Please provide emphasis my notes for university exam, second year, ABVM University, under the heading Introduction, Location, Etiology, Pathogenesis, Types, and types must be in comparative table, Gross Microscopy, Clinical Feature.
Asking for Preferences
From harsh mohan book
Asking for Preferences
Emphysema
Reading File
Finding Sources
Searching the Web
Harsh Mohan emphysema pathology types etiology pathogenesis gross microscopy
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I have all the content needed. Here are your comprehensive exam notes on Emphysema, structured as requested.
EMPHYSEMA
Pathology Notes - 2nd Year | ABVM University
Source: Robbins & Cotran Pathologic Basis of Disease (standard reference, equivalent to Harsh Mohan)
1. INTRODUCTION
Emphysema is defined as irreversible enlargement of the airspaces distal to the terminal bronchiole, accompanied by destruction of alveolar walls, WITHOUT obvious fibrosis.
- It is one of the two major components of Chronic Obstructive Pulmonary Disease (COPD), the other being chronic bronchitis.
- Clinically significant obstruction occurs when respiratory bronchioles collapse during expiration due to loss of elastic recoil from destroyed alveolar walls.
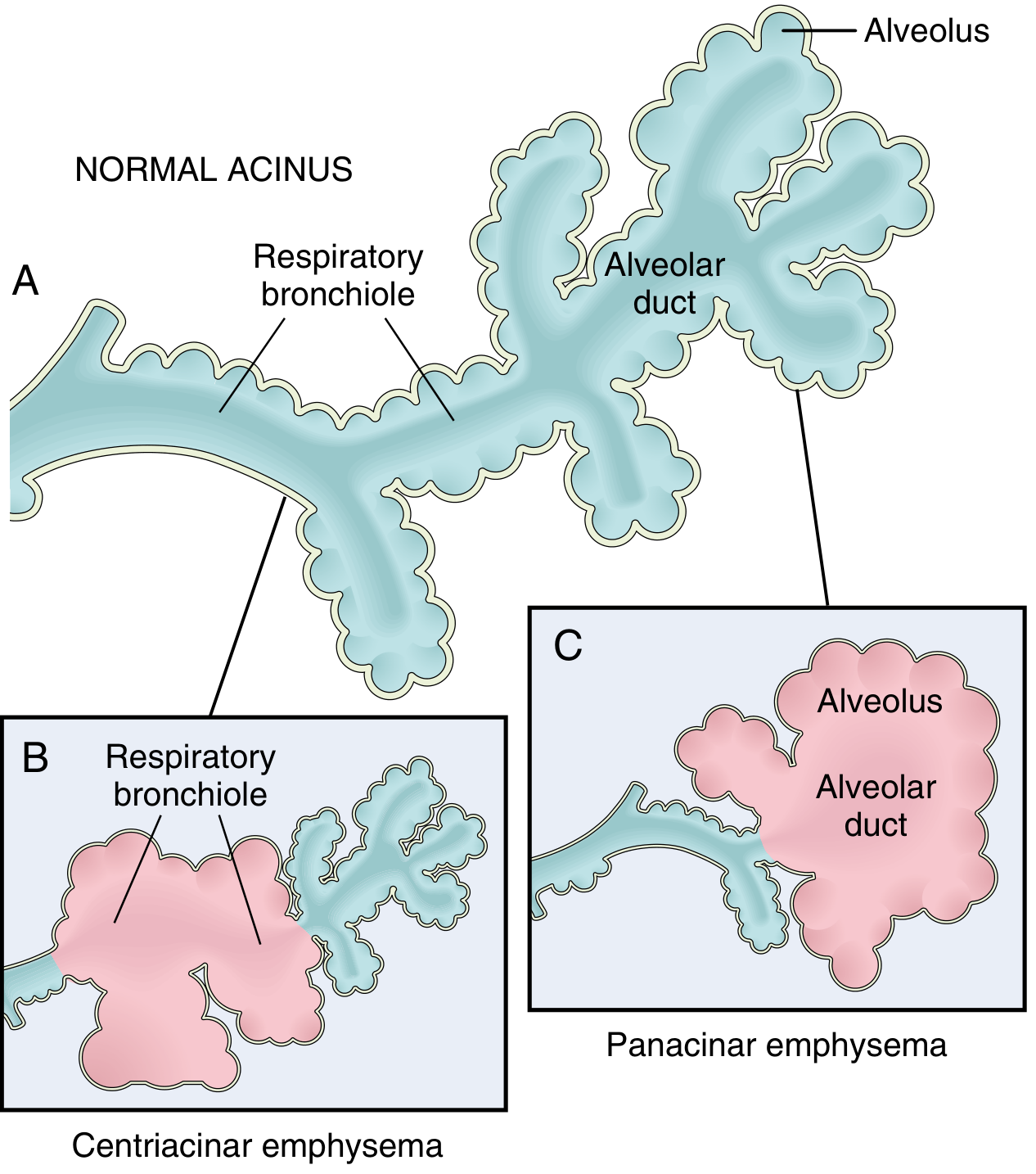
- The lobule is a cluster of acini (terminal respiratory units); emphysema is classified by which segment of the acinus is affected.
2. LOCATION
The location of emphysema within the lung depends on the type:
- Centriacinar - Upper lobes predominant, particularly apical segments; most common in smokers
- Panacinar - Lower zones and anterior margins; severe at the lung bases; associated with alpha-1 antitrypsin (AAT) deficiency
- Paraseptal (Distal acinar) - Adjacent to the pleura, along lobular connective tissue septa; upper half of lungs; near areas of fibrosis or atelectasis
- Irregular (Paracicatricial) - Anywhere, always associated with areas of scarring; usually small foci
3. ETIOLOGY
The two principal etiologic factors are:
A. Cigarette Smoking (Most Common)
- Responsible for the vast majority of clinically significant emphysema
- Causes toxic injury, inflammation, protease release, and oxidative stress to respiratory epithelium
- Nicotinic acetylcholine receptor variants may influence smoking addictiveness and thus lung cancer/emphysema risk
B. Alpha-1 Antitrypsin (AAT) Deficiency (Genetic)
- Congenital deficiency of the antiprotease AAT
- Leads to unopposed protease activity in the lung
- Causes panacinar emphysema; greatly exacerbated by smoking
- AAT is encoded on chromosome 14 (Pi locus); the severe Z allele produces a misfolded protein retained in hepatocytes
C. Other Contributing Factors
- Air pollutants and dust (grain, cotton, silica)
- Repeated pulmonary infections may acutely exacerbate existing disease (though not initiating)
- Other genetic variants linked to emphysema risk have been identified
4. PATHOGENESIS
The pathogenesis centers on protease-antiprotease imbalance compounded by oxidative stress and chronic inflammation.
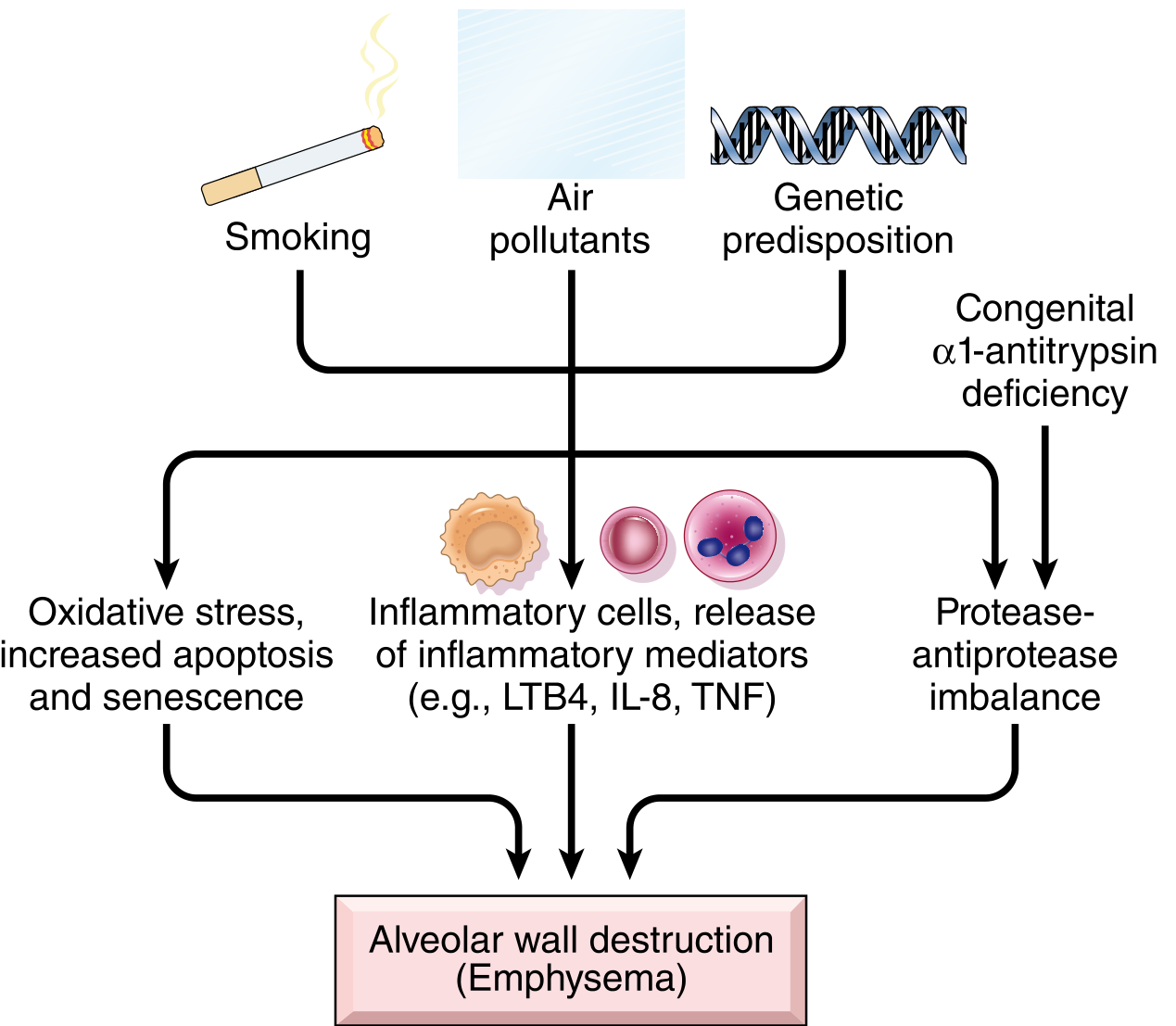
Step-by-step mechanism:
Step 1 - Toxic Injury and Inflammation
- Inhaled smoke/noxious particles damage respiratory epithelium
- Resident epithelial cells and macrophages release inflammatory mediators: LTB4, IL-8, TNF, and others
- These mediators attract inflammatory cells (neutrophils, macrophages), amplify inflammation, and induce structural changes
- Chronic inflammation accumulates T and B lymphocytes in affected lung
Step 2 - Protease-Antiprotease Imbalance
- Neutrophils and macrophages release proteases (mainly elastase, matrix metalloproteinases - MMPs) that break down connective tissue (elastin, collagen)
- Protective antiproteases are relatively deficient - in some patients this is genetic (AAT deficiency)
- Unchecked protease activity destroys alveolar walls
Step 3 - Oxidative Stress
- Tobacco smoke, alveolar damage, and inflammatory cells all produce reactive oxygen species (ROS)
- Oxidants cause direct tissue damage, endothelial dysfunction, and amplify inflammation
- NRF2 (encoded by NFE2L2) normally protects cells from oxidant damage; its impairment worsens susceptibility
- Mice lacking NRF2 are markedly more sensitive to tobacco smoke
Step 4 - Loss of Elastic Recoil
- Destruction of alveolar walls reduces elastic tissue
- Small airways lose radial traction from surrounding parenchyma
- Airways collapse during expiration → functional airflow obstruction
Step 5 - Infection (Exacerbating)
- Bacterial/viral infections do not initiate destruction but acutely worsen existing disease
5. TYPES - COMPARATIVE TABLE
| Feature | Centriacinar (Centrilobular) | Panacinar (Panlobular) | Paraseptal (Distal Acinar) | Irregular (Paracicatricial) |
|---|---|---|---|---|
| Part of acinus affected | Central/proximal - respiratory bronchioles | Entire acinus uniformly (respiratory bronchiole to terminal alveoli) | Distal acinus only; proximal spared | Irregular; varies |
| Association | Heavy cigarette smoking | Alpha-1 antitrypsin deficiency; worsened by smoking | Spontaneous pneumothorax in young adults; fibrosis/scarring | Scarring/fibrosis (always) |
| Location in lung | Upper lobes, apical segments | Lower zones, anterior margins; worst at lung bases | Adjacent to pleura; lobular septa; upper half of lungs | Anywhere near areas of scar |
| Frequency | Most common (>95% of clinically significant cases) | Less common; important in AAT deficiency | Uncommon; incidental finding | Common but usually clinically insignificant |
| Clinical significance | Significant airflow obstruction | Significant airflow obstruction | Often causes spontaneous pneumothorax; may form bullae | Usually NOT clinically significant |
| Coexistence | Both emphysematous and normal airspaces in same acinus | Uniform dilation; hard to distinguish from severe centriacinar | Multiple enlarged airspaces, 0.5 - 2.0 cm; cyst-like structures | Associated with focal scarring |
6. GROSS AND MICROSCOPIC FEATURES
Gross (Macroscopic) Appearance
- Voluminous, overinflated lungs - Lungs overlap the heart anteriorly on gross examination
- Flattened diaphragm - Due to air trapping and hyperinflation
- Large visible alveoli on the cut surface of fixed lungs
- Apical blebs and bullae - Characteristic of irregular (paraseptal) emphysema; prominent in advanced disease; bullae are air spaces >1 cm in diameter
- Upper two-thirds of lungs more severely affected in smoking-related disease
Microscopic (Histological) Appearance
- Abnormally large, dilated alveoli separated by thin septa
- Focal centriacinar fibrosis within the thin septa
- Loss of alveolar wall attachments to the outer wall of small airways
- Enlarged pores of Kohn - So large that the septa appear to be "floating" or protruding blindly into alveolar spaces with club-shaped ends
- Decreased capillary bed area due to alveolar wall destruction
- In advanced disease: even larger abnormal airspaces, bullae that compress respiratory bronchioles and vasculature
- Superimposed inflammatory changes in small airways (from coexisting chronic bronchitis)
- Vascular changes of pulmonary hypertension - Due to local hypoxemia and loss of capillary beds
7. CLINICAL FEATURES
Emphysema presents as part of COPD. The classic presentation is:
Symptoms
- Progressive exertional dyspnea - The dominant complaint; insidious onset
- Minimal or no cough (in pure emphysema, unlike chronic bronchitis)
- Little to no sputum production
- Weight loss in advanced disease
Classic "Pink Puffer" appearance (typical of pure emphysema)
- Barrel chest - Increased AP diameter from air trapping
- Pursed-lip breathing - Maintains positive end-expiratory pressure to prevent airway collapse
- Accessory muscle use
- Prolonged expiratory phase
- Relatively well-oxygenated (pink) due to increased respiratory effort maintaining PaO2
- Tachypnea (rapid breathing rate)
Physical Signs
- Hyperresonance on percussion
- Diminished breath sounds bilaterally
- Decreased chest expansion
- Low, flat diaphragm (seen on CXR)
Complications
- Spontaneous pneumothorax - Especially with paraseptal/bullous emphysema when a bulla ruptures
- Pulmonary hypertension - From hypoxic vasoconstriction and capillary bed loss
- Cor pulmonale (right heart failure) - From chronic pulmonary hypertension
- Secondary polycythemia - From chronic hypoxemia stimulating erythropoietin
- Respiratory failure in end-stage disease
Pulmonary Function Tests (PFTs)
- Reduced FEV1/FVC ratio (<70%) - Obstructive pattern
- Increased TLC, RV (air trapping)
- Reduced DLCO (diffusing capacity) - Due to loss of alveolar-capillary surface area
Exam Tip: Remember that only Centriacinar and Panacinar types cause clinically significant airflow obstruction. Paraseptal causes spontaneous pneumothorax; Irregular is usually clinically silent. The key mechanism is protease-antiprotease imbalance - always highlight this in exams.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 635-636
This is a shared conversation. Sign in to Orris to start your own chat.