevated PaCO2 causes renal compensation and elevated bicarbonate, so a superimposed acute rise has a less dramatic pH effect. - Fishman's Pulmonary Diseases and Disorders, p. 4236
2. Severity Classification (COPD Model - Applicable Broadly)
| Grade | Clinical Features |
|---|---|
| No respiratory failure | RR 20-30/min, normal WOB, baseline mentation, mild hypoxemia responsive to nasal cannula O2, no hypercapnia |
| Acute respiratory failure | RR >30/min, accessory muscle use, baseline mentation preserved, hypoxemia responsive to <35% FiO2, PaCO2 50-60 mmHg, pH >7.25 |
| Severe respiratory failure | Altered mental status, hypoxemia requiring >35% FiO2, PaCO2 >60 mmHg or pH ≤7.25 |
- Rosen's Emergency Medicine, Box 60.1
3. Pathophysiology and Causes
Mechanisms of Hypoxemia (Type 1)
- V/Q mismatch - commonest cause (pneumonia, pulmonary embolism, COPD, atelectasis)
- Intrapulmonary shunt - blood bypasses ventilated alveoli (ARDS, hepatopulmonary syndrome, cardiac shunt)
- Diffusion impairment - interstitial lung disease, emphysema
- Hypoventilation - raises alveolar PCO2, reduces PAO2
- Low inspired FiO2 - high altitude
Mechanisms of Hypercapnia (Type 2)
The Fishman's framework models this as ventilatory demand exceeding ventilatory supply:
Diminished Ventilatory Supply:
- Decreased respiratory muscle strength (fatigue, disuse atrophy, malnutrition, hypophosphatemia, hypokalemia)
- Decreased motor neuron function (Guillain-Barre syndrome, phrenic nerve injury, myasthenia gravis)
- Airflow limitation (bronchospasm, upper airway obstruction, secretions)
- Loss of lung volume (lung resection, large pleural effusion, tense abdomen)
Increased Ventilatory Demand:
- Increased dead space (V/Q mismatch, pulmonary embolism)
- Increased CO2 production (fever, sepsis, overfeeding, thyrotoxicosis)
Categories of Causes by System
| System | Examples |
|---|---|
| CNS | Opioid/sedative overdose, brainstem stroke, meningitis, trauma |
| Peripheral nerves | Guillain-Barre, critical illness polyneuropathy, phrenic nerve injury |
| Neuromuscular junction | Myasthenia gravis, botulism, organophosphate poisoning |
| Respiratory muscles | Fatigue, myopathy, malnutrition |
| Chest wall | Flail chest, kyphoscoliosis, obesity |
| Upper airway | Epiglottitis, foreign body, angioedema, obstructive sleep apnea |
| Lower airway | COPD exacerbation, asthma, bronchiectasis |
| Parenchyma | Pneumonia, ARDS, pulmonary fibrosis, pulmonary edema |
| Vascular | Massive pulmonary embolism, pulmonary hypertension |
4. Clinical Evaluation
History and Physical
- Presenting symptoms: dyspnea, orthopnea, cough, sputum, chest pain
- Onset and tempo (acute vs. chronic)
- Baseline functional status and prior pulmonary disease
- Signs: tachypnea, accessory muscle use, paradoxical breathing, cyanosis, altered mentation, diaphoresis, tripod positioning
- Dynamic hyperinflation in COPD: increased end-expiratory lung volume, alveolar overdistension, decreased compliance, elevated work of breathing, and respiratory muscle fatigue ultimately cause hypercapnia - Rosen's Emergency Medicine
Investigations
| Test | Purpose |
|---|---|
| ABG | Definitive - PaO2, PaCO2, pH, bicarbonate, A-a gradient |
| SpO2 continuous monitoring | Real-time oxygenation |
| CXR | Consolidation, pneumothorax, pulmonary edema, effusion |
| ECG | Right heart strain, arrhythmias |
| CBC, BMP, lactate | Infection, electrolytes, tissue perfusion |
| BNP/NT-proBNP | Distinguish cardiac from pulmonary cause |
| CT chest / CTPA | PE, parenchymal disease, ARDS |
| Echo (bedside) | Cardiac function, RV strain, pericardial effusion |
A-a gradient = PAO2 - PaO2 [PAO2 = (FiO2 × 713) - PaCO2/0.8]. A normal A-a gradient (< ~15 mmHg in young adults, up to 25 mmHg in elderly) with hypoxemia suggests hypoventilation. A raised A-a gradient indicates V/Q mismatch, shunt, or diffusion impairment.
5. Clinical Management
Step 1: Immediate Stabilization (First Minutes)
- Position: Head of bed 30-45°, sitting up to recruit lung bases
- Airway: Assess patency; suction secretions; jaw thrust/chin lift if needed; oral/nasal airway as bridge
- Oxygen: Start supplemental oxygen immediately (see targets below)
- IV access, monitoring: SpO2, ETCO2 if available, continuous ECG, BP
Step 2: Oxygen Therapy Targets
| Patient Group | SpO2 Target | Approach |
|---|---|---|
| Most patients | 94-98% | Titrate to avoid hyperoxia |
| COPD, chronic hypercapnia | 88-92% | Avoid high-flow O2 (risk of hypercapnic drive suppression) |
| Carbon monoxide poisoning | 100% | High-flow 100% O2 via NRM |
Oxygen delivery devices (escalating flow/FiO2):
- Nasal cannula: 1-6 L/min → FiO2 24-44%; for mild hypoxemia
- Simple face mask: 6-10 L/min → FiO2 35-55%
- Non-rebreather mask (NRM): 10-15 L/min → FiO2 60-90%
- High-Flow Nasal Cannula (HFNC): Up to 60 L/min, FiO2 up to 100% - see below
- NIV (BiPAP/CPAP) - see below
- Invasive mechanical ventilation - when above measures fail
Step 3: High-Flow Nasal Cannula (HFNC)
HFNC is the primary indicated support modality for acute hypoxemic respiratory failure, particularly from community- or hospital-acquired pneumonia. Meta-analyses advocate for HFNC especially with more severe hypoxemia - the key benefit is fewer patients require escalation to intubation and mechanical ventilation, reducing associated complications including death. - Murray & Nadel's Textbook of Respiratory Medicine
HFNC Benefits:
- Delivers heated, humidified gas at high flows (up to 60 L/min)
- Provides a small degree of PEEP (~0.5-1 cmH2O/10 L/min of flow)
- Washes nasopharyngeal dead space (reduces CO2 rebreathing)
- Reduces work of breathing
- Better tolerated than NIV face mask
Caution: HFNC is considered an aerosol-generating procedure. Use in negative-pressure isolation for patients with novel respiratory pathogens (COVID-19, TB, etc.).
ROX Index (SpO2/FiO2 ratio / RR): A score <2.85 at 2, 6, or 12 hours predicts HFNC failure and need for intubation.
Step 4: Non-Invasive Ventilation (NIV)
NIV uses positive pressure delivered via a mask (full-face, oronasal, or nasal) without endotracheal intubation.
Strongest indications (Level A evidence):
- COPD exacerbation with hypercapnia (pH <7.35, PaCO2 >45 mmHg) - reduces intubation rate, ICU mortality, and length of stay
- Acute cardiogenic pulmonary edema - CPAP reduces need for intubation
- Immunocompromised patients with acute hypoxemic RF (avoids complications of intubation)
- Neuromuscular disease with respiratory failure (BiPAP)
- Post-extubation in high-risk patients (COPD, cardiac failure)
Modes:
- CPAP: Constant positive pressure throughout respiratory cycle; best for cardiogenic pulmonary edema, OSA
- BiPAP (IPAP/EPAP): Separate inspiratory and expiratory pressures; best for COPD and neuromuscular failure
- Typical starting: IPAP 10-12 cmH2O, EPAP 4-5 cmH2O, titrate to response
- Target: RR decrease, SpO2 improvement, pH correction, relief of accessory muscle use
Absolute contraindications to NIV:
- Respiratory or cardiac arrest
- Uncooperative, agitated patient
- Unable to protect airway (swallowing, cough impairment)
- Excessive secretions not manageable
- Recent upper GI surgery or facial trauma
In cystic fibrosis patients, BiPAP has been used successfully as a bridge to lung transplant, improving oxygenation and reducing respiratory rate, with successful transition to home nocturnal use. - Fishman's Pulmonary Diseases and Disorders
Step 5: Endotracheal Intubation and Invasive Mechanical Ventilation
Indications for intubation:
- Failure or contraindication of NIV/HFNC
- GCS ≤8 or inability to protect airway
- Refractory hypoxemia (PaO2/FiO2 <100 despite maximal non-invasive support)
- Severe respiratory acidosis (pH <7.20)
- Hemodynamic instability / impending respiratory arrest
- Massive secretions or upper airway hemorrhage
- Post-cardiac arrest
Initial Ventilator Settings (general):
| Parameter | Setting | Rationale |
|---|---|---|
| Mode | Volume-controlled AC (ACVC) or PRVC | Guaranteed tidal volume delivery |
| Tidal Volume (VT) | 6 mL/kg ideal body weight (IBW) | Lung-protective (ARDSnet); prevents VILI |
| RR | 12-20/min | Adjust to patient need and PaCO2 target |
| FiO2 | Start at 1.0, then wean | Target PaO2 55-80 mmHg, SpO2 88-95% |
| PEEP | 5-8 cmH2O initial; higher in ARDS | Prevent alveolar derecruitment |
| I:E ratio | 1:2 (standard); 1:3-4 in obstructive disease | Allow full exhalation in COPD/asthma |
| Plateau pressure | Keep <30 cmH2O | Prevent barotrauma |
| Driving pressure | Keep <15 cmH2O (Plateau - PEEP) | Independent predictor of ARDS mortality |
Special Ventilator Strategies by Condition:
ARDS (Berlin Criteria: PaO2/FiO2 <300 with bilateral infiltrates, not fully explained by cardiac failure):
- Lung-protective ventilation: VT 6 mL/kg IBW, plateau pressure <30 cmH2O
- Higher PEEP strategy for moderate-severe ARDS (guided by PEEP/FiO2 tables)
- Prone positioning for 16 hours/day in severe ARDS (PaO2/FiO2 <150) - reduces mortality (PROSEVA trial)
- Neuromuscular blockade (cisatracurium 48h) for severe ARDS - controversial but used for ventilator dyssynchrony
- Inhaled nitric oxide (iNO) or inhaled prostacyclin as rescue for refractory hypoxemia
- Corticosteroids (methylprednisolone) - may be considered for non-resolving ARDS
- ECMO (venovenous VV-ECMO) as last resort for refractory ARDS when conventional therapy fails - see below
COPD Exacerbation:
- Permissive hypercapnia acceptable (pH >7.20)
- Prolonged expiratory time (low RR, short I-time, high flow rate)
- Avoid high PEEP (risk of dynamic hyperinflation)
- Set extrinsic PEEP at ~80% of measured auto-PEEP to reduce inspiratory triggering work
- Wean aggressively; daily spontaneous breathing trials (SBTs)
Asthma (Status Asthmaticus):
- Permissive hypercapnia (pH >7.20)
- Low RR (8-12/min), low minute ventilation to prevent air trapping
- High inspiratory flow to maximize expiratory time
- Monitor for pneumothorax
Opioid/CNS Depression:
- Naloxone 0.4 mg IV/IM/intranasal for opioid-induced respiratory failure (titrate to avoid precipitating acute withdrawal)
- Reversal agents for residual neuromuscular blockade (sugammadex for rocuronium/vecuronium; neostigmine + glycopyrrolate for older agents)
- Schwartz's Principles of Surgery
Step 6: ECMO (Extracorporeal Membrane Oxygenation)
ECMO provides mechanical support when conventional therapies fail.
| Mode | Indication | Mechanism |
|---|---|---|
| VV-ECMO | Severe respiratory failure (refractory ARDS) with intact cardiac function | Provides gas exchange (O2 delivery + CO2 removal), allows "lung rest" |
| VA-ECMO | Cardiogenic shock or combined cardiorespiratory failure | Provides both cardiac support and gas exchange |
| V-AV ECMO | Dynamic scenarios needing both circulatory and respiratory support | Hybrid approach |
- Sabiston Textbook of Surgery
ECMO in ARDS: VV-ECMO is used when PaO2/FiO2 <80 despite optimal ventilation, or when lung-protective ventilation is incompatible with adequate gas exchange.
6. Pharmacological Management
Bronchodilators (obstructive disease)
- Short-acting beta-2 agonists (SABA): Salbutamol (albuterol) 2.5-5 mg nebulized q20min x3, then PRN; or MDI with spacer
- Short-acting anticholinergics (SAMA): Ipratropium bromide 0.5 mg nebulized q6h; additive to SABA
- IV magnesium sulfate: 1.2-2 g IV over 20 min in severe acute asthma - bronchodilator effect via Ca2+ antagonism
- IV methylxanthines (aminophylline): Second-line in severe refractory bronchospasm
Corticosteroids
- Systemic steroids in COPD exacerbations: Prednisolone 40 mg PO or methylprednisolone 0.5 mg/kg IV q6h x 5 days; reduce treatment failure and shorten hospitalization
- Dexamethasone for croup and post-extubation stridor
Diuretics
- For acute cardiogenic pulmonary edema: Furosemide 40-80 mg IV (or 2.5x home dose); reduces preload and relieves pulmonary congestion
- Combined with nitrates in acute pulmonary edema (IV nitrates reduce preload rapidly)
Antibiotics
- Indicated for infectious causes (pneumonia, COPD exacerbation with purulent sputum, sepsis-related RF)
- Target empirically based on suspected pathogen and severity; adjust per culture results
Opioids (palliative dyspnea management)
- Low-dose IV/SC morphine 2-4 mg PRN relieves distressing dyspnea in end-stage disease without significantly worsening respiratory status in carefully selected patients
Sedation and Analgesia (in mechanically ventilated patients)
- Analgesia-first approach: IV fentanyl or morphine for pain
- Light sedation target (RASS -1 to 0): Associated with better outcomes than deep sedation
- Propofol (ICU sedation, short-acting, easily titratable) or dexmedetomidine (alpha-2 agonist, preserves respiratory drive)
- Benzodiazepines (midazolam, lorazepam): Avoid in delirium; associated with worse ICU outcomes
- In ECMO patients, specific sedation goals are used to minimize circuit-drug interactions and facilitate earlier mobilization - Sabiston Textbook of Surgery
7. Supportive ICU Care
| Domain | Intervention |
|---|---|
| Fluid management | Conservative fluid strategy after resuscitation; avoid fluid overload (worsens hypoxemia in ARDS) |
| Nutrition | Early enteral nutrition (within 24-48h); avoid overfeeding (excess carbohydrate raises VCO2 and CO2 load) |
| Electrolytes | Maintain K+ >4.0, Mg2+ >0.8, PO4 >1.0 mmol/L (hypophosphatemia weakens diaphragm) |
| DVT prophylaxis | Pharmacologic (LMWH) + mechanical (compression stockings) |
| Stress ulcer prophylaxis | PPI or H2 blocker in high-risk intubated patients |
| Glycemic control | Target glucose 7.8-10 mmol/L (140-180 mg/dL); avoid hypoglycemia |
| Delirium prevention | ABCDEF bundle (Awakening, Breathing, Coordination, Delirium, Exercise/mobility, Family) |
| Daily SBTs | Spontaneous breathing trials (SBT) once extubation criteria met - reduces ventilator days |
| Posture | Head of bed 30-45°; prone positioning in severe ARDS |
8. Weaning from Mechanical Ventilation
Readiness criteria (all should be met):
- Underlying cause resolving
- Hemodynamically stable (minimal or no vasopressors)
- Adequate oxygenation: SpO2 ≥92% on FiO2 ≤0.4, PEEP ≤8 cmH2O
- Capable of spontaneous respiratory effort
- Alert, following commands; intact cough/gag
Spontaneous Breathing Trial (SBT):
- T-piece or pressure support (PS 5 cmH2O + PEEP 5 cmH2O) for 30-120 minutes
- Failed SBT signs: RR >35/min, SpO2 <90%, HR >140, BP swing >20%, agitation, diaphoresis
Extubation failure rescue:
- Preferentially use HFNC or NIV BiPAP post-extubation in high-risk patients (COPD, cardiac failure, high APACHE score)
- High-flow nasal cannula is increasingly used for post-extubation respiratory failure in postoperative patients, with several studies demonstrating benefit - Schwartz's Principles of Surgery
9. Special Situations
Flail Chest
Multifactorial mechanism: pain → shallow breathing → atelectasis; impaired respiratory muscle efficiency; increased O2 cost of breathing. When compounded by lung contusion and hypoxemia → muscle fatigue → respiratory failure. Algorithm: pain control (epidural/PCA) → NIV/HFNC → intubation if failing → consider surgical fixation for unstable lateral segments. - Murray & Nadel's Textbook of Respiratory Medicine
Neuromuscular Disease
- When respiratory failure is the end of progressive chronic insufficiency (e.g., advanced CF, ALS), mechanical ventilation may be unhelpful and goals-of-care discussions are required. For acute-on-chronic (e.g., viral pneumonia in CF), mechanical ventilation is appropriate in patients with previously good baseline pulmonary function. - Fishman's Pulmonary Diseases and Disorders
Postoperative Respiratory Failure
- Reverse residual neuromuscular blockade and opioid-induced respiratory depression
- HFNC or NIV as first-line; intubate if failing or contraindicated
10. Complications of Mechanical Ventilation
| Complication | Prevention/Management |
|---|---|
| Ventilator-Induced Lung Injury (VILI) | Lung-protective low VT, limit plateau pressure |
| Ventilator-Associated Pneumonia (VAP) | Oral care, HOB elevation, SDD, minimize sedation |
| Barotrauma (pneumothorax) | Monitor peak/plateau pressures; low VT |
| Oxygen toxicity | Wean FiO2 to minimum needed; target SpO2 88-95% (not 100%) |
| Diaphragm atrophy | Early weaning, avoid deep sedation, maintain respiratory effort |
| Hemodynamic compromise | High PEEP reduces venous return; monitor CVP, volume status |
11. Key Prognostic Indicators
- PaO2/FiO2 ratio: <200 = moderate ARDS; <100 = severe ARDS; predicts mortality
- Driving pressure (plateau - PEEP): independent predictor of mortality in ARDS
- pH on admission: pH <7.20 associated with poor outcomes
- Duration of mechanical ventilation: >10-14 days significantly increases morbidity
- Patients who survive but remain "chronically critically ill" - require dedicated post-ICU rehabilitation programs
Key References:
- Fishman's Pulmonary Diseases and Disorders, 5th ed., Chapter 139 (Respiratory Failure - Classification, Pathophysiology, Management)
- Murray & Nadel's Textbook of Respiratory Medicine, 7th ed., Chapter on HFNC and Acute Hypoxemic Respiratory Failure
- Rosen's Emergency Medicine, 9th ed., Chapter 60 (COPD and Respiratory Failure Classification)
- Sabiston Textbook of Surgery, Chapter 116 (ECMO in Respiratory and Cardiac Failure)
- Schwartz's Principles of Surgery, 11th ed., Chapter on Postoperative Respiratory Failure
This is a shared conversation. Sign in to Orris to start your own chat.