Niacinamide
Reading File
Searching the Web
niacinamide pharmacology clinical uses mechanism 2025
Finding Sources
Searching PubMed
niacinamide nicotinamide clinical applications
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a detailed overview of Niacinamide (Nicotinamide / Vitamin B3) compiled from authoritative medical textbooks:
Niacinamide (Nicotinamide) - Vitamin B3
Chemical Identity & Structure
Niacinamide is the amide form of niacin (pyridine-3-carboxylic acid). It is distinct from nicotinic acid in that it carries an -NH₂ group instead of -OH on the carboxyl. Both are collectively called "niacin" or vitamin B3.
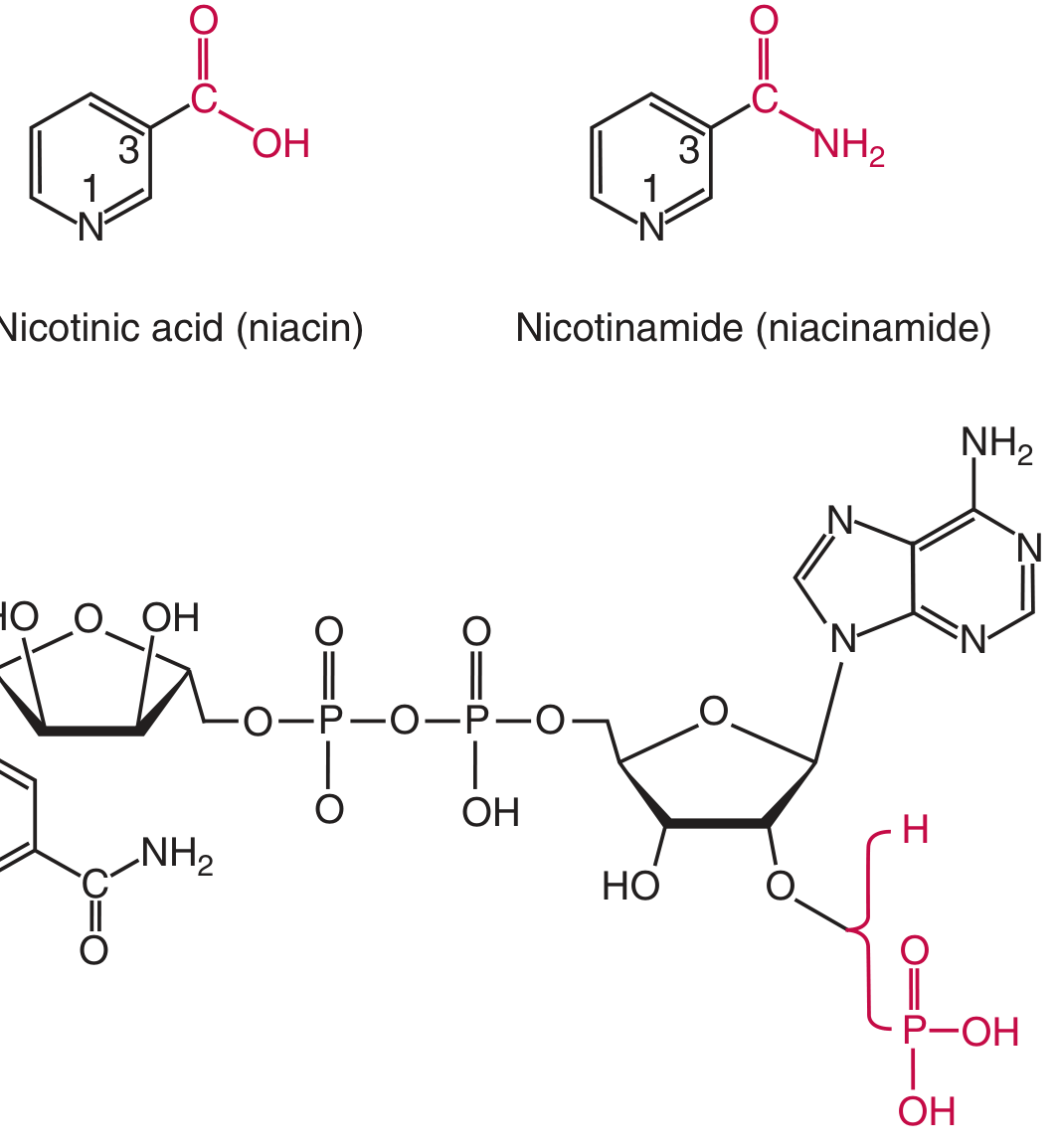
Chemical structures of nicotinic acid, niacinamide, and NAD (Tietz Textbook of Laboratory Medicine, 7th Ed)
Pharmacokinetics
- Absorption: Dietary NAD and NADP are hydrolyzed by intestinal NAD glycohydrolase to release nicotinamide, which is absorbed in the stomach and small intestine by Na+-dependent facilitated diffusion at low concentrations and passive diffusion at higher concentrations.
- Circulation: Nicotinamide is the main circulating form in plasma.
- Metabolism: Inside cells (liver, kidney, brain), nicotinamide is converted to NAD and NADP via phosphoribosyltransferase reactions. NADP is then formed by kinase-catalyzed phosphorylation of NAD.
- Excretion: Excess is methylated in the liver to N-methylnicotinamide (NMN) and excreted in urine, along with its oxidation products (N-methyl-2-pyridone-5-carboxamide and N-methyl-4-pyridone-carboxamide).
- Storage: Minimal storage occurs in the body.
(Tietz Textbook of Laboratory Medicine, 7th Ed)
Biochemical Functions
- NAD/NADH & NADP/NADPH co-enzyme activity - Niacinamide is incorporated into NAD+ and NADP+, which act as hydrogen/electron carriers in hundreds of redox reactions: glycolysis, fatty acid synthesis and oxidation, the TCA cycle, and amino acid metabolism.
- DNA repair via PARP-1 - NAD is a substrate for poly(ADP-ribose) polymerase-1 (PARP-1), an enzyme critical for base excision repair and genomic stability. This is why nicotinamide deficiency impairs DNA repair.
- Cellular energy - Prevents ATP depletion, particularly under UV radiation stress in keratinocytes.
(Tietz Textbook of Laboratory Medicine, 7th Ed; Scott-Brown's Otorhinolaryngology)
Dietary Sources & Requirements
- Rich sources: meat, fish, liver, eggs, mushrooms, nuts, legumes, dairy, whole grains.
- Tryptophan is a precursor: ~60 mg tryptophan yields 1 mg niacin equivalent (NE). Up to two-thirds of adult niacin requirements can be derived from tryptophan.
- Bound niacin in corn/maize (niacytin) is nutritionally unavailable without alkaline hydrolysis (e.g., lime-water treatment used in Mexican cuisine - "nixtamalization").
(Tietz Textbook of Laboratory Medicine, 7th Ed; Fitzpatrick's Dermatology)
Deficiency: Pellagra
Classic "4 Ds": Dermatitis, Diarrhea, Dementia, Death
- Caused by inadequate niacin AND tryptophan intake, or impaired conversion.
- At-risk populations: populations subsisting on untreated maize (parts of South Africa, India, China); alcoholism; isoniazid therapy (blocks B6 needed for tryptophan conversion); malabsorptive GI diseases; carcinoid syndrome (tryptophan diverted to serotonin).
- Treatment: Nicotinamide 100 mg three times daily (oral or parenteral) to correct malnutrition; animal proteins, eggs, milk, and vegetables alongside supplementation.
(Fitzpatrick's Dermatology; Andrews' Diseases of the Skin; Bradley and Daroff's Neurology)
Clinical Uses
1. Chemoprevention of Non-Melanoma Skin Cancer (NMSC)
- Dose: 500 mg orally twice daily for 12 months
- A large randomized Phase III trial showed a 23% lower rate of newly formed NMSC (both SCC and BCC) compared with placebo, with a favorable safety profile.
- Mechanism: prevents UV-induced NAD depletion in keratinocytes, restores cellular energy, enhances DNA repair, and inhibits UV-induced immunosuppression.
- Also significantly reduces actinic keratoses in high-risk patients.
- Note: in immunosuppressed organ-transplant recipients, benefit was not demonstrated.
(Fitzpatrick's Dermatology, Vol 1-2; Dermatology 2-Volume Set 5e; Scott-Brown's)
2. Acne Vulgaris (Topical)
- 4% nicotinamide gel is available OTC and is as effective as clindamycin 1% gel (non-inferior) for moderate inflammatory acne in comparative studies.
- 2% nicotinamide cream reduces sebum production and improves facial shine/oiliness within 4-6 weeks.
- Mechanism: anti-inflammatory (reduces IL-1, IL-6, TNF-alpha release), sebostatic, and increases ceramide production to reinforce skin barrier.
(Dermatology 2-Volume Set 5e; Scott-Brown's; Fitzpatrick's Dermatology)
3. Hyperpigmentation & Photoaging
- 5% nicotinamide cream applied twice daily for 12 weeks in a split-face study improved fine lines, wrinkles, hyperpigmented spots, redness, sallowness, and skin elasticity.
- Mechanism: inhibits melanosome transfer from melanocytes to keratinocytes (interferes with the Pak1 signaling pathway), without directly inhibiting tyrosinase (contrast with hydroquinone or vitamin C).
- Often combined with 2% N-acetyl glucosamine; a double-blind RCT (n=202) found this combination significantly reduced facial spots and pigmentation vs. vehicle.
(Scott-Brown's Otorhinolaryngology; Indian Journal of Dermatology)
4. Glaucoma (Investigational)
- Clinical trials have commenced to evaluate whether supplementary nicotinamide is neuroprotective in glaucoma patients, given its role in maintaining cellular NAD+ levels in retinal ganglion cells.
(Kanski's Clinical Ophthalmology, 10th Ed)
5. Dyslipidemia (Nicotinic Acid - Note the Distinction)
- At pharmacologic doses, nicotinic acid (not niacinamide) is used for dyslipidemia. Niacinamide does not cause flushing or have lipid-lowering effects because it does not activate the GPR109A (HM74A) receptor on adipocytes and Langerhans cells that nicotinic acid activates.
(Katzung's Basic and Clinical Pharmacology, 16th Ed; Tietz Textbook of Laboratory Medicine)
Key Distinction: Niacinamide vs. Nicotinic Acid
| Property | Niacinamide | Nicotinic Acid |
|---|---|---|
| Flushing | No | Yes (prostaglandin-mediated) |
| Lipid lowering | No | Yes (TG↓, HDL↑, LDL↓) |
| DNA repair / PARP-1 inhibition | Yes | Less prominent |
| Anti-inflammatory / anti-acne | Yes (topical) | Not used topically |
| Skin cancer chemoprevention | Yes | Not established |
Safety Profile
- Well-tolerated orally at 500 mg twice daily (standard chemoprevention dose).
- Does not cause the cutaneous flushing seen with nicotinic acid.
- High oral doses (>3 g/day) can cause hepatotoxicity, nausea, and hyperglycemia, but these are uncommon at therapeutic dermatological doses.
- Topically (2-5%): excellent safety record, non-irritating, suitable for sensitive skin.
Sources: Fitzpatrick's Dermatology (Vol 1-2) | Dermatology 2-Volume Set 5e | Scott-Brown's Otorhinolaryngology | Tietz Textbook of Laboratory Medicine 7th Ed | Kanski's Clinical Ophthalmology 10th Ed | Katzung's Basic and Clinical Pharmacology 16th Ed | Harper's Illustrated Biochemistry 32nd Ed
This is a shared conversation. Sign in to Orris to start your own chat.