Pneumothorax
Reading File
Finding Sources
Searching PubMed
pneumothorax management treatment
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Pneumothorax
Pneumothorax is defined as an abnormal collection of air in the pleural space between the parietal and visceral pleura. It ranges from a minor incidental finding to a life-threatening emergency.
Classification
| Type | Description |
|---|---|
| Primary Spontaneous | No underlying lung disease; blebs rupture in otherwise healthy individuals |
| Secondary Spontaneous | Occurs in setting of pre-existing lung disease |
| Traumatic | Penetrating or blunt chest trauma; includes iatrogenic |
| Tension | One-way valve mechanism; pressure builds progressively - medical emergency |
Pathophysiology
Normally, intrapleural pressure is negative throughout the respiratory cycle. When the alveolar-pleural barrier is disrupted, air enters the pleural space until either the defect seals or intraalveolar and intrapleural pressures equalize. This collapses the ipsilateral lung and reduces vital capacity, functional residual capacity (FRC), and total lung capacity (TLC). Hypoxemia results from shunting through atelectatic lung, though hypoxic vasoconstriction in the collapsed lung partially compensates.
In tension pneumothorax, the pleural defect acts as a one-way valve: air enters during inspiration but cannot escape during expiration. Progressive air accumulation causes:
- Increasing intrapleural pressure
- Mediastinal shift to the contralateral side
- Compression of mediastinal veins - reduced venous return
- Cardiovascular collapse and death if untreated
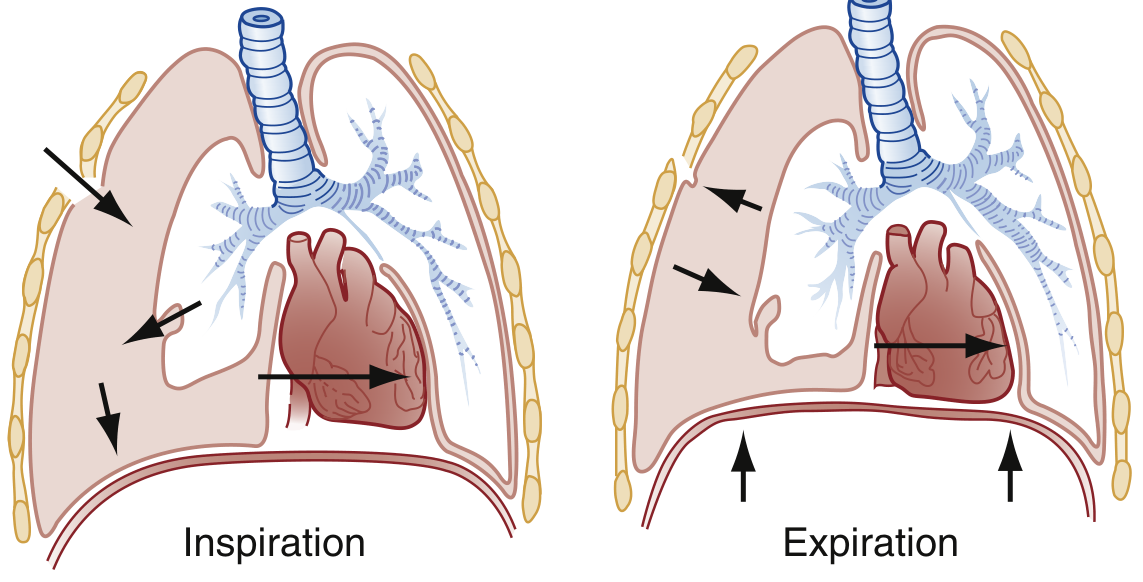
Tension pneumothorax: during inspiration air enters the pleural space; during expiration the valve closes and air cannot escape. - Rosen's Emergency Medicine
Primary Spontaneous Pneumothorax (PSP)
- Classic profile: tall, thin young male in 2nd-4th decade; 3:1 male-to-female ratio
- Incidence ~10/100,000 in men, ~3/100,000 in women
- Etiology: rupture of subpleural blebs (small thin-walled cystic spaces at the lung apex), found at CT or surgery in ~80% of patients
- Risk factors: smoking (10-20x increased risk, dose-dependent), Marfan syndrome, mitral valve prolapse, changes in ambient atmospheric pressure
- Recurrence: ~25% after first episode, typically within 1-2 years; ~50-60% after second; even higher after third
Secondary Spontaneous Pneumothorax (SSP)
SSP occurs in patients with underlying lung disease and is physiologically more serious due to limited pulmonary reserve. Patients are typically 15-20 years older than those with PSP. Death is not rare in SSP (versus extremely rare in PSP).
Causes of Secondary Spontaneous Pneumothorax:
- Airway disease: COPD (most common in US), asthma, cystic fibrosis (marker of poor prognosis)
- Infections: Pneumocystis jirovecii pneumonia (HIV), tuberculosis, lung abscess (leading causes in developing countries)
- Interstitial lung disease: sarcoidosis, IPF, lymphangioleiomyomatosis, tuberous sclerosis, pneumoconioses
- Neoplasms: primary lung cancers, pulmonary/pleural metastases
- Connective tissue disease: Marfan syndrome, Ehlers-Danlos, scleroderma, rheumatoid arthritis
- Miscellaneous: pulmonary infarction, endometriosis (catamenial pneumothorax)
Traumatic and Iatrogenic Pneumothorax
Traumatic pneumothoraces arise from penetrating or blunt chest injuries and are usually treated with tube drainage. Iatrogenic pneumothorax is increasingly common - leading causes include transthoracic needle aspiration, thoracentesis, and central line placement. Most iatrogenic cases can be managed with supplemental oxygen or aspiration.
Clinical Features
Symptoms (often begin suddenly):
- Ipsilateral pleuritic chest pain - sharp, sudden onset, may evolve to dull ache
- Dyspnea (may be mild in PSP without underlying disease)
- Dry cough (occasional)
- Patients may wait days before seeking care; symptoms can spontaneously improve within 24-72 hours even while pneumothorax persists
Signs (simple pneumothorax):
- Decreased/absent breath sounds on the affected side
- Hyperresonance to percussion
- Tachycardia (anxiety-driven)
- Subcutaneous emphysema (rare)
- Small-to-moderate pneumothoraces may have no physical signs
Signs of Tension Pneumothorax (not all need be present):
- Air hunger, severe dyspnea
- Tachycardia, then hypotension
- Elevated peak airway pressures (ventilated patients)
- Jugular venous distention (may be absent if hypovolemic)
- Hyperresonance on affected side (difficult in a noisy resuscitation area)
- Absent/diminished breath sounds ipsilaterally
- Tracheal deviation away from the affected side (late, not always present)
- Cardiovascular collapse - cardiac arrest if untreated
Treat tension pneumothorax clinically before waiting for a chest X-ray. Absence of tracheal deviation does NOT rule it out. - Tintinalli's Emergency Medicine
Diagnosis
Chest X-ray: First-line investigation. Shows a visible pleural line with absent lung markings beyond it. In erect posture, air collects at the apex. In supine patients, air collects anteriorly and may be subtle. Tension pneumothorax shows mediastinal shift away from the pneumothorax, diaphragm depression, and widened rib spaces.
CT Chest: Provides precise sizing, identifies underlying blebs/bullae, guides drainage of loculated collections.
Lung Ultrasound (POCUS):
- Presence of pleural sliding (lung sliding sign) excludes pneumothorax at that location
- Absence of sliding (with A-line pattern/"bar code sign" on M-mode = "stratosphere sign") suggests pneumothorax
- Lung point sign (transition from sliding to no-sliding) is highly specific for pneumothorax and can estimate size
- B-lines exclude pneumothorax at that location
- More sensitive than CXR in experienced hands
Note on supplemental O₂: Oxygen is absorbed ~60x faster than nitrogen, and CO₂ ~20x faster than O₂. Supplemental oxygen accelerates resorption of the pneumothorax (1-5% per 24 hours at baseline on room air). - Current Surgical Therapy 14e
Management
Simple Pneumothorax - Observation
- Small pneumothorax in a spontaneously breathing, stable patient: observation with repeat CXR in 4-6 hours, drain only if expanding
- This is NOT an option in patients on any form of positive pressure ventilation (PPV), as simple can rapidly progress to tension
Needle Decompression (Tension Pneumothorax)
- Immediate large-bore needle into the 2nd intercostal space, midclavicular line (or 4th-5th ICS, anterior axillary line per updated ATLS)
- Life-saving; follow immediately with tube thoracostomy
Tube Thoracostomy (Chest Drain)
- Indicated for: tension pneumothorax after needle decompression, secondary spontaneous pneumothorax (nearly all patients), ventilated patients, expanding pneumothorax
- Small-bore tubes (24 Fr) or pigtail catheters via Seldinger technique for simple air evacuation
- Connect to water-seal drainage system with suction (~20 cmH₂O for persistent air leaks)
- Wean to water seal only after air leak resolves
- For loculated pneumothoraces: ultrasound- or CT-guided percutaneous drainage
Chemical/Surgical Pleurodesis
- For recurrent PSP or failed lung expansion: thoracoscopy with stapling of blebs + pleurodesis
- Nearly 100% effective in preventing recurrence
- Chemical pleurodesis for patients who refuse or are not candidates for surgery
PSP-Specific Guidance
- Asymptomatic or minimally symptomatic: conservative management / outpatient observation is an option for low-risk patients
- Recurrent pneumothorax or failed expansion: thoracoscopy with bleb stapling + pleurodesis
SSP-Specific Guidance
- Nearly all need tube drainage
- Many require thoracoscopy/thoracotomy with bleb stapling + surgical pleurodesis
- Cystic fibrosis-related pneumothorax carries poor prognosis; management is complex
Return to Sports
After pneumothorax, return to play is generally safe after 3-4 weeks if the patient is stable and there was less than 15-20% volume loss. - Textbook of Family Medicine
Special Situations
Mechanically Ventilated Patients: Pneumothorax stems from alveolar overdistension (volutrauma/barotrauma). All pneumothoraces in ventilated patients should be drained to prevent tension pneumothorax. COPD and asthma patients are especially prone.
Hemopneumothorax: Two chest tubes - one superior (air) and one inferior (blood).
Catamenial Pneumothorax: Rare condition related to thoracic endometriosis; occurs in menstruating women. Recent systematic review (2026) confirms surgical management (VATS) as the mainstay.
Iatrogenic Tension Pneumothorax: Can occur from aggressive bag-valve-mask ventilation, especially in COPD/asthma patients.
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Rosen's Emergency Medicine | Current Surgical Therapy 14e | Murray & Nadel's Textbook of Respiratory Medicine | Tintinalli's Emergency Medicine | Roberts and Hedges' Clinical Procedures in Emergency Medicine
Chest xray of pneumothorax
Finding Sources
Searching the Web
pneumothorax chest xray findings radiology images
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have all the images and textbook content needed for a thorough radiological review. Here is the complete answer:
Chest X-Ray of Pneumothorax
The Key Radiographic Sign: Visceral Pleural Line
The hallmark of pneumothorax on CXR is a thin, sharp white line (the visceral pleural line) separated from the chest wall by a lucent (black) zone devoid of lung markings. This line has lucency on both sides - air in the lung on one side, and air in the pleural space on the other.
"The outer margin of the visceral pleura separated from the parietal pleura by a lucent space devoid of pulmonary vessels." - Fishman's Pulmonary Diseases
CXR Appearances by Position
Upright (Erect) Patient
Gas rises to the apex. The pleural line is most easily seen at the apex/upper zone. Look for:
- A visible pleural line in the upper hemithorax
- Absent vascular markings beyond that line
- Increased lucency (blacker) in the peripheral zone
CXR: Right-sided pneumothorax - absent lung markings and increased lucency lateral to the pleural line

Right-sided pneumothorax. Absent lung markings and increased air density lucency lateral to the pleural line. - Tintinalli's Emergency Medicine
CXR: Pneumothorax with pleural line visible at apex + skinfold comparison
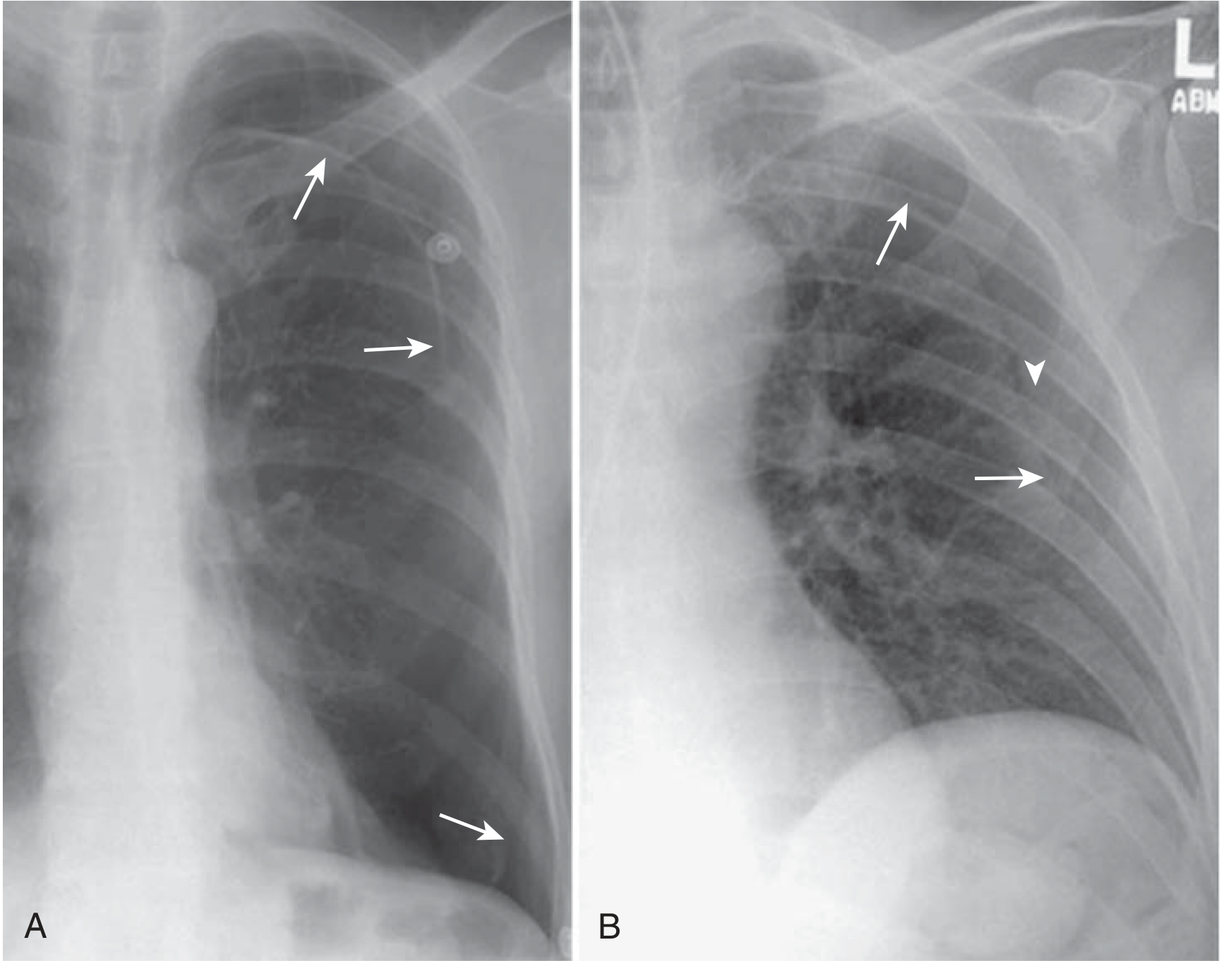
(A) True pneumothorax: the pleural line has lucency on both sides, no blood vessels seen beyond it, line traces the lung contour continuously (arrows).
(B) Skinfold mimic: lucency on only one side, border is poorly defined, blood vessels can be traced beyond the fold (arrowhead).
- Murray & Nadel's Textbook of Respiratory Medicine
CXR: Upright vs. lateral decubitus comparison
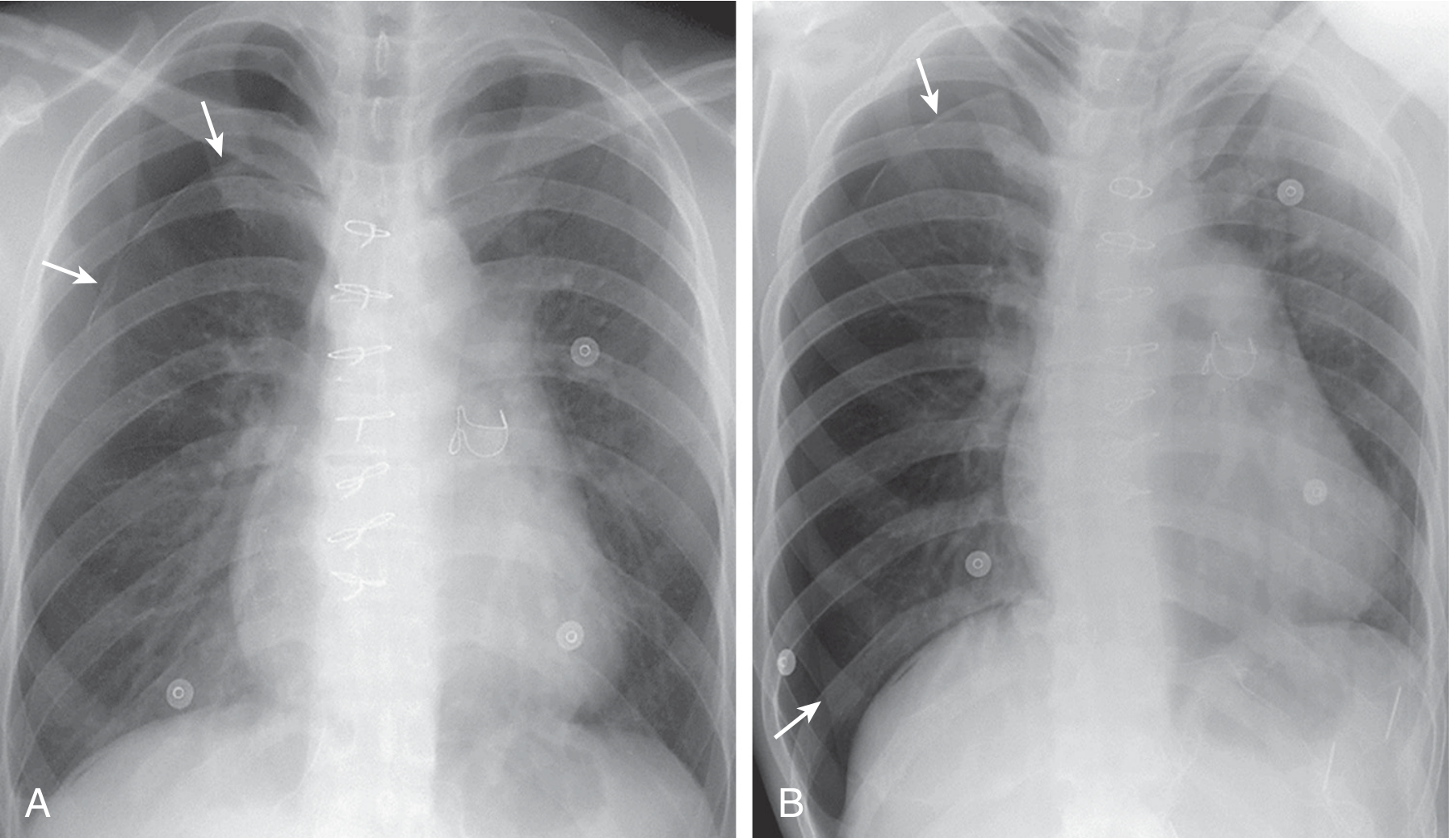
(A) Upright inspiratory CXR: pleural line (arrows) visible over the apex of the right lung.
(B) Left lateral decubitus view: gas in the pleural space migrates to the non-dependent (right) thorax, making the pleural line visible over both the apical and costophrenic regions (arrows).
- Murray & Nadel's Textbook of Respiratory Medicine
Supine Patient (ICU/Trauma)
Gas migrates anteriorly along the broad ventral surface of the lung - much harder to detect on a frontal film. CXR misses up to 80% of pneumothoraces in the supine position.
Look for:
| Sign | Location | Appearance |
|---|---|---|
| Deep sulcus sign | Costophrenic angle | Unusually deep, sharp, lucent costophrenic angle |
| Juxtacardiac lucency | Medial border of heart | Unusually lucent zone beside the cardiac silhouette |
| Subpulmonic lucency | Between lung base and diaphragm | Air-tissue interface |
CXR + CT: Bullae vs. pneumothorax distinction
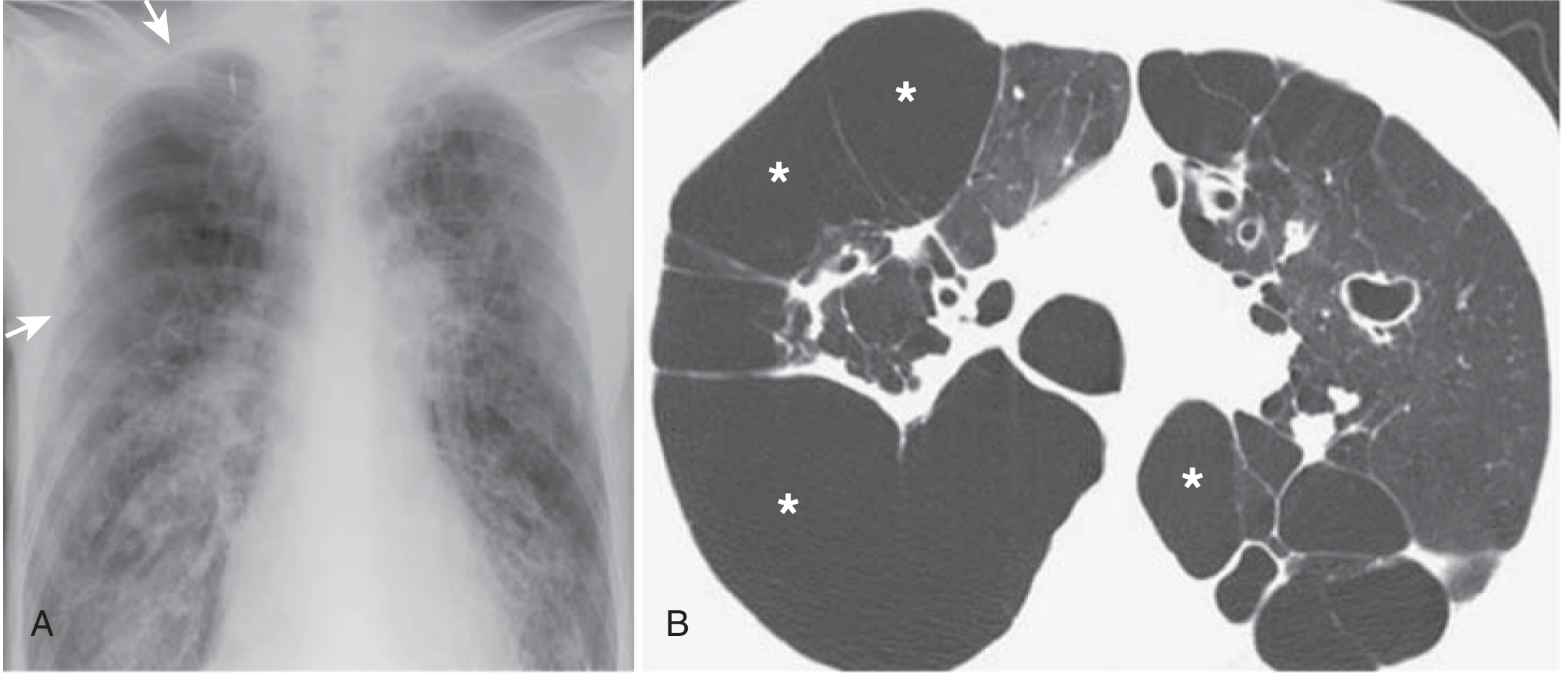
Bullae () resembling pneumothorax in a patient with cystic fibrosis. (A) CXR: subtle pleural line (arrows) easy to miss or confuse with bullae. (B) CT: confirms large bullae (* marking) rather than free pleural air. CT is definitive when CXR is ambiguous. - Murray & Nadel's*
CXR: Secondary spontaneous pneumothorax (silicosis)

Secondary spontaneous pneumothorax in a patient with nodular silicosis. The visceral pleural line is clearly seen (upper right) with absent vascular markings beyond it. Cicatricial bullae visible in both bases. - Fishman's Pulmonary Diseases
Tension Pneumothorax on CXR
Do NOT wait for CXR to treat tension pneumothorax - treat clinically first.
When present, CXR shows:
- Complete or near-complete lung collapse on affected side
- Mediastinal shift away from the affected side
- Tracheal deviation to the contralateral side
- Diaphragmatic depression (flattened or inverted hemidiaphragm on affected side)
- Widened intercostal spaces on the affected side
Note: Mediastinal shift can occur without true tension physiology if the mediastinum is mobile - it does not by itself equal tension pneumothorax.
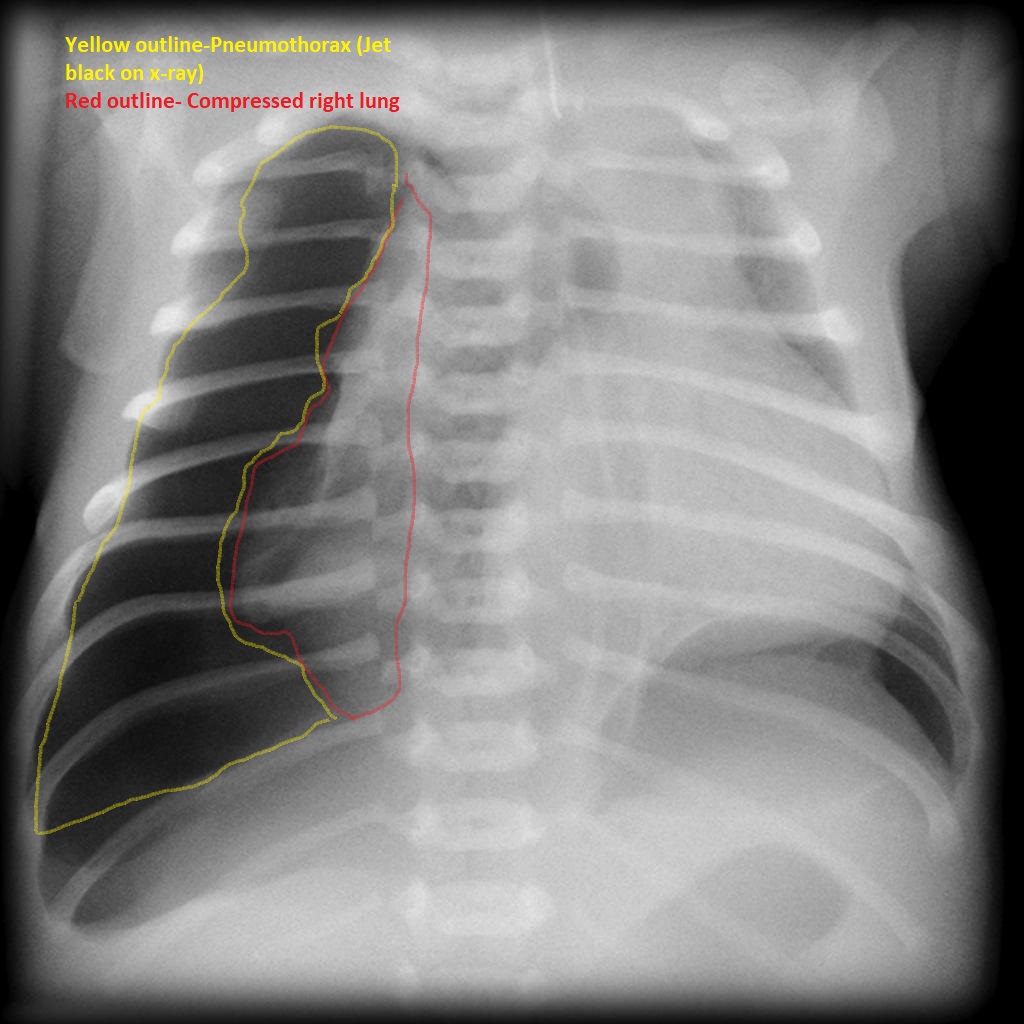
Tension pneumothorax: yellow outline = free pleural air (jet black on X-ray); red outline = compressed right lung pushed toward the mediastinum.
How to Distinguish Pleural Line from Artifacts
| Feature | True Pneumothorax | Skinfold / Artifact |
|---|---|---|
| Lucency | Both sides of the line | One side only |
| Line continuity | Sharp, traceable | Poorly defined, fades out |
| Chest wall conformity | Parallels chest wall curve | May extend beyond thorax |
| Vascular markings beyond line | Absent | Present |
| Shape | Convex toward lateral wall | Concave (bullae/cysts) |
Important mimics to exclude:
- Skinfold
- Edge of scapula
- Clothing/tubing artifact
- Avascular bullae or thin-walled cysts (inner margin concave, not convex toward chest wall)
- A bulla with a pleural adhesion can form a straight line mimicking a pneumothorax
When doubt exists, CT chest is definitive. - Fishman's Pulmonary Diseases
Expiratory Films
Several studies show expiratory films have little or no advantage over upright inspiratory films for diagnosing pneumothorax - this is a commonly taught but evidence-weak practice. However, if initial film is negative and suspicion is high, repeat imaging or POCUS/CT is more useful. - Fishman's Pulmonary Diseases
Sizing on CXR
Rough clinical methods:
- BTS method: distance from lung edge to chest wall at the hilum level - ≥2 cm = large pneumothorax
- Most clinicians estimate based on the amount of air at the apex and laterally
- CT is more accurate for volume estimation but rarely needed just for sizing
Sensitivity Comparison
| Modality | Notes |
|---|---|
| Upright CXR | Misses 17% of pneumothoraces |
| Supine CXR | Misses up to 80% |
| POCUS | More sensitive than supine CXR; rapid; operator-dependent |
| CT chest | Most sensitive; definitive; detects occult pneumothoraces |
Sources: Tintinalli's Emergency Medicine | Murray & Nadel's Textbook of Respiratory Medicine | Fishman's Pulmonary Diseases and Disorders | Grainger & Allison's Diagnostic Radiology | Roberts and Hedges' Clinical Procedures in Emergency Medicine
Managment
Finding Sources
Searching PubMed
pneumothorax management guidelines
Reading File
Reading File
Reading Article
PMID: 38806203
Reading Article
PMID: 40383767
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full management guide.
Management of Pneumothorax
The two goals of treatment are: (1) evacuate air from the pleural space and (2) prevent recurrence. - Rosen's Emergency Medicine
Treatment decisions are individualized based on: size of pneumothorax, severity of symptoms, presence of underlying lung disease, history of previous pneumothorax, patient reliability, availability of follow-up, and degree of air leak.
Step 1 - Identify the Type
| Type | Urgency | Default Initial Approach |
|---|---|---|
| Tension pneumothorax | Immediate emergency | Needle decompression → chest drain |
| Secondary spontaneous (SSP) | Urgent | Chest drain (nearly all patients) |
| Primary spontaneous, large / symptomatic | Semi-urgent | Needle aspiration or small-bore drain |
| Primary spontaneous, small / stable | Non-urgent | Observation ± supplemental O₂ |
| Iatrogenic / small traumatic | Variable | O₂ ± aspiration; drain if expanding |
| Mechanically ventilated patient | Urgent | Drain always (risk of tension) |
A. Tension Pneumothorax - Immediate Action
Do not delay for CXR. Diagnose and treat clinically.
1. Needle Decompression (emergency first step)
- Insert a large-bore needle (14-16G) into the pleural space
- Sites (either is acceptable per evidence):
- 2nd intercostal space, midclavicular line (2nd ICS MCL) - traditional ATLS site
- 4th/5th intercostal space, anterior axillary line (4-5th ICS AAL) - ATLS alternate / ETC preferred
- A 2025 meta-analysis (PMID 40383767) found a 32.84% failure rate for needle penetration into the pleural cavity with standard cannulas. A 7 cm needle is recommended to reduce failure. For left-sided tension pneumothorax, the 2nd ICS MCL is safer to avoid cardiac injury.
- Follow immediately with tube thoracostomy - needle decompression is a bridge only
2. Tube Thoracostomy
- Definitive treatment after needle decompression
- Connect to water-seal drainage system with suction
B. Primary Spontaneous Pneumothorax (PSP)
Small + Clinically Stable (< 2 cm on BTS / < 3 cm ACCP from apex)
- Observation + 100% supplemental oxygen via non-rebreather mask
- Intrinsic resorption rate: 1-2% per day on room air
- Supplemental O₂ accelerates resorption ~4-fold (O₂ absorbed 60x faster than N₂)
- Observe in ED for at least 4 hours; repeat CXR before discharge to confirm no worsening
- Discharge with strict return precautions + follow-up in 24-48 hours
- 2024 ERS/EACTS/ESTS guidelines: conditional recommendation for conservative care of minimally symptomatic, clinically stable PSP patients
Large (> 2-3 cm) OR Symptomatic OR Expanding
Option 1 - Needle Aspiration (preferred by 2024 ERS guidelines)
- 2024 ERS/EACTS/ESTS guidelines (PMID 38806203) make a strong recommendation for needle aspiration over chest tube drain as the initial treatment for PSP
- Technique:
- Thoracentesis kit (8 Fr catheter / 18G needle + three-way stopcock)
- Insert at 2nd ICS MCL or 4th-5th ICS anterior axillary line under local anaesthesia
- Aspirate with large syringe until resistance met; then remove catheter
- If > 2.5 L aspirated, suggests continuing air leak - proceed to tube
- More likely to succeed if: patient < 50 years, volume aspirated < 2.5 L
- No significant difference in immediate success between aspiration and tube drainage in RCTs (see table)
RCT comparison - Aspiration vs. Chest Tube Initial Success:
| Study | Year | N | Aspiration (%) | Chest Tube (%) |
|---|---|---|---|---|
| Harvey | 1994 | 73 | 80 | 100 |
| Andrivet | 1995 | 61 | 67 | 93 |
| Noppen | 2002 | 60 | 59 | 64 |
| Ayed | 2006 | 137 | 62 | 68 |
| Parlak | 2012 | 56 | 68 | 81 |
Murray & Nadel's Textbook of Respiratory Medicine
Option 2 - Small-bore chest tube / Pigtail catheter (8-14 Fr)
- If aspiration fails or is not feasible
- Pigtail catheters (Seldinger technique) have outcomes similar to small-bore tubes
- Complications: kinking, malposition, occlusion by blood/clot, failure with large air leak
Option 3 - Conservative (observation alone) for moderate-large PSP
- A recent RCT showed conservative management is non-inferior to drainage in uncomplicated moderate-large PSP, with a lower rate of serious adverse events
- Same RCT: conservatively managed patients had lower recurrence at 1 year than those receiving aspiration/drain - suggesting slow re-expansion may improve healing
- 2024 ERS guidelines also give a conditional recommendation for ambulatory management
Ambulatory Management (outpatient)
- A Heimlich valve attached to a small chest tube allows outpatient treatment
- Significantly reduced hospital stay (median 0 days vs. 4 days; P < 0.0001) vs. standard care
- Higher readmission rate but fewer total pleural procedures
C. Secondary Spontaneous Pneumothorax (SSP)
- Nearly all patients require tube thoracostomy - observation is rarely appropriate
- SSP carries higher physiological risk (limited pulmonary reserve) and higher recurrence risk
- Many will require thoracoscopy/thoracotomy + bleb stapling + pleurodesis
- Patients unfit for surgery (severe COPD, end-stage ILD): chemical pleurodesis or blood patch via the chest drain
D. Traumatic and Iatrogenic Pneumothorax
- Iatrogenic (post-thoracentesis, central line, needle biopsy): most managed with supplemental O₂ alone or simple aspiration; tube drain if these fail
- Traumatic (penetrating or blunt): usually requires tube drainage unless very small
- Hemopneumothorax: two tubes - one superior (air), one inferior (blood)
- Patients on PPV: drain all pneumothoraces regardless of size - risk of rapid progression to tension
E. Chest Tube Management Details
- Connect to a water-seal chamber drainage system
- Suction (20 cmH₂O): for persistent air leaks; suction not recommended by 2024 ERS guidelines routinely, but may help if lung not re-expanding
- Risk: rapid re-expansion pulmonary oedema (RPE); increased airflow through visceral defect may enlarge it
- When to wean: place on water seal only after air leak resolves
- When to remove: if no pneumothorax on CXR after water seal; or after 4-hour clamp trial + normal repeat film
- A 4-hour clamp is preferred over direct removal: easier to unclamp than to replace if pneumothorax recurs
- Loculated pneumothoraces: drain under ultrasound or CT guidance
F. Prevention of Recurrence - Pleurodesis and Surgery
Indications for Definitive Intervention
- 2nd or subsequent ipsilateral pneumothorax (recurrence rate ~50-60% after 2nd episode)
- Contralateral or synchronous bilateral pneumothorax
- Persistent air leak (PAL > 5-7 days)
- Occupation at risk (airline pilots, commercial divers) - even after 1st episode
- Failure of lung to expand with drain
- Patient preference after 1st PSP (shared decision-making)
Video-Assisted Thoracoscopic Surgery (VATS) - Gold Standard
- VATS with bleb/bulla stapling + mechanical or talc pleurodesis
- Recurrence prevention rate: ~95-100% (nearly 100% after surgical pleurodesis) - Harrison's 22E
- 2024 ERS guidelines: conditional recommendation for early surgical intervention for initial PSP in patients who prioritise recurrence prevention
- RCT data: VATS after 1st PSP showed 13% recurrence vs. 34% conservative management (Olesen et al.)
Medical (Chemical) Pleurodesis
- Agents: graded talc (most effective; 70-80% success), tetracycline, minocycline, autologous blood
- Instilled via chest tube or at thoracoscopy
- Preferred for patients who refuse or are not surgical candidates
- 2024 ERS guidelines: conditional recommendation for autologous blood patch in SSP patients with persistent air leak
Key Point on Suction vs. Seal
Current guidelines do not recommend routine suction. Water seal alone is preferred - evidence suggests conservative re-expansion may improve long-term outcomes.
G. Special Situations
| Situation | Management |
|---|---|
| Mechanically ventilated | Drain all (no observation); urgent; risk of tension even from small PTX |
| COPD patient | High risk for SSP; poor surgical candidate; consider medical pleurodesis |
| Cystic fibrosis | Indicates advanced disease; complex - involve specialist early |
| Catamenial pneumothorax | VATS + hormonal therapy; surgical management is mainstay |
| HIV / PCP | Underlying disease drives SSP; treat underlying infection + drain |
| Occult PTX on CT (no PPV) | Observation; no intervention needed; PPV converts plan to urgent drain |
| Stab wound | Repeat imaging at 4-6 hours even if initial CXR normal; 12% incidence of delayed PTX |
Quick Summary Algorithm
Pneumothorax confirmed
|
Tension signs? → YES → Needle decompression 2nd ICS MCL (7cm needle) → Tube drain
|
NO
|
On PPV? → YES → Tube drain (all sizes)
|
NO
|
Secondary (underlying lung disease)?
YES → Tube drain ± surgery/pleurodesis
|
NO (PSP)
|
Small + stable? → YES → O₂ + Observe 4h → Discharge + follow-up 24-48h
|
Large / symptomatic? → Needle aspiration (1st line, 2024 ERS) → if fails → Small-bore tube
|
Recurrent / PAL / failed? → VATS + pleurodesis
Sources: 2024 ERS/EACTS/ESTS Clinical Practice Guidelines (PMID 38806203) | 2025 Needle decompression meta-analysis (PMID 40383767) | Rosen's Emergency Medicine | Murray & Nadel's Textbook of Respiratory Medicine | Current Surgical Therapy 14e | Harrison's Principles of Internal Medicine 22E (2025)
This is a shared conversation. Sign in to Orris to start your own chat.