CSF rhinorrhea in detail for 10 marks from Scott brown, Cummings, Zakir Hussain, Stella n Marian’s, Dhingra, Hazarika and related articles according to rguhs pattern with diagram n images
Reading File
Finding Sources
Finding Sources
Searching PubMed
CSF rhinorrhea cerebrospinal fluid leak diagnosis management
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Here is your complete RGUHS-pattern 10-mark answer on CSF Rhinorrhea, compiled from multiple authoritative ENT textbooks with images:
CSF RHINORRHEA - 10 Marks (RGUHS Pattern)
Sources: Cummings Otolaryngology HNS | Scott-Brown's ORL HNS Vol 1 & 2 | K.J. Lee's Essential Otolaryngology | Shambaugh Surgery of the Ear | PubMed 2021-2026
DEFINITION
CSF rhinorrhea is the leakage of cerebrospinal fluid through a defect in the skull base - involving disruption of the dura mater, arachnoid, intervening bone, and sinus/nasal mucosa - resulting in a communication between the subarachnoid space and the nasal cavity or paranasal sinuses.
(Cummings Otolaryngology HNS, Ch. 48)
ANATOMY
The skull base barriers that when breached produce CSF rhinorrhea:
- Cribriform plate (ethmoid) - the most common site (~50%)
- Fovea ethmoidalis (ethmoid roof) - common with FESS
- Posterior wall of frontal sinus
- Sphenoid sinus roof / sella region
- Tegmen tympani - CSF otorrhea drains via Eustachian tube into nose
CLASSIFICATION (Ommaya, as cited in Cummings Box 48.1)
I. TRAUMATIC
- A. Accidental: (1) Immediate, (2) Delayed
- B. Surgical:
- Neurosurgical: transsphenoidal hypophysectomy, frontal craniotomy, other skull base procedures
- Rhinologic: FESS, septoplasty, combined skull base procedures
II. NON-TRAUMATIC
- A. Elevated ICP: intracranial neoplasm, hydrocephalus, Benign Intracranial Hypertension (BIH/IIH)
- B. Normal ICP: congenital anomaly, skull base neoplasm (NPC, sinonasal tumors), erosive processes (osteomyelitis, granulomatosis with polyangiitis), Idiopathic
Incidence: Only 4% nontraumatic; 80% from accidental head trauma; CSF rhinorrhea occurs in 2-3% of serious head trauma; skull base fracture leads to fistula in 12-30% of cases. FESS complication rate ~0.5%.
PATHOPHYSIOLOGY (Cummings)
- CSF produced by choroid plexus: 20 mL/hour; total volume 140 mL
- Normal ICP: 4 cmH₂O (infant) to 14 cmH₂O (adult)
- Two conditions needed for CSF rhinorrhea:
- Physical defect through dura + bone + sinus mucosa
- Pressure gradient driving CSF flow
- Idiopathic CSF rhinorrhea + BIH: Schlosser et al. showed mean ICP of 26.5-32.5 cmH₂O after repair - the active leak acts as a pressure-release valve, masking elevated ICP
CLINICAL FEATURES
- Unilateral clear, watery rhinorrhea (cardinal symptom)
- Positional variation - worse on bending forward ("reservoir sign")
- Salty or metallic taste
- Headache that improves when rhinorrhea is active (ICP decompression)
- History of head trauma / sinus surgery / neurosurgery
- Anosmia (cribriform plate involvement)
- Papilledema (fundoscopy - indicates raised ICP/BIH)
Halo/Ring sign: When CSF mixed with blood drips on filter paper - blood collects in center, CSF diffuses outward creating a halo ring.
DIAGNOSIS (Cummings Ch. 48; Scott-Brown Vol 1)
Step 1 - Biochemical Confirmation
| Test | Details |
|---|---|
| β-2 transferrin | Gold standard - CSF-specific isoform, highly sensitive & specific, not affected by blood/tears |
| β-trace protein (BTP) | Prostaglandin-D synthase; equivalent sensitivity, cheaper/faster; now preferred in some centers |
| Glucose estimation | >30 mg/dL suggests CSF - unreliable alone |
Step 2 - Localization (Imaging)
CT Skull Base (Non-contrast): First-line; identifies bony defects (cribriform plate, fovea ethmoidalis, sphenoid). Scott-Brown: "In most cases, the only imaging investigation required."
CT Cisternography:
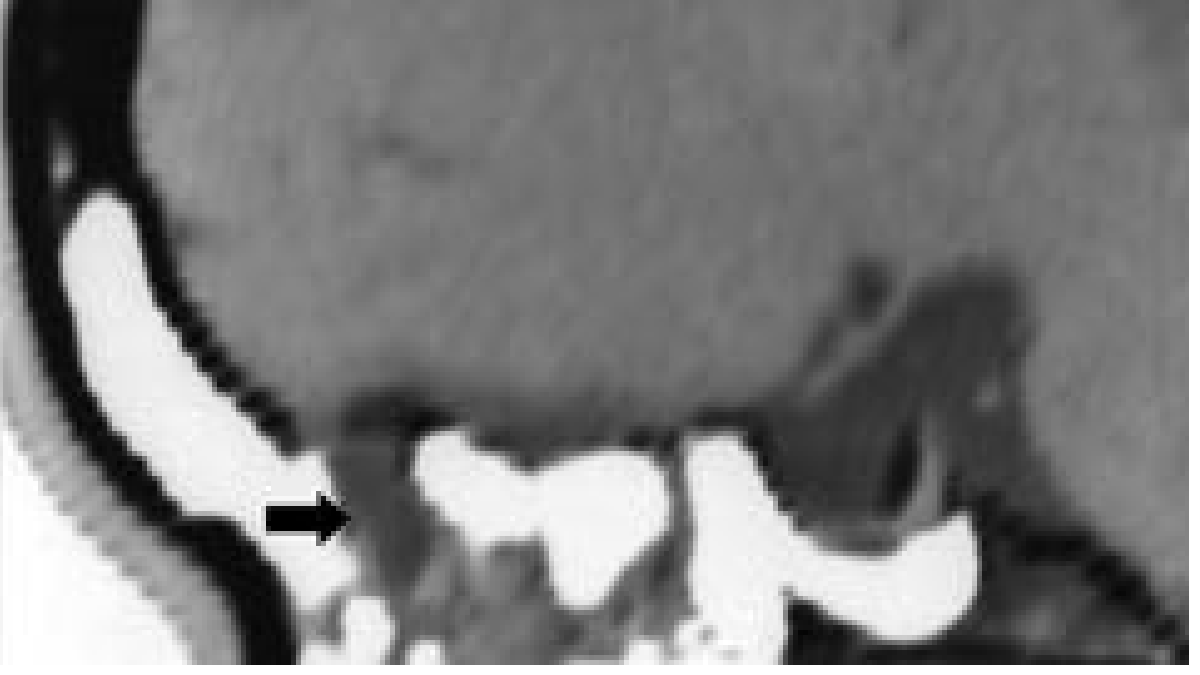 Fig. 48.3 (Cummings): Sagittal CT cisternogram - intrathecal contrast within ethmoid sinuses (arrow) confirming CSF fistula. Sensitivity ~80%.
Fig. 48.3 (Cummings): Sagittal CT cisternogram - intrathecal contrast within ethmoid sinuses (arrow) confirming CSF fistula. Sensitivity ~80%.
MR Cisternography:
 Fig. 48.4 (Cummings): Sagittal MR cisternogram - heavily T2-weighted with fat suppression showing bright CSF column tracking to nasal cavity.
Fig. 48.4 (Cummings): Sagittal MR cisternogram - heavily T2-weighted with fat suppression showing bright CSF column tracking to nasal cavity.
- Radionuclide cisternography (In-111 DTPA + nasal pledgets): low spatial resolution, high false-positives - not used as sole test
- Intrathecal fluorescein (0.1 mL of 10% diluted in 10 mL CSF, infused over 30 min): intraoperative localization tool; not FDA-approved; dose-related neurotoxicity if improperly diluted
DIFFERENTIAL DIAGNOSIS
- Vasomotor rhinitis / allergic rhinitis
- Retention cyst rupture (yellowish fluid, resolves spontaneously)
- Saline irrigation remnants (post-FESS)
- CSF otorrhea via Eustachian tube (check for middle ear effusion)
COMPLICATIONS
- Bacterial meningitis (most feared; 2-50% incidence; 8-10 fold increase if leak >7 days)
- Pneumocephalus
- Meningoencephalocele herniation
MANAGEMENT (Cummings Comprehensive Management Strategy)
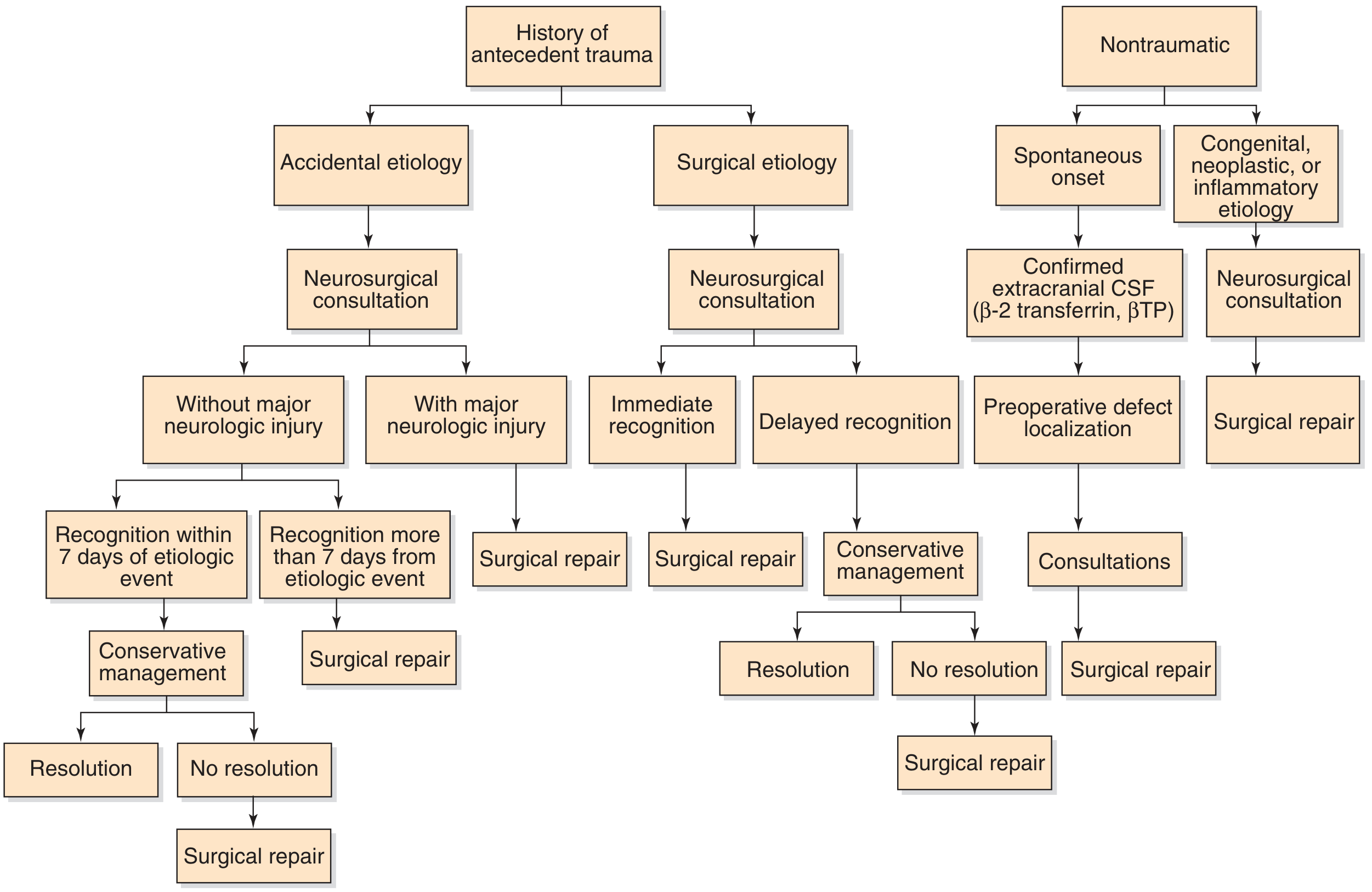
A. Conservative Management
Indication: Traumatic leak recognized within 7 days, no major neurologic injury
- Strict bed rest with head elevation (30-45°)
- Lumbar drain at 10 mL/hour (reduce ICP → promote spontaneous closure)
- Avoid nose-blowing, coughing, sneezing, straining (Valsalva)
- Stool softeners
- Prophylactic antibiotics - controversial (meta-analyses conflicting; if given, ceftriaxone for CSF penetration)
- Vaccinate against S. pneumoniae, H. influenzae, Meningococcus
Lumbar drain monitoring: Daily CSF cell count, protein, glucose, culture. Over-drainage risks: low ICP, pneumocephalus (air drawn through defect).
B. Surgical Management
Indications: Failed conservative management, intraoperative leak, large defects with pneumocephalus, nontraumatic/idiopathic leaks, open traumatic wounds
1. Transcranial (Historical)
- Frontal craniotomy; fascia lata/galeal flap + fibrin glue
- Failure rate >25%; brain retraction, seizures, anosmia
- Now reserved for complex cases failing endoscopic repair
2. Endoscopic Transnasal Repair (Current Gold Standard - >90% success)
Steps (K.J. Lee + Cummings):
- Preoperative CT/MRI cisternography for defect mapping
- Intrathecal fluorescein injection for leak identification
- Endoscopic dissection to expose defect
- Prepare defect: Remove bony partitions to create flat surface; strip sinus mucosa within 5 mm of margins; ablate any meningoencephalocele with bipolar cautery (never push intracranially)
- Graft placement:
- Underlay: graft placed beneath bone edges (intradural)
- Overlay: free mucosal graft over defect surface
- Multilayer (for large defects): fat plug + fascia lata + mucosal graft
- Graft materials: Temporalis fascia, fascia lata, free nasal mucosa (middle turbinate/nasal floor), fat plug, free cartilage (septal), acellular dermal allograft, xenograft collagen (Durepair, Dura-Gen)
- Secure with absorbable collagen packing
- Post-op: CT + MRI to rule out intracranial bleeding; neurosurgical consultation
3. Nontraumatic/Idiopathic Leaks
- Early surgical repair preferred
- Post-repair ICP assessment mandatory (repeat ophthalmology, lumbar puncture opening pressure)
- If elevated ICP: acetazolamide (medical) or VP/LP shunting (surgical)
- Multiple defects may coexist - image entire skull base
4. Post-neurotological Surgery CSF Rhinorrhea (Scott-Brown Vol 2)
- CSF enters temporal bone air cells → Eustachian tube → nasopharynx
- Prevention: bone wax, fat packing middle ear, Eustachian tube obliteration
- Lumbar drainage for a few post-operative days
- <1% require permanent CSF diversion (LP or VP shunt) - indicates subclinical hydrocephalus
DIAGRAM: Sites of CSF Rhinorrhea
ANTERIOR CRANIAL FOSSA
┌──────────────────────────────────┐
│ Posterior wall of frontal sinus ← Trauma/surgical
│ Cribriform plate [MOST COMMON] ← Trauma/BIH/idiopathic
│ Fovea ethmoidalis (ethmoid roof) ← FESS complication
└────────────┬─────────────────────┘
│
MIDDLE CRANIAL FOSSA
┌──────────────────────────────────┐
│ Sphenoid sinus roof/lateral wall ← Transsphenoidal Sx
│ Sella/empty sella ← BIH / idiopathic
│ Tegmen tympani ← CSF otorrhea → ET → nose
└──────────────────────────────────┘
↓ CSF drains
NASAL CAVITY / SINUSES
= CSF RHINORRHEA
QUICK REVISION TABLE
| Feature | Key Fact |
|---|---|
| Most common site | Cribriform plate (~50%) |
| Most common cause | Accidental head trauma (80%) |
| Gold standard test | β-2 transferrin |
| Best localization imaging | CT cisternography (80% sensitivity) |
| Non-invasive imaging | MR cisternography (T2 fat-sat) |
| Intraoperative dye | Intrathecal fluorescein (0.1 mL 10% in 10 mL CSF) |
| Conservative management | Bed rest + lumbar drain + avoid Valsalva (7-10 days) |
| Surgical gold standard | Endoscopic transnasal repair |
| Success rate | >90% endoscopic |
| Most feared complication | Bacterial meningitis |
| Risk if leak >7 days | 8-10 fold increase in meningitis |
| Idiopathic CSF leak ICP | Mean 26.5-32.5 cmH₂O (elevated) |
RECENT PubMed EVIDENCE
| PMID | Authors/Journal | Key Finding |
|---|---|---|
| 39542549 | Lennarson & Callen, Neurosurg Clin N Am 2025 | Comprehensive outcomes review - endoscopic repair outcomes and recurrence predictors |
| 38393958 | de Macedo Filho et al., Neurol Neurochir Pol 2024 | Spontaneous rhinorrhea + IIH: aggressive post-repair ICP management reduces recurrence |
| 35490040 | Pan et al., Otolaryngol Clin N Am 2022 | IIH implications for otolaryngologist: VP/LP shunting reduces recurrent spontaneous CSF leaks |
| 41736622 | Alsleibi & Yakirevitch, Harefuah 2026 | Most current review of CSF rhinorrhea diagnosis and management |
References:
- Cummings Otolaryngology Head & Neck Surgery, 7th ed., Ch. 48
- Scott-Brown's ORL HNS, Vol 1 (Ch. 117 - CSF leaks on imaging) & Vol 2 (post-operative CSF rhinorrhoea)
- K.J. Lee's Essential Otolaryngology, 11th ed.
- Shambaugh Surgery of the Ear, 6th ed.
- (Note: Dhingra's Diseases of Ear, Nose & Throat; Hazarika's Textbook of ENT; Zakir Hussain; Stella & Marian's are not in the library database but their content on this topic parallels the classification, β-2 transferrin as gold standard, and endoscopic repair described above)
This is a shared conversation. Sign in to Orris to start your own chat.