meniscus repair criteria
Reading File
Finding Sources
Searching PubMed
"meniscus repair" criteria outcomes
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
I now have all the information needed for a comprehensive answer.
Meniscus Repair Criteria
Vascularity Zones (the Foundation of Decision-Making)
The meniscus is divided into three zones based on blood supply from the perimeniscal capillary plexus:
| Zone | Location | Vascularity | Healing Potential |
|---|---|---|---|
| Red-red zone | Outer 1/3 (meniscosynovial junction) | Fully vascular | Excellent |
| Red-white zone | Middle 1/3 (within ~3 mm of junction) | Partial | Good |
| White-white zone | Inner 1/3 | Avascular | Poor/repair controversial |
Tears That Can DEFINITELY Be Repaired
According to Campbell's Operative Orthopaedics (15th Ed, 2026), tears that definitely qualify for repair are:
- Single vertical (longitudinal) tears in the peripheral vascular portion (red-red or red-white zone, within 3 mm of the meniscosynovial junction)
- Tear is displaceable (unstable on probing)
- Length >1 cm (shorter peripheral tears of ≤7 mm with <3 mm displacement can often heal with rasping alone, without sutures)
- Minimal damage to the body of the meniscus
- Acute presentation (fresh tear with good tissue quality)
Patient-Related Criteria (Bailey & Love's Surgery, 28th Ed)
| Factor | Favorable | Unfavorable |
|---|---|---|
| Age | Young (active patients) | Elderly |
| Presentation timing | Early (acute) | Late/chronic |
| Tear configuration | Simple, vertical/longitudinal | Complex, horizontal, degenerative |
| Knee stability | Stable (or ACL reconstruction planned) | Chronic ACL-deficient, unstable |
| Articular cartilage | Preserved (<Outerbridge grade II) | Significant chondral damage |
Conditional Repairs (Certain Circumstances)
- Tears 3-5 mm from the meniscosynovial junction may be repaired when:
- Tourniquet deflation confirms vascularity (rasping produces bleeding)
- Patient is young and active with minimal meniscal body damage
- ACL reconstruction is performed concomitantly (hemarthrosis enhances healing)
- Trephination with an 18-gauge spinal needle can be used to stimulate bleeding and create vascular access channels in borderline tears
Special Tear Types
- Posterior root tears (10-20% of tears): must be repaired in non-arthritic knees to prevent cartilage overload and degeneration - transtibial tunnel + button fixation
- Ramp lesions: peripheral posterior horn medial meniscal tears from ACL pivot shift - repair recommended
- Radial tears: complete radial tears to the meniscosynovial junction should be repaired (horizontal mattress) to preserve load-distribution function; a 2026 systematic review (PMID 42432690) confirms favorable healing rates for surgical repair of radial tears
- Bucket-handle tears: acute displaced bucket-handle tears in young patients are candidates for repair; keep patient non-weight bearing on crutches until MRI confirms, to prevent fragment damage
Contraindications to Repair
- Degenerative/chronic tears with distorted, fixed tissue
- White-white zone (avascular inner third) - if repair attempted, requires fibrin clot or biologic augmentation
- Significant chondral damage (Outerbridge III-IV)
- Horizontal cleavage tears in older patients - generally resect
- Unstable ACL-deficient knee (relative contraindication unless concurrent ACL reconstruction)
Repair Technique Selection (Box 56.3, Campbell's)
| Technique | Best For |
|---|---|
| Outside-in sutures | Anterior horn, midthird, radial tears |
| Inside-out sutures | Posterior horn, midthird, displaced bucket-handle |
| All-inside fixator implants | Posterior horn tears, 2-3 mm rim width, vertical/longitudinal, midthird, radial tears |
Campbell's Core Principles
"Preserve functional meniscus; resect and contour damaged tissue. Repair the meniscus to protect the cartilage; repair the cartilage to protect the meniscus."
The key mnemonic for lateral meniscus is the "3 Rs": Wrisberg rips, ramp lesions, and posterior root tears - all require identification and repair.
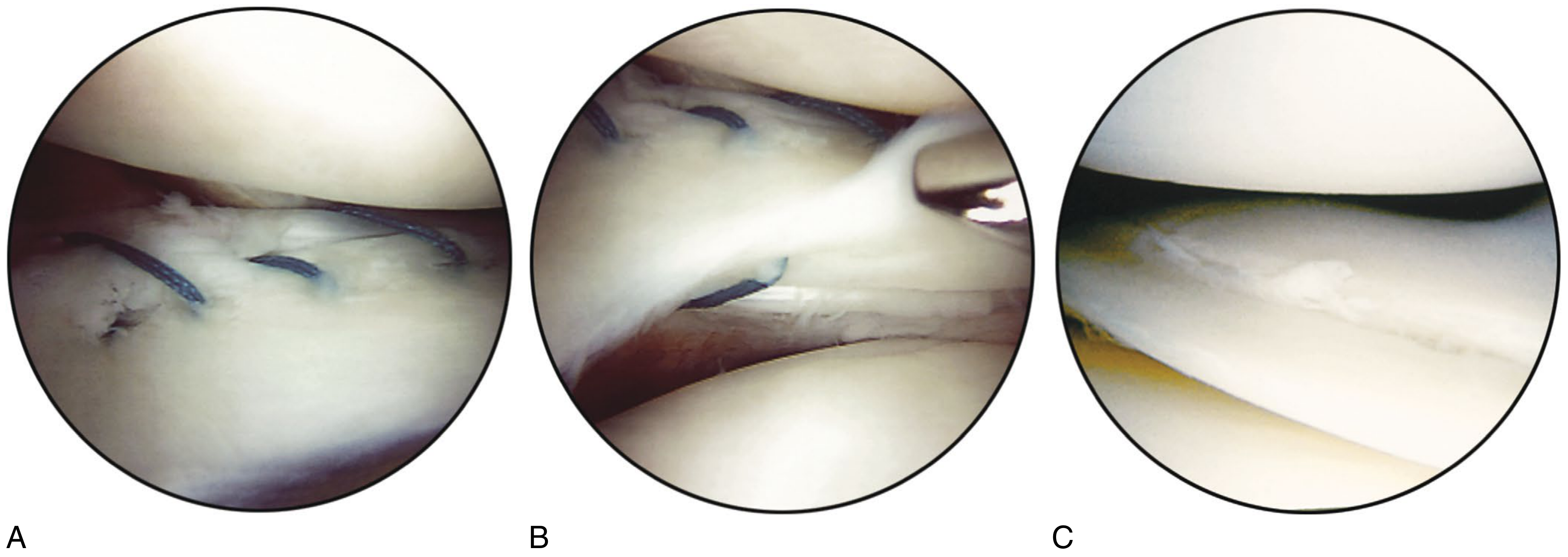
Arthroscopic views: A) unstable peripheral tear repaired with stacked vertical mattress sutures, B) incomplete undersurface tear treated with abrasion + 1-2 sutures, C) complete tear in the avascular zone - generally excised unless fibrin clot augmentation is used
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 3059-3065
- Bailey and Love's Short Practice of Surgery 28th Ed, p. 585
topics to be studied in detail for case presentation of a case of periprosthetic(hemi arthroplasty right hip) fracture femur
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Here is a complete, structured guide of topics to study in detail for your case presentation of a periprosthetic femur fracture around a right hip hemiarthroplasty.
Topics for Case Presentation: Periprosthetic Femur Fracture Around Right Hip Hemiarthroplasty
1. THE ORIGINAL PROCEDURE - Hemiarthroplasty Right Hip
Why it was done (the background diagnosis)
- Femoral neck fracture - most common indication
- Garden classification of femoral neck fractures:
- Garden I (incomplete/impacted), II (complete undisplaced), III (partial displacement), IV (complete displacement)
- Garden III and IV = displaced intracapsular fractures - primary indication for hemiarthroplasty
- Pauwels classification (angle of fracture line): Type I <30°, Type II 30-50°, Type III >50° - relevant to biomechanical stability
- AO/OTA classification of femoral neck fractures
Indications for Hemiarthroplasty vs. other options
| Option | Indication |
|---|---|
| Cannulated screws | Undisplaced (Garden I/II), young patients |
| Hemiarthroplasty | Displaced (Garden III/IV), elderly, low-demand |
| Total Hip Arthroplasty (THA) | Displaced, active, cognitively intact (NICE guidelines) |
- NICE guidelines: THA preferred if patient walks independently (no more than a stick), expected to perform ADLs for >2 years, no contraindication to THA
- Hemiarthroplasty advantages: shorter operative time, less blood loss, lower dislocation rate (0.9% vs 1.6% for THA)
- Hemiarthroplasty disadvantages: risk of acetabular erosion/wear, no ability to resurface acetabulum
Implant types in hemiarthroplasty
- Unipolar (Austin Moore, Thompson): single articulation at native acetabulum - higher acetabular wear
- Bipolar: inner and outer articulations - theoretically less acetabular wear (long-term data show no significant difference)
- Cemented vs. uncemented:
- Cemented: lower risk of periprosthetic fracture, risk of bone cement implantation syndrome (BCIS)
- Uncemented: higher fracture risk, especially intraoperatively with press-fit stems
Surgical approaches
- Posterior approach (Moore): most common, higher dislocation risk
- Anterolateral (Watson-Jones): lower dislocation rate
- Direct lateral (Hardinge): risk of abductor damage
2. ANATOMY - Proximal Femur and Implant
Bony anatomy
- Femoral head, neck, greater and lesser trochanters
- Femoral shaft - cortical thickness, medullary canal dimensions
- Calcar femorale - dense cortical bone at inferomedial neck-shaft junction
- Anterior bow of the femur (relevant to stem fit and fracture pattern)
Vascular anatomy
- Medial and lateral circumflex femoral arteries (from profunda femoris)
- Retinacular vessels along femoral neck - critical for femoral head vascularity
- Perimeniscal capillary plexus not applicable here - focus on periosteal blood supply of diaphysis
Implant-bone interface zones
- Metaphyseal fit (proximal), diaphyseal fit (distal)
- Stem tip = stress riser - highest risk zone for fracture
3. PERIPROSTHETIC FEMUR FRACTURE (PPF) - Core Topic
Definition
Fracture occurring in bone adjacent to or around a femoral hip implant, arising as a complication of the hemiarthroplasty.
Epidemiology and Risk Factors
- Incidence after primary THA: <1% to 2.3% postoperatively; 0.8% at 5 years, 3.5% at 10 years
- Incidence after hemiarthroplasty is similar, slightly higher with uncemented stems
- Projected to rise 4.6% per decade due to increasing arthroplasty burden
- Patient risk factors: osteoporosis, female sex, rheumatoid arthritis, Paget's disease, osteolysis, revision surgery (6x higher risk), old age
- Implant risk factors: uncemented stem (higher risk than cemented), poor cortical index, previous osteolysis/lysis around stem
Timing
- Intraoperative: calcar crack during insertion of press-fit stem - may be unrecognized
- Early postoperative: propagation of unrecognized intraoperative fracture
- Late postoperative: low-energy fall onto background of osteoporosis or periprosthetic osteolysis
4. CLASSIFICATION - The Most Important Topic
Vancouver Classification (Standard - must know in detail)
The Vancouver classification considers 3 factors: fracture location, implant stability, bone stock quality.
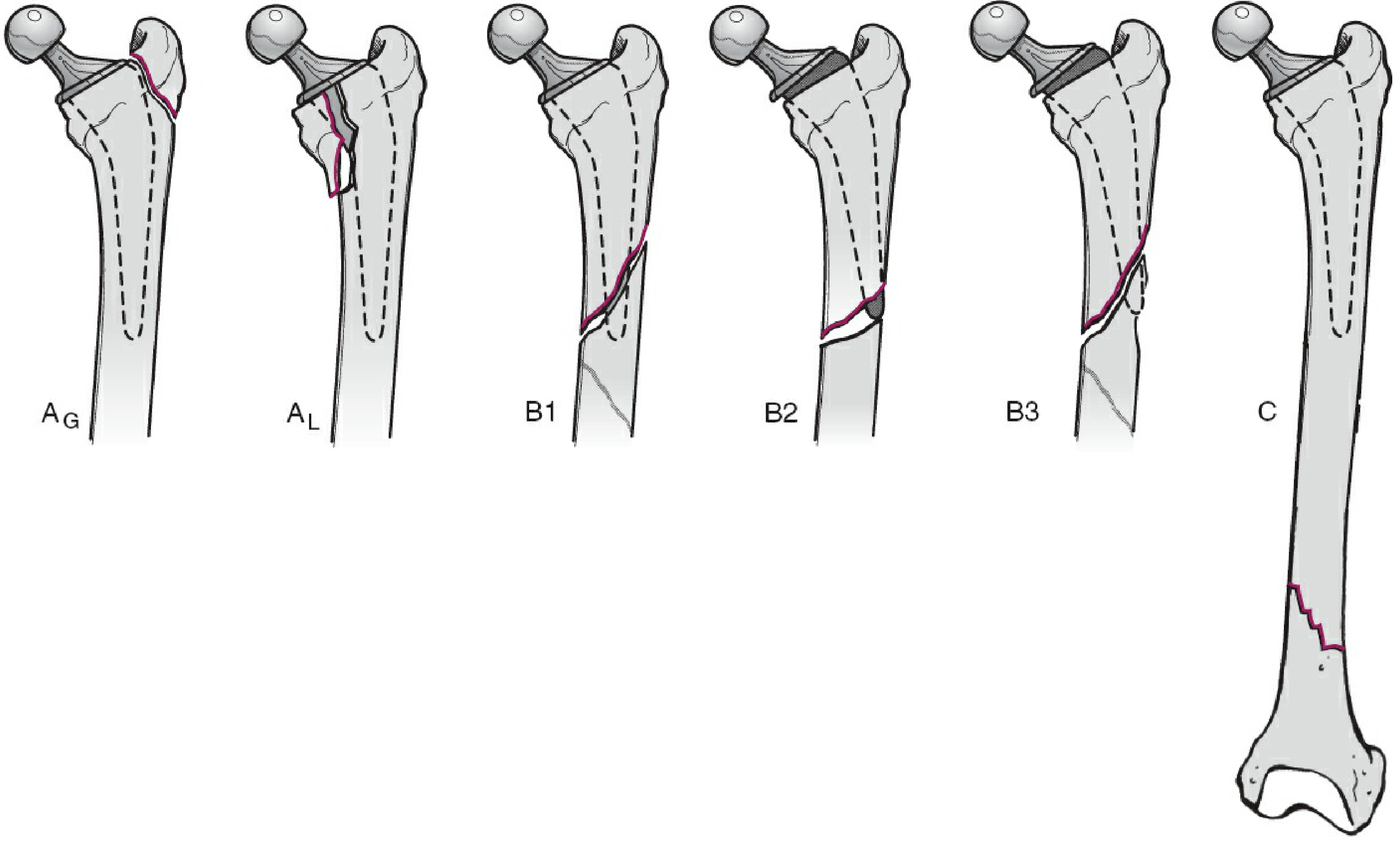
| Type | Location | Subtypes | Details |
|---|---|---|---|
| A | Trochanteric region | AG - greater trochanter, AL - lesser trochanter | Metaphyseal, proximal to stem |
| B | At or around stem tip | B1 - stable stem, B2 - loose stem, B3 - loose stem + poor bone stock | Most common type, most important clinically |
| C | Distal to stem tip | - | Treat independently of prosthesis |
- B1: fracture around stem tip, stem is well-fixed - treat with ORIF (plate + screws ± strut allograft)
- B2: fracture around stem tip, stem is loose - revision arthroplasty to long stem
- B3: fracture around loose stem + significant bone loss - revision + allograft/proximal femoral replacement
Key clinical challenge: Distinguishing B1 from B2 intraoperatively (implant stability testing) and radiographically.
Intraoperative Vancouver Classification
| Subtype | Morphology | Zone |
|---|---|---|
| I | Cortical perforation | A / B / C |
| II | Undisplaced linear crack | A / B / C |
| III | Displaced/unstable fracture | A / B / C |
Unified Classification System for Periprosthetic Fractures (UCPF)
- More recently proposed, applicable across all joints
5. CLINICAL PRESENTATION AND WORKUP
History
- Original indication for hemiarthroplasty (displaced NOF fracture)
- Mechanism of current injury (low-energy fall vs. spontaneous)
- Pre-fracture hip symptoms: mechanical thigh pain or groin pain = suggests loosening even before fracture
- Comorbidities: osteoporosis (on bisphosphonates?), rheumatoid arthritis, steroid use, metabolic bone disease
- Functional status pre- and post-hemiarthroplasty
Examination
- Pain, deformity, shortening, external rotation of the limb
- Neurovascular status (sciatic nerve, femoral nerve)
- Skin condition, wounds (previous surgical scars)
- Signs of infection (warmth, erythema, discharge)
Investigations
Radiological
- AP pelvis and lateral hip X-ray (baseline comparison with old films is essential)
- Full-length femur X-ray - to assess entire stem and distal extent of fracture
- CT scan - fracture pattern, bone stock assessment, implant positioning
- Look for: stem subsidence, cement mantle fracture, endosteal scalloping/osteolysis (loosening signs)
Laboratory
- FBC, ESR, CRP - rule out periprosthetic joint infection (PJI) as a differential
- Serum calcium, phosphate, ALP, PTH - metabolic bone disease
- Renal function (bisphosphonate use, contrast for CT)
- Clotting, group and save (pre-operative)
Nuclear Medicine
- Bone scan/SPECT - assess implant loosening (increased uptake around stem tip = loose)
- White cell scan - if PJI suspected
6. TREATMENT - The Heart of the Presentation
Treatment Algorithm Based on Vancouver Type
| Type | Treatment |
|---|---|
| AG (greater trochanter) | Non-op if non-displaced + stable abductors; ORIF with wires/cables if displaced |
| AL (lesser trochanter) | Usually non-operative |
| B1 (fracture, stable stem) | ORIF - lateral locking plate + unicortical screws above stem, bicortical below; ± cortical strut allograft |
| B2 (fracture, loose stem) | Revision to long uncemented revision stem ± plate/strut allograft |
| B3 (fracture, loose stem, poor bone) | Revision + impaction bone grafting, allograft-prosthesis composite, or proximal femoral replacement |
| C (distal to stem) | Treat as standard femur fracture; retrograde nail or plate (must clear stem tip) |
Non-operative Treatment
- Only for: truly non-displaced fractures, patient unfit for surgery, or minimal functional demands
- Non-displaced B fractures: protected weight bearing + teriparatide (PTH analogue) - 100% union in B1, 75% in B2 in one series
ORIF Techniques for B1
- Locking plates with unicortical screws/cables proximal (around stem), bicortical screws distal
- Cortical strut allografts - onlay grafts supplementing plate fixation, biologic augmentation
- Cable-plate systems (e.g., Dall-Miles)
Revision Arthroplasty for B2/B3
- Long-stem uncemented revision femoral component (bypasses fracture by 2+ cortical diameters)
- ± adjuvant lateral plate or cortical strut allograft
- Check acetabular component stability - may need concomitant acetabular revision
- Pre-operative planning: obtain original operative note, manufacturer details for component compatibility
Special Surgical Considerations
- Bone cement implantation syndrome (BCIS) if cementing a new stem
- Intraoperative cerclage wires for calcar cracks during stem insertion
- Need for bone graft - autograft (iliac crest) or allograft struts
7. COMPLICATIONS
Early
- Re-fracture
- Implant failure (stem subsidence, plate breakage)
- Infection / Periprosthetic Joint Infection (PJI)
- Dislocation
- Neurovascular injury (sciatic nerve palsy - risk if leg lengthened >3-5 cm)
- DVT / PE (high risk in elderly post-arthroplasty)
- BCIS
Late
- Non-union
- Malunion
- Aseptic loosening of revised stem
- Heterotopic ossification
- Acetabular erosion (hemiarthroplasty-specific)
Mortality
- PPF carries high 1-year mortality in elderly patients - equivalent to the original hip fracture
- 8-fold higher mortality rate vs age-matched controls; ~11% in some ORIF series
- Functional outcomes (Oxford Hip Score) are worse than revision THA for other causes
8. POSTOPERATIVE REHABILITATION AND WEIGHT BEARING
- Weight bearing status depends on fracture type and fixation
- B1 (ORIF): protected weight bearing until radiologic evidence of healing
- B2/B3 (revision with long stem): often immediate full weight bearing if stem bypasses fracture adequately
- DVT prophylaxis (LMWH / DOACs), physiotherapy, fall prevention
- Osteoporosis management: calcium, vitamin D, bisphosphonates (note: hold until fracture heals)
9. RELEVANT SCORES AND OUTCOME MEASURES
- Oxford Hip Score (OHS) - functional outcome
- Harris Hip Score - widely used in hip arthroplasty
- Parker Mobility Score - pre-fracture mobility assessment
- ASA grade - anaesthetic risk
- Nottingham Hip Fracture Score - 30-day mortality prediction
10. IMPORTANT DIFFERENTIAL DIAGNOSES TO MENTION
- Periprosthetic Joint Infection (PJI) - can cause pathological fracture; elevated ESR/CRP; use ICM (International Consensus Meeting) criteria
- Aseptic loosening without fracture
- Stress fracture vs. insufficiency fracture (osteoporotic)
- Pathological fracture from metastatic disease (rule out with bone scan + primary workup if suspected)
Summary of Key Learning Points for Your Case
| Domain | Key Thing to Know |
|---|---|
| Classification | Vancouver system - types A/B1/B2/B3/C; three determinants |
| Diagnosis | Full-length femur X-ray + old films for comparison |
| B1 vs B2 | Hinge of entire treatment decision - assess stem stability |
| B1 treatment | ORIF with locking plate ± strut allograft |
| B2/B3 treatment | Revision to long-stem implant ± allograft/proximal femoral replacement |
| Prognosis | High mortality in elderly; worse outcomes than standard THA revision |
| Infection | Always rule out PJI with serologies before surgery |
| Hemiarthroplasty | Know why it was done - Garden III/IV NOF, its implant types, and complications |
Sources: Rockwood and Green's Fractures in Adults 10th Ed, 2025 (Ch. 59); Campbell's Operative Orthopaedics 15th Ed, 2026; Miller's Review of Orthopaedics 9th Ed; Bailey and Love's Short Practice of Surgery 28th Ed
This is a shared conversation. Sign in to Orris to start your own chat.