# Physiology of Functional Types of Movements in the GI Tract & Splanchnic Circulation --- ## PART 1: FUNCTIONAL TYPES OF GI MOVEMENTS The gastrointestinal tract performs two fundamental types of movements: 1. **Mixing movements** 2. **Propulsive movements** Both are modifications of the basic contractile activity of GI smooth muscle. --- ## BASIC ELECTRICAL ACTIVITY OF GI SMOOTH MUSCLE Before understanding movements, we must understand the electrical basis: ### Slow Waves (Basic Electrical Rhythm - BER) - **Not true action potentials** — they are rhythmic, undulating changes in resting membrane potential - Generated by the **Interstitial Cells of Cajal (ICC)**, which act as the **pacemaker cells** of the GI tract - ICC are located between the longitudinal and circular muscle layers (at the level of the myenteric plexus) and also within the circular muscle layer - Slow wave frequency varies by region: - **Stomach (body/antrum):** 3 per minute - **Duodenum:** 12 per minute (highest frequency in the GI tract) - **Ileum:** 8-9 per minute - **Cecum/colon:** 2-6 per minute (gradient from cecum to sigmoid) - Slow waves **do not cause contraction by themselves** (except in the stomach where they can cause weak contractions). They merely set the **timing** and **maximum frequency** of contractions - Mechanism: Cyclic opening of non-selective cation channels → Na⁺ influx → depolarization; then repolarization by K⁺ efflux ### Spike Potentials (Action Potentials) - True action potentials superimposed on slow waves - Occur when the slow wave depolarization reaches **threshold** (approximately -40 mV) - Duration: **10-40 ms** (much longer than nerve/skeletal muscle action potentials of 1-2 ms) - Ionic basis: **Calcium-sodium channels** (slow channels) — Ca²⁺ influx is the major depolarizing current (not Na⁺ as in skeletal muscle) - This is why GI smooth muscle contraction depends heavily on extracellular Ca²⁺ - K⁺ efflux causes repolarization - The **number of spike potentials** on a slow wave determines the **strength of contraction** (more spikes = more Ca²⁺ entry = stronger contraction) ### Factors That Affect Spike Generation **Factors that DEPOLARIZE (increase excitability):** - Stretching of the muscle - Acetylcholine (parasympathetic stimulation) - Substance P - GI-specific stimulating hormones (gastrin, CCK, motilin) **Factors that HYPERPOLARIZE (decrease excitability):** - Norepinephrine (sympathetic stimulation) - Epinephrine - VIP, Secretin, GIP - Nitric oxide ### Clinical Correlation: Hirschsprung's Disease (Congenital Megacolon) - **Pathology:** Absence of ganglion cells (both myenteric and submucosal plexus) in a segment of the distal colon (usually rectosigmoid) due to failure of neural crest cell migration - Also involves absence or dysfunction of ICC in the aganglionic segment - The aganglionic segment remains **tonically contracted** (because the normal inhibitory innervation via NO and VIP is absent) - The **proximal** normal colon dilates massively (megacolon) - **Presentation:** Failure to pass meconium within 48 hours of birth, abdominal distension, bilious vomiting - **Diagnosis:** Rectal suction biopsy (absence of ganglion cells), barium enema (transition zone), anorectal manometry (absence of rectoanal inhibitory reflex — RAIR) - **Treatment:** Surgical pull-through procedure (Soave, Swenson, or Duhamel) --- ## PROPULSIVE MOVEMENTS — PERISTALSIS ### Definition Peristalsis is an **organized, wave-like pattern** of contraction and relaxation that propels a bolus of food in the **aboral (aborad) direction** — from mouth toward anus. ### Mechanism (Law of the Intestine / Law of the Gut / Myenteric Reflex) This was first described by **Bayliss and Starling** in 1899. When a bolus distends the gut at any point: 1. **Behind the bolus (orad side):** - Stretch activates sensory neurons (IPANs — intrinsic primary afferent neurons) in the myenteric plexus - These activate excitatory motor neurons - Excitatory neurotransmitters: **Acetylcholine** and **Substance P** - Result: **Contraction of circular muscle** (constriction) behind the bolus — the "propulsive segment" - Simultaneously, the longitudinal muscle relaxes (shortens the segment) 2. **Ahead of the bolus (aborad side):** - Inhibitory motor neurons are activated - Inhibitory neurotransmitters: **Nitric oxide (NO)**, **VIP (Vasoactive Intestinal Peptide)**, and **ATP** - Result: **Relaxation of circular muscle** ahead of the bolus — the "receiving segment" - Simultaneously, the longitudinal muscle contracts (the gut shortens to "receive" the bolus) This creates a **pressure gradient** that pushes the bolus forward. ### Characteristics of Peristalsis - **Unidirectional:** Normally proceeds only in the oral-to-anal direction (anterograde). This directional polarity is called **the law of the intestine** and is an inherent property of the enteric nervous system - **Velocity:** Varies by region: - Esophagus: 3-5 cm/sec (fastest) - Stomach: 1 cm/sec - Small intestine: 0.5-2 cm/sec - Colon: Very slow, usually a few cm/sec during mass movements - **Stimulus:** The most important natural stimulus is **distension** of the gut wall - **Dies out after traveling a variable distance** — usually a few centimeters in the small intestine (unlike esophageal peristalsis which traverses the entire length) - **Requires an intact myenteric plexus** — the enteric nervous system is essential. If the myenteric plexus is destroyed (e.g., by nicotine, Chagas disease), peristalsis is abolished or severely impaired ### Types of Peristalsis in Different Regions #### Esophageal Peristalsis **Primary Peristalsis:** - Continuation of the pharyngeal phase of swallowing - Initiated by the **swallowing center** in the medulla (deglutition center) - Travels the entire length of the esophagus in 8-10 seconds - Upper 1/3 (striated muscle): Controlled by sequential activation via **vagus nerve (nucleus ambiguus)** - Lower 2/3 (smooth muscle): Controlled by **myenteric plexus** with vagal modulation - Wave speed: 3-5 cm/sec **Secondary Peristalsis:** - Initiated by **local distension** of the esophageal wall (e.g., retained food bolus) - Does NOT require a swallowing reflex; purely a local reflex via intrinsic neurons - Continues until esophagus is cleared - Important for clearing refluxed gastric contents **Tertiary Contractions (Non-peristaltic):** - Simultaneous, disorganized contractions - **NOT propulsive** - Considered **pathological** in younger individuals; may be normal in elderly - Seen in **diffuse esophageal spasm** ### Clinical Correlation: Achalasia - **Pathology:** Loss of inhibitory neurons (NO and VIP-producing neurons) in the myenteric plexus of the lower esophageal sphincter (LES) and distal esophagus - Also involves loss of ganglion cells in the Auerbach's plexus - **Result:** - Failure of LES relaxation with swallowing - Aperistalsis of the esophageal body (loss of coordinated peristalsis in the smooth muscle segment) - Increased resting LES pressure - **Symptoms:** Progressive dysphagia to both solids AND liquids (unlike mechanical obstruction which is initially solids only), regurgitation of undigested food, chest pain, weight loss - **Diagnosis:** - **Barium swallow:** "Bird's beak" or "rat tail" appearance at the GEJ, dilated esophagus (megaesophagus) - **Esophageal manometry** (Gold standard): Aperistalsis, incomplete LES relaxation, elevated resting LES pressure - **Endoscopy:** To rule out pseudoachalasia (malignancy at the GEJ) - **Treatment:** Pneumatic balloon dilation, Heller myotomy (laparoscopic), Peroral endoscopic myotomy (POEM), botulinum toxin injection into LES (temporary) - **Complication:** Increased risk of **squamous cell carcinoma** of the esophagus (due to chronic stasis and irritation) ### Clinical Correlation: Chagas Disease (American Trypanosomiasis) - Caused by **Trypanosoma cruzi** (transmitted by reduviid bug — "kissing bug") - The parasite destroys **myenteric plexus neurons** → secondary achalasia, megaesophagus, megacolon - Endemic in Central and South America - Also causes dilated cardiomyopathy ### Clinical Correlation: Diffuse Esophageal Spasm - Simultaneous, high-amplitude, non-peristaltic contractions of the esophageal body - Manometry: Simultaneous contractions in >20% of swallows (with some normal peristalsis — distinguishes from achalasia) - Barium swallow: "**Corkscrew esophagus**" or "rosary bead" esophagus - Symptoms: Intermittent dysphagia and severe chest pain (can mimic angina) - Treatment: Calcium channel blockers (nifedipine), nitrates, tricyclic antidepressants --- #### Gastric Peristalsis - Peristaltic waves originate from the **pacemaker zone** located in the **mid-body** of the stomach on the greater curvature - Frequency: **3 waves per minute** (set by the slow wave frequency) - Waves become progressively **stronger and faster** as they move toward the pylorus - The antrum has the strongest contractions - Functions: 1. **Mixing** of food with gastric secretions → formation of **chyme** 2. **Grinding** of food particles (antral mill — see below) 3. **Propulsion** of chyme through the pylorus **Gastric Emptying and the Antral Pump/Mill:** - As the peristaltic wave approaches the pylorus, the pylorus closes - The bolus of chyme is forced back into the body of the stomach (**retropulsion**) - This creates powerful **mixing and grinding** — the **antral mill** - Only particles smaller than **1-2 mm** can pass through the pylorus into the duodenum - The rate of gastric emptying is controlled by: - **Gastric factors:** Volume of gastric contents (more volume = faster emptying), gastrin - **Duodenal factors (feedback inhibition):** - Fat in duodenum (most potent inhibitor) → releases CCK, GIP → slows gastric emptying - Acid in duodenum → releases secretin → slows gastric emptying - Hypertonicity/hypotonicity in duodenum → osmoreceptors → slows emptying - Protein digestion products - Distension of duodenum These duodenal factors act via: - **Enterogastric reflex** (neural — both intrinsic ENS and extrinsic vagal/sympathetic) - **Hormones:** CCK, secretin, GIP, peptide YY — all inhibit gastric motility and emptying **Liquids empty faster than solids; carbohydrates fastest, then proteins, then fats (fats slowest)** ### Clinical Correlation: Gastroparesis - **Definition:** Delayed gastric emptying without mechanical obstruction - **Causes:** - **Diabetic gastroparesis** (most common cause) — due to vagal neuropathy (autonomic neuropathy from chronic hyperglycemia) and damage to ICC - Post-surgical (vagotomy) - Idiopathic (second most common) - Medications (opioids, anticholinergics, GLP-1 agonists) - Parkinson's disease, scleroderma, amyloidosis - **Symptoms:** Early satiety, nausea, vomiting (often of undigested food eaten hours/days earlier), bloating, upper abdominal pain, weight loss - **Diagnosis:** - **Gastric emptying scintigraphy** (gold standard): Patient eats a radiolabeled meal (usually egg sandwich with technetium-99m sulfur colloid); retention of >10% at 4 hours is diagnostic - Upper endoscopy to rule out obstruction - **Treatment:** - Dietary: Small, frequent, low-fat, low-fiber meals; liquid nutrition - Prokinetic agents: **Metoclopramide** (dopamine D2 antagonist + 5-HT4 agonist — accelerates gastric emptying; crosses BBB → extrapyramidal side effects, tardive dyskinesia), **Domperidone** (D2 antagonist, doesn't cross BBB, fewer CNS side effects), **Erythromycin** (motilin receptor agonist — most potent prokinetic, but tachyphylaxis limits long-term use) - Gastric electrical stimulation (Enterra device) - Pyloromyotomy (G-POEM) ### Clinical Correlation: Dumping Syndrome - Occurs after gastric surgery (gastrectomy, pyloroplasty, gastric bypass) - **Early dumping** (within 15-30 minutes of eating): Rapid emptying of hyperosmolar chyme into small intestine → osmotic fluid shift into gut lumen → hypovolemia, distension → cramping, diarrhea, nausea, tachycardia, diaphoresis, dizziness - **Late dumping** (1-3 hours after eating): Rapid glucose absorption → exaggerated insulin release → reactive hypoglycemia → tremor, weakness, sweating, confusion - **Treatment:** Small, frequent meals; avoid simple carbohydrates; lie down after meals; octreotide (somatostatin analog) in refractory cases --- #### Small Intestinal Peristalsis - Normal peristalsis in the small intestine moves chyme at **0.5-2 cm/sec** - Each peristaltic wave **dies out after 3-5 cm** — this means transit through the entire small intestine (6-7 meters) takes **3-5 hours** - Peristalsis is **markedly increased** after a meal — this is the **gastroileal reflex** (gastric distension enhances ileal motility and relaxes the ileocecal valve via vagus nerve and gastrin) - Peristaltic activity is enhanced by: - **Gastrin, CCK, motilin, insulin, serotonin (5-HT)** - Parasympathetic (vagal) stimulation - Peristaltic activity is inhibited by: - **Secretin, glucagon** - Sympathetic stimulation **Peristaltic Rush:** - A powerful peristaltic wave that travels long distances rapidly (may traverse entire small intestine in minutes) - Caused by intense irritation of the intestinal mucosa (e.g., infectious enteritis, castor oil) - Represents a **protective mechanism** to sweep irritating/infectious material quickly through the gut - Results in **diarrhea** (material moves too fast for adequate absorption) ### Clinical Correlation: Paralytic Ileus (Adynamic Ileus) - **Definition:** Temporary cessation of peristalsis in the absence of mechanical obstruction - **Causes:** - **Post-surgical** (most common — especially after abdominal surgery; due to handling of bowel, anesthesia, opioid analgesics) - Peritonitis, pancreatitis, retroperitoneal hemorrhage - Hypokalemia (impairs smooth muscle contractility) - Hypomagnesemia - Opioid use (activate μ-receptors on myenteric neurons → inhibit ACh release) - Anticholinergic drugs - Spinal cord injury, traumatic brain injury - **Presentation:** Abdominal distension, absent bowel sounds, no passage of flatus/stool, nausea, vomiting - **Diagnosis:** Abdominal X-ray shows diffusely dilated loops of bowel (both small and large) with air-fluid levels; no transition point (unlike mechanical obstruction) - **Treatment:** - NPO, nasogastric decompression, IV fluids, electrolyte correction - Minimize opioids; use NSAIDs for pain - **Alvimopan** (peripheral μ-opioid receptor antagonist — accelerates recovery of bowel function after surgery; does not cross BBB so doesn't reverse central analgesia) - **Methylnaltrexone** (peripheral μ-opioid antagonist) for opioid-induced constipation - **Neostigmine** (acetylcholinesterase inhibitor) — especially useful for **Ogilvie's syndrome** (acute colonic pseudo-obstruction) - Early ambulation, chewing gum (sham feeding stimulates vagal-mediated GI motility) ### Clinical Correlation: Mechanical Intestinal Obstruction - Unlike ileus, there IS a physical obstruction - **Small bowel obstruction (SBO):** Most common cause = **adhesions** (from prior surgery), hernias, tumors - **Large bowel obstruction (LBO):** Most common cause = **colorectal carcinoma**, volvulus, diverticulitis - Above the obstruction: Vigorous peristalsis (hyperperistalsis) → high-pitched, tinkling bowel sounds, "rushes" - Below the obstruction: Quiet/absent bowel sounds - **Can lead to:** Bowel ischemia, perforation, sepsis, death --- #### Colonic Peristalsis The colon exhibits special types of propulsive movements: **1. Haustral Contractions (Haustrations):** - These are the **primary mixing movements** of the colon (but also have a slow propulsive component) - The circular muscle contracts in isolated segments creating **haustra** (sacculations) - Slow, sluggish contractions - Also called "segmentation" of the colon - Move contents slowly — contribute to the **12-24 hours** transit time through the colon - Allow maximum absorption of water and electrolytes **2. Mass Movements (Mass Peristalsis):** - A **modified type of peristalsis** unique to the colon - A constrictive ring forms (usually in the transverse colon), and a long segment distal to it (20 cm or more) contracts as a unit, forcing fecal material en masse toward the rectum - **Duration:** The contraction builds up over ~30 seconds, lasts about 2-3 minutes, then relaxes for a variable period before occurring again - **Frequency:** Occurs only **1-3 times per day**, usually after meals - **Triggered by:** - **Gastrocolic reflex:** Distension of the stomach → vagal and hormonal signals → mass movement in the colon - **Duodenocolic reflex:** Distension of the duodenum → colonic motility - Both reflexes are strongest after **breakfast** (after the overnight fast) - This is why many people feel the urge to defecate after breakfast - **Hormones involved:** Gastrin, CCK - Mass movements are responsible for moving fecal material into the sigmoid colon and rectum, initiating the urge to defecate ### Clinical Correlation: Irritable Bowel Syndrome (IBS) - **Functional disorder** — no structural/biochemical abnormality identifiable - Altered GI motility and visceral hypersensitivity - **IBS-D (diarrhea-predominant):** Increased propulsive contractions, rapid transit - **IBS-C (constipation-predominant):** Increased non-propulsive (segmenting) contractions, slow transit - **IBS-M (mixed)** - Rome IV criteria: Recurrent abdominal pain at least 1 day/week in the last 3 months, associated with ≥2 of: related to defecation, change in stool frequency, change in stool form - Treatment: Dietary modification (low FODMAP diet), fiber, antispasmodics, loperamide (IBS-D), linaclotide/lubiprostone (IBS-C), rifaximin, psychological therapies ### Clinical Correlation: Volvulus - **Twisting** of the colon around its mesenteric axis → obstruction + vascular compromise - **Sigmoid volvulus** (most common in adults; elderly, nursing home patients, psychiatric patients on constipating medications) - X-ray: "Coffee bean sign" or "inverted U sign" - Treatment: Sigmoidoscopic decompression followed by elective sigmoid resection - **Cecal volvulus** (younger patients, mobile cecum) - Treatment: Surgical (right hemicolectomy — endoscopic decompression usually fails) --- ## MIXING MOVEMENTS ### Segmentation Contractions (Small Intestine) - The **primary mixing movement** of the small intestine - **Mechanism:** Localized, concentric contractions of the circular muscle that divide the intestine into small ovoid segments - The contractions appear and disappear rhythmically at different points — the chyme is **"chopped" and "churned"** back and forth - **Frequency:** Set by the slow wave frequency: - Duodenum: 12 per minute - Ileum: 8-9 per minute - This frequency gradient (higher in duodenum, lower in ileum) contributes to a slow **net aboral movement** of chyme (but the primary function is mixing, not propulsion) - **Purpose:** 1. Thorough mixing of chyme with digestive enzymes, bile, pancreatic juice 2. Exposure of all parts of chyme to the mucosal surface for absorption 3. Slows transit to allow adequate time for digestion and absorption ### Pendular Movements - Rhythmic **longitudinal** contractions that cause the intestinal segments to shorten and lengthen alternately - This moves chyme back and forth over the mucosal surface without significant net propulsion - Contributes to mixing - Less important than segmentation ### Gastric Mixing Movements - In the stomach, the mixing is achieved primarily through **retropulsion** (as described above with the antral mill) - When peristaltic waves reach the closed pylorus, the chyme is forced backward → vigorous mixing - The fundus and body also exhibit **tonic contractions** that maintain steady pressure on gastric contents --- ## SPECIFIC MOVEMENTS IN DIFFERENT REGIONS ### Movements of the Esophagus Already discussed above under peristalsis. To summarize: - **Primary peristalsis** — continuation of swallowing - **Secondary peristalsis** — local distension reflex - **LES relaxation** — receptive relaxation (mediated by VIP and NO via vagus nerve and myenteric plexus) ### Deglutition (Swallowing) — Briefly Three phases: 1. **Oral (voluntary) phase:** Tongue pushes bolus posteriorly against palate → bolus reaches posterior pharynx → triggers swallowing reflex 2. **Pharyngeal (involuntary) phase:** Rapid (~1 second); coordinated by swallowing center (nucleus tractus solitarius and nucleus ambiguus in medulla); involves soft palate elevation, epiglottic closure, UES relaxation, pharyngeal peristalsis 3. **Esophageal (involuntary) phase:** Primary peristalsis propels bolus; LES relaxes via vagus-mediated receptive relaxation ### Clinical Correlation: Dysphagia - **Oropharyngeal dysphagia:** Difficulty initiating swallow; causes include stroke (most common), myasthenia gravis, Parkinson's, ALS, Zenker's diverticulum, head/neck tumors - **Esophageal dysphagia:** Difficulty after swallow initiated: - **Mechanical obstruction:** Dysphagia to solids first, then liquids as lumen narrows; causes: strictures, Schatzki ring, esophageal cancer, eosinophilic esophagitis - **Motility disorders:** Dysphagia to BOTH solids AND liquids from the beginning; causes: achalasia, diffuse esophageal spasm, scleroderma (CREST syndrome — fibrosis of smooth muscle → aperistalsis + incompetent LES → severe GERD) ### Movements of the Stomach **Receptive Relaxation:** - When food enters the stomach, the fundus and body **relax** to accommodate increasing volumes **without a significant increase in intragastric pressure** - Mediated by **vagovagal reflex** (afferent and efferent limbs both via vagus nerve) - Neurotransmitter: **VIP and NO** (from inhibitory NANC neurons) - Normal stomach can accommodate up to **1.5 L** with minimal pressure rise (compliance) **Adaptive Relaxation:** - Further relaxation that occurs when food is already in the stomach - Triggered by gastric wall distension (local reflex) ### Clinical Correlation: Post-Vagotomy Syndromes - **Truncal vagotomy** (for peptic ulcer disease — rarely done now): - Loss of receptive relaxation → rapid rise in intragastric pressure → rapid emptying of liquids (but delayed emptying of solids due to loss of antral pump coordination) - Requires drainage procedure (pyloroplasty or gastrojejunostomy) - Other complications: dumping syndrome, diarrhea, gallstone formation (loss of vagal stimulation to gallbladder) ### Movements of the Small Intestine Already discussed: - **Segmentation** (primary mixing movement) - **Peristalsis** (primary propulsive movement) - Both occur simultaneously — segmentation predominates in the fed state; peristalsis predominates in the fasted state (see MMC below) ### Migrating Motor Complex (MMC) / Migrating Myoelectric Complex - A pattern of electromechanical activity that occurs **during fasting** (interdigestive period) - Described by Szurszewski in 1969 - Originates in the stomach/duodenum and migrates slowly down the entire small intestine (takes about 90-120 minutes to traverse) - **Phases:** 1. **Phase I (Quiescence):** ~40-60% of the cycle; no contractile activity; only slow waves, no spikes 2. **Phase II (Intermittent irregular contractions):** ~20-30% of the cycle; increasing frequency of contractions; random spikes on slow waves 3. **Phase III (Regular, intense contractions):** ~5-10 minutes; maximum contractile activity; every slow wave has spike bursts; the "activity front" that sweeps the gut clean 4. **Phase IV (Declining activity):** Brief transition back to Phase I - **"Housekeeper of the gut"** — Phase III sweeps residual food particles, bacteria, desquamated cells, and secretions from the stomach and small intestine into the colon - **Regulation:** - **Motilin** is the primary hormonal mediator of Phase III - Motilin is released cyclically from Mo cells in the duodenum and jejunum during fasting - **Erythromycin** is a motilin receptor agonist — mimics Phase III activity → prokinetic effect - Vagal input also important - **Fed state abolishes the MMC** — eating triggers a change to the "fed pattern" (segmentation + short peristaltic waves) mediated by gastrin, CCK, insulin, and vagal activity ### Clinical Correlation: Small Intestinal Bacterial Overgrowth (SIBO) - **Disruption of the MMC** can lead to bacterial accumulation in the small intestine (normally relatively sterile: <10⁴ organisms/mL) - Causes: Diabetes (gastroparesis/dysmotility), scleroderma, intestinal pseudo-obstruction, post-surgical (blind loops, strictures), opioid use, achlorhydria (PPI use), immunodeficiency - **Consequences:** Bacterial deconjugation of bile salts → fat malabsorption → steatorrhea; bacterial consumption of vitamin B12 → B12 deficiency (but folate is produced by bacteria → folate levels may be elevated); carbohydrate fermentation → bloating, diarrhea - **Diagnosis:** Glucose or lactulose hydrogen breath test; gold standard = jejunal aspirate with >10⁵ CFU/mL - **Treatment:** Rifaximin (non-absorbable antibiotic), dietary modification, treat underlying cause, prokinetics ### Movements of the Large Intestine **Haustral contractions** and **mass movements** (already discussed above) **Ileocecal Valve (Sphincter):** - Normally slightly constricted (tonic contraction) — prevents backflow of colonic contents into ileum - **Relaxed by:** Gastrin (via gastroileal reflex), food in stomach - **Contracted by:** Distension of cecum (cecoileal reflex via short reflexes), irritants in cecum - Prevents bacterial contamination of the small intestine ### Defecation Reflex **Intrinsic (Myenteric) Defecation Reflex:** - Feces enter rectum → rectal wall distension → myenteric plexus activation → peristaltic waves in descending colon, sigmoid, and rectum → internal anal sphincter relaxation - This reflex alone is **weak** — usually insufficient for defecation **Parasympathetic Defecation Reflex (Extrinsic):** - When the intrinsic reflex is activated, afferent signals also travel via **pelvic nerves (S2-S4)** to the sacral spinal cord - Reflexive efferent signals return via pelvic nerves → greatly intensify peristalsis + relax internal anal sphincter (mediated by NO and VIP) - This is the **dominant reflex** **Anal Sphincters:** - **Internal anal sphincter (IAS):** Smooth muscle, under **autonomic (involuntary)** control; normally tonically contracted (sympathetic via hypogastric nerve); relaxes during defecation (parasympathetic + enteric NO/VIP) - **External anal sphincter (EAS):** Skeletal (striated) muscle, under **voluntary (somatic)** control via **pudendal nerve (S2-S4)**; can voluntarily contract to delay defecation - **Puborectalis muscle:** Maintains the anorectal angle (~90°); must relax during defecation to straighten the angle (to ~130-140°) **Defecation sequence:** 1. Mass movement delivers feces to rectum 2. Rectal distension → urge to defecate → RAIR (rectoanal inhibitory reflex — IAS relaxes) 3. Sampling reflex: Small amount of rectal contents contacts anal canal epithelium → sensory neurons discriminate gas vs liquid vs solid 4. If conditions are appropriate: - Voluntary relaxation of EAS and puborectalis - Assumption of squatting position (straightens anorectal angle) - Valsalva maneuver (increased intra-abdominal pressure) - Peristalsis evacuates rectum 5. If not appropriate: - Voluntary contraction of EAS → rectal accommodation (compliance) → urge temporarily subsides ### Clinical Correlations Related to Defecation **Fecal Incontinence:** - Loss of EAS tone: Pudendal nerve damage (obstetric injury, surgery, diabetes) - Loss of IAS tone: Scleroderma, aging, surgery - Rectal prolapse - Neurological: Cauda equina syndrome, spinal cord injury below S2 (loss of voluntary EAS control AND loss of parasympathetic defecation reflex) **Spinal Cord Lesions and Defecation:** - **Lesion above S2-S4 (upper motor neuron):** Loss of voluntary control of EAS, BUT the sacral parasympathetic reflex arc is intact → reflex defecation occurs (mass reflex defecation) → spastic bowel; can be managed with digital stimulation, suppositories - **Lesion at/below S2-S4 (lower motor neuron; cauda equina):** Loss of the parasympathetic defecation reflex AND loss of EAS voluntary control → flaccid, atonic bowel → constipation + overflow incontinence; requires manual evacuation **Hirschsprung's Disease:** (discussed above) — absence of RAIR is diagnostic **Constipation:** - Functional (most common): Inadequate fiber/fluid, sedentary lifestyle, ignoring urge to defecate - Slow-transit constipation: Reduced colonic motility, decreased ICC density - Outlet obstruction (dyssynergic defecation/anismus): Failure to relax puborectalis and EAS during defecation → paradoxical contraction → diagnosed by anorectal manometry and balloon expulsion test → treated with biofeedback --- ## SPHINCTERS OF THE GI TRACT Sphincters are areas of **tonically contracted circular muscle** that act as valves: | Sphincter | Location | Tonic State | Key Controllers | |-----------|----------|-------------|-----------------| | Upper Esophageal Sphincter (UES) | Cricopharyngeus | Closed | Vagus, glossopharyngeal; opens with swallowing | | Lower Esophageal Sphincter (LES) | GE junction | Closed (15-25 mmHg) | Intrinsic myogenic tone; VIP/NO → relaxation; ACh → contraction | | Pyloric Sphincter | Gastroduodenal junction | Partially closed | CCK → contraction; vagal stimulation → relaxation during gastric emptying | | Sphincter of Oddi | Ampulla of Vater | Closed | CCK → relaxation; opioids → contraction | | Ileocecal Valve | Ileal-cecal junction | Partially closed | Discussed above | | Internal Anal Sphincter | Anal canal | Closed | Sympathetic → contraction; parasympathetic/NO → relaxation | | External Anal Sphincter | Anal canal | Closed | Pudendal nerve (voluntary) | ### Clinical Correlation: GERD (Gastroesophageal Reflux Disease) - **Primary mechanism:** Transient lower esophageal sphincter relaxations (TLESRs) — inappropriate relaxation of LES not associated with swallowing - Other factors: Low resting LES pressure, hiatal hernia (disrupts diaphragmatic crural contribution to LES), delayed gastric emptying, impaired esophageal clearance - Factors that DECREASE LES pressure: Chocolate, caffeine, alcohol, smoking, fatty foods, peppermint, progesterone (pregnancy), anticholinergics, calcium channel blockers, nitrates, theophylline - Factors that INCREASE LES pressure: Gastrin, motilin, substance P, prostaglandin F2α, protein meals - **Complications:** Erosive esophagitis, stricture, Barrett's esophagus (intestinal metaplasia — replacement of stratified squamous epithelium with columnar epithelium with goblet cells → risk of esophageal adenocarcinoma), aspiration pneumonia - **Treatment:** Lifestyle modifications, PPIs, H2 blockers, fundoplication (Nissen) for refractory cases ### Clinical Correlation: Sphincter of Oddi Dysfunction - Stenosis or spasm → recurrent biliary/pancreatic-type pain, elevated liver enzymes, dilated CBD - **Opioids (especially morphine)** cause contraction of the sphincter of Oddi → contraindicated in biliary colic (meperidine traditionally considered to cause less spasm, but evidence is weak) - **CCK** causes sphincter of Oddi relaxation (opposite to its effect on the pylorus!) - Diagnosis: Sphincter of Oddi manometry - Treatment: Endoscopic sphincterotomy --- ## NEURAL CONTROL OF GI MOTILITY — SUMMARY ### Intrinsic (Enteric) Nervous System - "Brain of the gut" — can function independently of CNS - ~100 million neurons - **Myenteric (Auerbach's) plexus:** Between longitudinal and circular muscle layers; primarily controls **motility** - **Submucosal (Meissner's) plexus:** In submucosa; primarily controls **secretion** and local blood flow - Key neurotransmitters: - **Excitatory:** ACh, Substance P (promote contraction) - **Inhibitory:** NO, VIP, ATP (promote relaxation) ### Extrinsic Nervous System **Parasympathetic:** - **Vagus nerve:** Innervates esophagus through proximal 2/3 of transverse colon (entire foregut and midgut) - **Pelvic nerves (S2-S4):** Innervate distal 1/3 of transverse colon through rectum and anus (hindgut) - Generally **excitatory** (increases motility, relaxes sphincters, increases secretion) - Works by stimulating enteric neurons (mainly myenteric plexus) — ACh and other transmitters **Sympathetic:** - T5-L2 → celiac, superior mesenteric, inferior mesenteric, and hypogastric ganglia → post-ganglionic fibers to gut wall - Generally **inhibitory** (decreases motility, contracts sphincters, decreases secretion) - Norepinephrine acting on β2 receptors → smooth muscle relaxation - Norepinephrine acting on α1 receptors → sphincter contraction - Also inhibits ACh release from enteric neurons (presynaptic α2 receptors) - Vasoconstriction of GI blood vessels (α1) --- ## PART 2: GASTROINTESTINAL BLOOD FLOW — SPLANCHNIC CIRCULATION --- ## OVERVIEW AND ANATOMY ### Definition The **splanchnic circulation** includes the blood supply to: - The GI tract (stomach, small intestine, large intestine) - Spleen - Pancreas - Liver ### Arterial Supply The GI organs receive blood from three major branches of the abdominal aorta: 1. **Celiac trunk (artery)** — supplies foregut derivatives: - **Left gastric artery** → lesser curvature of stomach, lower esophagus - **Common hepatic artery** → liver (hepatic artery proper), gallbladder (cystic artery), duodenum (gastroduodenal → superior pancreaticoduodenal), stomach (right gastric) - **Splenic artery** → spleen, body/tail of pancreas, stomach (short gastric arteries, left gastroepiploic) 2. **Superior Mesenteric Artery (SMA)** — supplies midgut derivatives: - Inferior pancreaticoduodenal artery - Jejunal and ileal branches - Middle colic artery (transverse colon) - Right colic artery (ascending colon) - Ileocolic artery (terminal ileum, cecum, appendix) - Supplies from lower duodenum to proximal 2/3 of transverse colon 3. **Inferior Mesenteric Artery (IMA)** — supplies hindgut derivatives: - Left colic artery (descending colon) - Sigmoid arteries - Superior rectal artery - Supplies from distal 1/3 of transverse colon to upper rectum ### Collateral Circulation — Critical Anastomoses 1. **Marginal artery of Drummond:** Continuous arterial arcade along the mesenteric border of the colon connecting SMA and IMA territories 2. **Arc of Riolan (meandering mesenteric artery):** Direct connection between the middle colic artery (SMA) and left colic artery (IMA) — may be absent in some individuals 3. **Pancreaticoduodenal arcades:** Connect celiac and SMA territories ### Clinical Correlation: Watershed Areas - **Splenic flexure (Griffith's point):** Junction of SMA and IMA territories — most vulnerable to ischemia during low-flow states (shock, cardiac surgery, aortic surgery) - **Rectosigmoid junction (Sudeck's point):** Junction of IMA (superior rectal) and internal iliac (middle and inferior rectal) territories - These watershed areas are most susceptible to **ischemic colitis** ### Venous Drainage — The Portal System All venous blood from the GI tract (stomach through rectum), spleen, and pancreas drains into the **portal vein** → liver → hepatic veins → IVC **Formation of Portal Vein:** - **Superior Mesenteric Vein (SMV)** + **Splenic Vein** = **Portal Vein** (behind the neck of the pancreas) - **Inferior Mesenteric Vein (IMV)** usually joins the splenic vein (or SMV, or the junction) **Portal Vein:** - Length: ~8 cm - Carries **75% of total hepatic blood flow** (~1050 mL/min) but only **50% of oxygen delivery** - Contains nutrient-rich, partially deoxygenated blood - Pressure: 5-10 mmHg normally **Hepatic Artery:** - Carries **25% of total hepatic blood flow** (~300 mL/min) but **50% of oxygen delivery** - Contains fully oxygenated blood - There is a reciprocal relationship: If portal flow decreases, hepatic arterial flow increases (**hepatic arterial buffer response** — mediated by adenosine washout mechanism) ### Clinical Correlation: Portal Hypertension - **Definition:** Portal vein pressure >12 mmHg (or hepatic venous pressure gradient >5 mmHg; clinically significant if >10 mmHg) - **Most common cause:** Liver cirrhosis (intrahepatic, sinusoidal) - **Classification:** - **Pre-hepatic:** Portal vein thrombosis, splenic vein thrombosis - **Intrahepatic:** - Pre-sinusoidal: Schistosomiasis (most common cause worldwide), primary biliary cholangitis, sarcoidosis - Sinusoidal: Cirrhosis (most common cause in Western countries) - Post-sinusoidal: Veno-occlusive disease (sinusoidal obstruction syndrome — e.g., after bone marrow transplant, pyrrolizidine alkaloids) - **Post-hepatic:** Budd-Chiari syndrome (hepatic vein thrombosis), constrictive pericarditis, right heart failure - **Consequences of portal hypertension — Portosystemic anastomoses (sites of collateral circulation):** | Site | Portal Vessel | Systemic Vessel | Clinical Manifestation | |------|--------------|-----------------|----------------------| | Lower esophagus/gastric fundus | Left gastric vein (coronary vein) | Esophageal branches of azygos vein | **Esophageal/gastric varices** (most dangerous — rupture → massive upper GI bleeding) | | Rectum | Superior rectal vein | Middle and inferior rectal veins (internal iliac) | **Anorectal varices** (NOT hemorrhoids — hemorrhoids are not a consequence of portal hypertension) | | Periumbilical | Paraumbilical veins (via round ligament/ligamentum teres) | Superficial epigastric veins | **Caput medusae** (dilated periumbilical veins radiating from umbilicus) | | Retroperitoneal | Colic/intestinal veins | Renal, lumbar, gonadal veins | Retroperitoneal varices | | Bare area of liver | Portal branches | Diaphragmatic veins | — | - **Other manifestations:** Splenomegaly (congestive), ascites, hepatorenal syndrome, hepatic encephalopathy (portosystemic shunting of ammonia and other toxins) - **Treatment of variceal bleeding:** Resuscitation, octreotide/terlipressin (reduce splanchnic blood flow), emergent endoscopy with band ligation or sclerotherapy, balloon tamponade (Sengstaken-Blakemore tube) as bridge, TIPS (transjugular intrahepatic portosystemic shunt) for refractory cases, propranolol/nadolol (non-selective β-blockers) for primary/secondary prophylaxis (reduce portal pressure by decreasing cardiac output [β1] and causing splanchnic vasoconstriction [β2 blockade allows unopposed α-mediated constriction]) --- ## BLOOD FLOW DISTRIBUTION IN THE GI TRACT ### Magnitude - Total splanchnic blood flow at rest: approximately **1400-1800 mL/min** (25-30% of cardiac output) - After a meal: Can increase to **2000-2500 mL/min** or more - Distribution: - Liver: ~1350 mL/min (portal 1050 + hepatic arterial 300) - Small intestine: Receives the largest share of mesenteric flow - Stomach, colon, pancreas, spleen: Remainder ### Microcirculation of the Intestinal Villus The intestinal villus has a unique **countercurrent exchange system:** **Structure:** - A single arteriole ascends in the center of the villus to the tip - Blood flows up the arteriole and returns via a network of venules/capillaries surrounding it, flowing downward - The arteriole and venules run in close proximity in a **countercurrent arrangement** **Countercurrent Exchange of Oxygen:** - Oxygen diffuses from the ascending arteriole to the descending venules across the short distance at every level of the villus - This creates an **oxygen gradient:** highest at the base, lowest at the tip - The **tip of the villus** is relatively **hypoxic** even under normal conditions (PO₂ at villus tip can be as low as 10-20 mmHg compared to 60-70 mmHg at the base) **Significance:** - The villus tip is the **most vulnerable to ischemic injury** - During states of reduced blood flow (shock, hypotension, vasoconstriction), the villus tip undergoes ischemic necrosis first - This manifests as **villus sloughing** and loss of mucosal barrier ### Clinical Correlation: Neonatal Necrotizing Enterocolitis (NEC) - Primarily affects premature infants - Ischemic necrosis of intestinal mucosa (especially terminal ileum and proximal colon) - Pathogenesis: Immature gut + immature circulation + bacterial colonization → intestinal ischemia → necrosis → bacterial translocation → sepsis - **Pneumatosis intestinalis** (gas within the bowel wall) on X-ray is pathognomonic - Portal venous gas on X-ray indicates severe disease - Treatment: NPO, nasogastric decompression, IV antibiotics, surgery if perforation ### Countercurrent Exchange of Solutes - Absorbed solutes (e.g., sodium, glucose, small molecules) in the ascending venous blood can also diffuse back to the arteriolar blood → "short-circuiting" of absorbed solutes - This is normally not significant for most nutrients - However, it IS significant for **lipid-insoluble gases** (e.g., inert gases) and explains the "villus trapping" of certain substances - **Countercurrent multiplier for NaCl** may contribute to maintaining a hypertonic villus tip (helps with water absorption) --- ## REGULATION OF SPLANCHNIC BLOOD FLOW ### Intrinsic (Local) Regulation #### 1. Metabolic Autoregulation (Functional Hyperemia) - **Most important mechanism** for increasing GI blood flow after a meal - Active digestion and absorption → increased metabolic activity of mucosa → local release of vasodilator metabolites: - **Adenosine** (most important) - CO₂ - K⁺ - H⁺ - Decreased O₂ - These cause arteriolar dilation → increased blood flow - Blood flow can increase **50-100% or more** after a meal (postprandial hyperemia) - The increase is localized to the segment actively digesting/absorbing food #### 2. Myogenic Autoregulation (Bayliss Effect) - Smooth muscle in arteriolar walls responds to **stretch** (increased transmural pressure) by **contracting** - This helps maintain relatively constant blood flow when arterial pressure changes (autoregulation) - Effective over MAP range of approximately 60-140 mmHg - Below 60 mmHg → autoregulation fails → flow becomes pressure-dependent #### 3. Mucosal Blood Flow and the "Villus Pump" - Rhythmic contractions of the villus (via muscularis mucosae) create a pumping action that moves blood and lymph out of the villus - This promotes blood flow through the villus capillaries ### Hormonal Regulation | Hormone | Effect on GI Blood Flow | |---------|------------------------| | **Gastrin** | Increases mucosal blood flow (stomach) | | **CCK** | Increases blood flow to pancreas and small intestine | | **Secretin** | Increases pancreatic blood flow | | **Glucagon** | Vasodilation → increases splanchnic blood flow | | **VIP** | Potent vasodilator → increases mucosal blood flow | | **Substance P** | Vasodilation | | **Vasopressin (ADH)** | Splanchnic vasoconstriction (used therapeutically in variceal bleeding) | | **Angiotensin II** | Splanchnic vasoconstriction | - After a meal: Gastrin, CCK, secretin, and other hormones contribute to the **postprandial hyperemia** in addition to metabolic factors - **Kinins (bradykinin, kallidin):** Released by exocrine glands (salivary, pancreas) during secretory activity → potent vasodilation → increased glandular blood flow during secretion ### Neural Regulation #### Parasympathetic (Vagus and Pelvic Nerves) - **Indirect vasodilation:** Stimulates glandular secretion and motility → increased metabolic activity → local metabolic vasodilation → increased blood flow - Also releases **VIP** from enteric neurons → direct vasodilation - Does NOT directly innervate blood vessels significantly (except via VIP-ergic neurons) - So the parasympathetic effect on blood flow is primarily **indirect** (via increased metabolic activity) #### Sympathetic - Direct innervation of arterioles, venules, and arteries in the GI tract - **Neurotransmitter:** Norepinephrine - **α₁ receptors** (predominant) → **vasoconstriction** - This is the most important neural mechanism for **reducing** splanchnic blood flow - During sympathetic activation (exercise, hemorrhage, shock): - Intense splanchnic vasoconstriction → shunts blood to skeletal muscles, heart, brain - The splanchnic circulation serves as a **blood reservoir** (~20-30% of blood volume can be mobilized) - **Splanchnic venoconstriction** (α₁ on venous capacitance vessels) → mobilizes blood from the splanchnic venous reservoir → increases venous return to the heart - This is one of the first and most important compensatory mechanisms in hemorrhagic shock **Autoregulatory Escape:** - During sustained sympathetic stimulation, the initial vasoconstriction of the gut arterioles gradually **wanes** after 1-3 minutes - Blood flow partially returns toward normal despite continued sympathetic discharge - Mechanism: Local metabolic vasodilators (adenosine, etc.) accumulate due to ischemia and overcome the sympathetic vasoconstrictor effect - **Significance:** Protects the gut from prolonged ischemia during sympathetic activation (e.g., exercise) - However, during **severe, prolonged shock**, autoregulatory escape may be overwhelmed → mucosal ischemia → barrier breakdown → bacterial translocation → sepsis → MODS (multi-organ dysfunction syndrome) ### Clinical Correlation: Shock and GI Tract (Ischemic Gut) - During **hemorrhagic/cardiogenic/septic shock:** - Intense sympathetic-mediated splanchnic vasoconstriction redistributes blood to vital organs - Prolonged ischemia → mucosal barrier breakdown → bacterial translocation (bacteria and endotoxin cross into portal blood and systemic circulation) - This contributes to **SIRS (Systemic Inflammatory Response Syndrome)** and **MODS** - The gut has been called the **"motor of MODS"** or **"motor of multiple organ failure"** - **Non-occlusive mesenteric ischemia (NOMI):** Mesenteric vasoconstriction without arterial/venous occlusion, seen in: - Low-flow states (heart failure, shock) - Vasopressor use (norepinephrine, vasopressin, digitalis) - Cocaine use - Hemodialysis - Treatment: Papaverine infusion via mesenteric catheter, correct underlying cause --- ## MESENTERIC ISCHEMIA — DETAILED CLINICAL CORRELATIONS ### Acute Mesenteric Ischemia **Causes:** 1. **SMA embolism** (50%) — most common cause - Source: Left atrial thrombus (atrial fibrillation), LV mural thrombus (post-MI), valvular disease - Sudden onset; embolus typically lodges just distal to the origin of the middle colic artery 2. **SMA thrombosis** (15-25%) - Usually on pre-existing atherosclerotic plaque at the origin of the SMA - History of chronic mesenteric ischemia (intestinal angina) may precede 3. **Mesenteric venous thrombosis** (5-15%) - Associated with hypercoagulable states (Factor V Leiden, protein C/S deficiency, antiphospholipid syndrome), portal hypertension, intra-abdominal inflammation, malignancy - More insidious onset 4. **Non-occlusive mesenteric ischemia (NOMI)** (20-30%) - Discussed above **Classic Presentation:** **"Pain out of proportion to physical findings"** - Severe, diffuse, periumbilical abdominal pain - Early: Pain is severe but abdomen is soft and non-tender (discrepancy is the hallmark) - Late: Peritonitis (guarding, rigidity, rebound) — indicates bowel infarction - Bloody diarrhea (if hemorrhagic infarction) - Nausea, vomiting - Leukocytosis, elevated lactate, metabolic acidosis (late findings indicating infarction) **Diagnosis:** - **CT angiography** (best initial test) — shows vascular occlusion and bowel wall changes - Conventional angiography (gold standard for diagnosis AND treatment of NOMI) - Elevated serum lactate, D-dimer (sensitive but not specific) **Treatment:** - Fluid resuscitation, broad-spectrum antibiotics - **SMA embolism/thrombosis:** Surgical embolectomy/thrombectomy + resection of necrotic bowel; catheter-directed thrombolysis if no peritonitis; anticoagulation - **NOMI:** Intra-arterial papaverine; optimize cardiac output; avoid vasoconstrictors - **Venous thrombosis:** Anticoagulation (heparin → warfarin) **Prognosis:** Mortality 50-80% (especially if diagnosis delayed) ### Chronic Mesenteric Ischemia (Intestinal Angina) - Atherosclerotic narrowing of at least **2 of 3** mesenteric arteries (celiac, SMA, IMA) — collateral circulation protects until multiple vessels are compromised - **Postprandial abdominal pain** ("intestinal angina") — pain occurs 15-30 minutes after eating because digestion requires increased blood flow that the stenotic vessels cannot deliver - Weight loss (patients develop **sitophobia** — fear of eating due to pain) - Diagnosis: CTA or MRA, duplex ultrasound of mesenteric vessels - Treatment: Mesenteric revascularization (angioplasty + stenting or surgical bypass) ### Ischemic Colitis - Most common form of mesenteric ischemia overall - Usually affects **watershed areas** (splenic flexure, rectosigmoid junction) - Typical patient: Elderly with cardiovascular disease, after aortic surgery - Presentation: Sudden onset of crampy left-sided abdominal pain, urgency to defecate, bloody diarrhea (usually moderate) - Usually **non-gangrenous** (transient/self-limited in ~85% of cases) — affects only mucosa and submucosa - Diagnosis: CT, colonoscopy (within 48 hours — shows edema, hemorrhage, ulceration; "thumbprinting" on barium enema or CT = submucosal hemorrhage/edema) - Treatment: Supportive (IV fluids, bowel rest, antibiotics if severe); surgery if gangrenous/perforated - Can lead to stricture formation if chronic --- ## HEPATIC CIRCULATION IN DETAIL ### Dual Blood Supply - **Portal vein:** 75% of flow, 50% of O₂ - **Hepatic artery:** 25% of flow, 50% of O₂ - Total hepatic blood flow: ~1350-1500 mL/min (25-30% of cardiac output) ### Hepatic Sinusoids - Specialized capillaries of the liver - Receive mixed blood from both portal venules and hepatic arterioles - **Fenestrated endothelium** (discontinuous) with no basement membrane → allows free exchange of plasma proteins and nutrients with hepatocytes - Contain **Kupffer cells** (resident macrophages) — phagocytose bacteria, endotoxins, old RBCs from portal blood - Blood flows from **portal triads** (at periphery of lobule) → through sinusoids → to **central vein** (center of lobule) → hepatic veins → IVC ### Hepatic Zones (Rappaport Acinus Model) - **Zone 1 (periportal):** Closest to blood supply; receives most oxygenated blood; highest metabolic activity for gluconeogenesis, urea synthesis, bile formation; most resistant to ischemia - **Zone 2 (mid-zone):** Intermediate - **Zone 3 (pericentral/centrilobular):** Farthest from blood supply; most hypoxic; most susceptible to **ischemic necrosis** (centrilobular necrosis — seen in shock, CHF, hepatic vein obstruction); most active in drug metabolism (cytochrome P450), lipogenesis, glycolysis; where acetaminophen toxicity damage is worst ### Hepatic Arterial Buffer Response (HABR) - If **portal blood flow decreases** (e.g., portal vein thrombosis), **hepatic arterial flow automatically increases** to compensate - Mechanism: **Adenosine washout hypothesis** - Adenosine is constitutively produced in the space of Mall (periportal space) - Normal portal flow washes it away → keeps hepatic arterioles at baseline tone - When portal flow decreases → adenosine accumulates → adenosine causes hepatic arteriolar vasodilation → increased hepatic arterial flow - This is NOT reciprocal — hepatic arterial flow changes do NOT affect portal flow (portal flow is determined by splanchnic arteriolar resistance and cannot be independently regulated) - Clinical significance: Maintains hepatic oxygen delivery when portal flow is compromised ### Clinical Correlation: Budd-Chiari Syndrome - Thrombosis/obstruction of hepatic veins (or IVC at the hepatic level) - Classic triad: **Hepatomegaly, ascites, abdominal pain** - Causes: Myeloproliferative neoplasms (most common; especially polycythemia vera — JAK2 mutation), hypercoagulable states, oral contraceptives, pregnancy, paroxysmal nocturnal hemoglobinuria - **Nutmeg liver** on pathology (centrilobular congestion and necrosis) - Diagnosis: Doppler ultrasound (absence of hepatic venous flow), CT/MRI, hepatic venography - Treatment: Anticoagulation, TIPS, liver transplantation (severe cases) --- ## BLOOD RESERVOIR FUNCTION OF THE SPLANCHNIC CIRCULATION - The splanchnic venous system (especially the liver, spleen, and mesenteric veins) is a major **capacitance reservoir** - Normally holds **20-30% of total blood volume** (~1000-1500 mL) - During hemorrhage/shock: - Sympathetic activation → α₁-mediated venoconstriction → mobilizes up to **500-1000 mL** of blood from the splanchnic reservoir into the systemic circulation - This is one of the most important compensatory mechanisms to maintain cardiac output and blood pressure - During exercise: - Splanchnic vasoconstriction redistributes blood to skeletal muscles - Splanchnic blood flow can decrease by 50-80% during vigorous exercise - This explains why vigorous exercise after a meal causes GI cramps ("side stitches") — the gut is underperfused while it needs increased flow for digestion ### Clinical Correlation: Exercise-Related GI Symptoms - Common in endurance athletes: "Runner's diarrhea," abdominal cramps, nausea, GI bleeding - Mechanisms: Splanchnic hypoperfusion during exercise + mechanical trauma (running) - Can cause ischemic colitis in extreme cases - Prevention: Avoid eating close to exercise, adequate hydration, training adaptation --- ## POSTPRANDIAL HYPEREMIA — INTEGRATED RESPONSE After a meal, splanchnic blood flow increases by 50-100% or more. This involves multiple coordinated mechanisms: 1. **Metabolic factors** (most important): Increased mucosal metabolic activity → adenosine, CO₂, K⁺, H⁺ → arteriolar dilation 2. **GI hormones:** Gastrin, CCK, secretin, VIP, glucagon → vasodilation 3. **Parasympathetic activation:** Vagal stimulation → increased secretion and motility → increased metabolic activity → indirect vasodilation; also VIP release → direct vasodilation 4. **Kinins:** Released during glandular secretion → vasodilation 5. **Decreased sympathetic tone** to splanchnic bed after eating 6. **Serotonin (5-HT):** Released from enterochromaffin cells during mucosal stimulation → local vasodilation ### Sequence - Food enters stomach → gastrin release → gastric mucosal blood flow increases - Chyme enters duodenum → CCK, secretin release → pancreatic, duodenal blood flow increases - As chyme moves along small intestine → local metabolic hyperemia follows the wave of digestion/absorption ### Clinical Correlation: Postprandial Hypotension - Seen in elderly, patients with autonomic dysfunction (diabetes, Parkinson's, multiple system atrophy), dialysis patients - After a meal → splanchnic vasodilation → blood pooling in splanchnic bed → if sympathetic compensation is impaired → drop in systemic BP → syncope, falls - Defined as: Drop in systolic BP ≥20 mmHg within 2 hours of a meal - Management: Small, frequent meals; low carbohydrate content; adequate hydration; caffeine (adenosine antagonist — reduces splanchnic vasodilation); minimize antihypertensives before meals; octreotide (inhibits release of vasodilatory GI peptides) ### Clinical Correlation: Abdominal Angina / Chronic Mesenteric Ischemia (revisited) - Postprandial hyperemia cannot be achieved due to stenotic mesenteric arteries → supply-demand mismatch → ischemic pain after eating --- ## SPECIAL CIRCULATIONS WITHIN THE SPLANCHNIC BED ### Splenic Circulation - Splenic artery (from celiac trunk) → enters hilum → branches into trabecular arteries → central arteries (surrounded by white pulp/lymphoid tissue) → penicillar arteries → **open circulation** (blood spills into splenic cords of red pulp → percolates through → re-enters splenic sinuses → splenic vein) - Functions: Filtration of old/abnormal RBCs, immune surveillance, blood reservoir (~250 mL in normal spleen) - Splenomegaly (e.g., in portal hypertension) → increased blood sequestration → **hypersplenism** (pancytopenia) ### Pancreatic Circulation - Dual blood supply: Branches from celiac trunk (via splenic artery and gastroduodenal → superior pancreaticoduodenal) and SMA (inferior pancreaticoduodenal) - Blood flow increases significantly during secretion (stimulated by CCK, secretin) - Islets of Langerhans have a specialized microvasculature: **insulo-acinar portal system** — blood flows from islets → surrounding exocrine tissue → insulin modulates exocrine function --- ## SUMMARY TABLE: GI MOVEMENTS BY REGION | Region | Primary Mixing Movement | Primary Propulsive Movement | Frequency of Slow Waves | Special Features | |--------|------------------------|-----------------------------|------------------------|------------------| | Esophagus | None significant | Primary/secondary peristalsis | No slow waves in striated portion | Striated→smooth muscle transition | | Stomach (fundus/body) | Tonic contraction, retropulsion | Peristalsis (weak in body) | 3/min | Receptive relaxation, reservoir | | Stomach (antrum) | Antral mill (retropulsion) | Strong peristalsis toward pylorus | 3/min | Grinding of food | | Duodenum | Segmentation | Peristalsis | 12/min (highest) | Origin of MMC | | Jejunum | Segmentation | Peristalsis | 10-11/min | | | Ileum | Segmentation | Peristalsis | 8-9/min | Gastroileal reflex | | Colon | Haustral contractions | Mass movements (1-3/day) | 2-6/min | Gastrocolic reflex | | Rectum | — | Defecation reflex | — | RAIR | --- ## KEY CLINICAL CORRELATIONS — SUMMARY TABLE | Condition | Pathophysiology | Key Finding | |-----------|----------------|-------------| | Achalasia | Loss of inhibitory neurons (NO/VIP) in LES | Bird's beak on barium swallow; aperistalsis on manometry | | Hirschsprung's | Absent ganglion cells in distal colon | Absent RAIR; transition zone on barium enema | | GERD | Transient LES relaxations; low LES pressure | Heartburn; Barrett's esophagus | | Gastroparesis | Impaired gastric emptying (vagal neuropathy, loss of ICC) | Delayed gastric emptying on scintigraphy | | Paralytic ileus | Absent peristalsis without obstruction | Diffuse dilated bowel; no bowel sounds | | SIBO | Loss of MMC "housekeeper" function | B12 deficiency with elevated folate | | Acute mesenteric ischemia | SMA embolism/thrombosis, NOMI | Pain out of proportion to exam; elevated lactate | | Ischemic colitis | Watershed ischemia | Thumbprinting; splenic flexure involvement | | Portal hypertension | Increased resistance to portal flow | Varices, ascites, caput medusae, splenomegaly | | Dumping syndrome | Rapid gastric emptying post-surgery | Early (osmotic) and late (hypoglycemic) symptoms | | Diffuse esophageal spasm | Simultaneous non-peristaltic contractions | Corkscrew esophagus | | Chagas disease | Trypanosoma cruzi destroys myenteric plexus | Megaesophagus, megacolon | | Postprandial hypotension | Impaired sympathetic compensation for splanchnic vasodilation | Syncope after meals in elderly/dysautonomia | | Autoregulatory escape | Local metabolites overcome sympathetic vasoconstriction | Partial restoration of gut blood flow during sustained sympathetic stimulation | --- This comprehensive review covers the physiology of GI motility (electrical basis, propulsive and mixing movements in every region, sphincter function, neural and hormonal control, MMC, and defecation) and splanchnic circulation (anatomy, regulation, countercurrent exchange, portal system, hepatic circulation, reservoir function, and postprandial hyperemia), along with all major clinical correlations from achalasia to mesenteric ischemia to portal hypertension and beyond. Rewrite the whole content as it is plus add maximum number of high yield clear images along the content from your side
GI tract slow waves interstitial cells of Cajal peristalsis diagram physiology
achalasia bird beak barium swallow esophageal manometry radiology image
peristalsis law of intestine myenteric reflex diagram excitatory inhibitory neurons
migrating motor complex MMC phases diagram gastroenterology
portal hypertension portosystemic anastomoses varices caput medusae diagram
Physiology of Functional Types of Movements in the GI Tract & Splanchnic Circulation
PART 1: FUNCTIONAL TYPES OF GI MOVEMENTS
- Mixing movements
- Propulsive movements
BASIC ELECTRICAL ACTIVITY OF GI SMOOTH MUSCLE
Slow Waves (Basic Electrical Rhythm - BER)
- Not true action potentials — they are rhythmic, undulating changes in resting membrane potential
- Generated by the Interstitial Cells of Cajal (ICC), which act as the pacemaker cells of the GI tract
- ICC are located between the longitudinal and circular muscle layers (at the level of the myenteric plexus) and also within the circular muscle layer

- Slow wave frequency varies by region:
- Stomach (body/antrum): 3 per minute
- Duodenum: 12 per minute (highest frequency in the GI tract)
- Ileum: 8-9 per minute
- Cecum/colon: 2-6 per minute (gradient from cecum to sigmoid)
- Slow waves do not cause contraction by themselves (except in the stomach where they can cause weak contractions). They merely set the timing and maximum frequency of contractions
- Mechanism: Cyclic opening of non-selective cation channels → Na⁺ influx → depolarization; then repolarization by K⁺ efflux
Spike Potentials (Action Potentials)
- True action potentials superimposed on slow waves
- Occur when the slow wave depolarization reaches threshold (approximately -40 mV)
- Duration: 10-40 ms (much longer than nerve/skeletal muscle action potentials of 1-2 ms)
- Ionic basis: Calcium-sodium channels (slow channels) — Ca²⁺ influx is the major depolarizing current (not Na⁺ as in skeletal muscle)
- This is why GI smooth muscle contraction depends heavily on extracellular Ca²⁺
- K⁺ efflux causes repolarization
- The number of spike potentials on a slow wave determines the strength of contraction (more spikes = more Ca²⁺ entry = stronger contraction)

Factors That Affect Spike Generation
- Stretching of the muscle
- Acetylcholine (parasympathetic stimulation)
- Substance P
- GI-specific stimulating hormones (gastrin, CCK, motilin)
- Norepinephrine (sympathetic stimulation)
- Epinephrine
- VIP, Secretin, GIP
- Nitric oxide
🔴 Clinical Correlation: Hirschsprung's Disease (Congenital Megacolon)
- Pathology: Absence of ganglion cells (both myenteric and submucosal plexus) in a segment of the distal colon (usually rectosigmoid) due to failure of neural crest cell migration
- Also involves absence or dysfunction of ICC in the aganglionic segment
- The aganglionic segment remains tonically contracted (because the normal inhibitory innervation via NO and VIP is absent)
- The proximal normal colon dilates massively (megacolon)
- Presentation: Failure to pass meconium within 48 hours of birth, abdominal distension, bilious vomiting
- Diagnosis: Rectal suction biopsy (absence of ganglion cells), barium enema (transition zone), anorectal manometry (absence of rectoanal inhibitory reflex — RAIR)
- Treatment: Surgical pull-through procedure (Soave, Swenson, or Duhamel)
PROPULSIVE MOVEMENTS — PERISTALSIS
Definition
Mechanism (Law of the Intestine / Law of the Gut / Myenteric Reflex)
-
Behind the bolus (orad side):
- Stretch activates sensory neurons (IPANs — intrinsic primary afferent neurons) in the myenteric plexus
- These activate excitatory motor neurons
- Excitatory neurotransmitters: Acetylcholine and Substance P
- Result: Contraction of circular muscle (constriction) behind the bolus — the "propulsive segment"
- Simultaneously, the longitudinal muscle relaxes
-
Ahead of the bolus (aborad side):
- Inhibitory motor neurons are activated
- Inhibitory neurotransmitters: Nitric oxide (NO), VIP (Vasoactive Intestinal Peptide), and ATP
- Result: Relaxation of circular muscle ahead of the bolus — the "receiving segment"
- Simultaneously, the longitudinal muscle contracts

Characteristics of Peristalsis
- Unidirectional: Normally proceeds only in the oral-to-anal direction (anterograde). This directional polarity is called the law of the intestine and is an inherent property of the enteric nervous system
- Velocity: Varies by region:
- Esophagus: 3-5 cm/sec (fastest)
- Stomach: 1 cm/sec
- Small intestine: 0.5-2 cm/sec
- Colon: Very slow, usually a few cm/sec during mass movements
- Stimulus: The most important natural stimulus is distension of the gut wall
- Dies out after traveling a variable distance — usually a few centimeters in the small intestine
- Requires an intact myenteric plexus — if destroyed (e.g., by Chagas disease), peristalsis is abolished
TYPES OF PERISTALSIS IN DIFFERENT REGIONS
Esophageal Peristalsis
- Continuation of the pharyngeal phase of swallowing
- Initiated by the swallowing center in the medulla (deglutition center)
- Travels the entire length of the esophagus in 8-10 seconds
- Upper 1/3 (striated muscle): Controlled by sequential activation via vagus nerve (nucleus ambiguus)
- Lower 2/3 (smooth muscle): Controlled by myenteric plexus with vagal modulation
- Wave speed: 3-5 cm/sec
- Initiated by local distension of the esophageal wall (e.g., retained food bolus)
- Does NOT require a swallowing reflex; purely a local reflex via intrinsic neurons
- Continues until esophagus is cleared
- Important for clearing refluxed gastric contents
- Simultaneous, disorganized contractions
- NOT propulsive
- Pathological in younger individuals; may be normal in elderly
- Seen in diffuse esophageal spasm
🔴 Clinical Correlation: Achalasia
- Pathology: Loss of inhibitory neurons (NO and VIP-producing neurons) in the myenteric plexus of the LES and distal esophagus
- Also involves loss of ganglion cells in Auerbach's plexus
- Result:
- Failure of LES relaxation with swallowing
- Aperistalsis of the esophageal body
- Increased resting LES pressure
- Symptoms: Progressive dysphagia to both solids AND liquids, regurgitation of undigested food, chest pain, weight loss
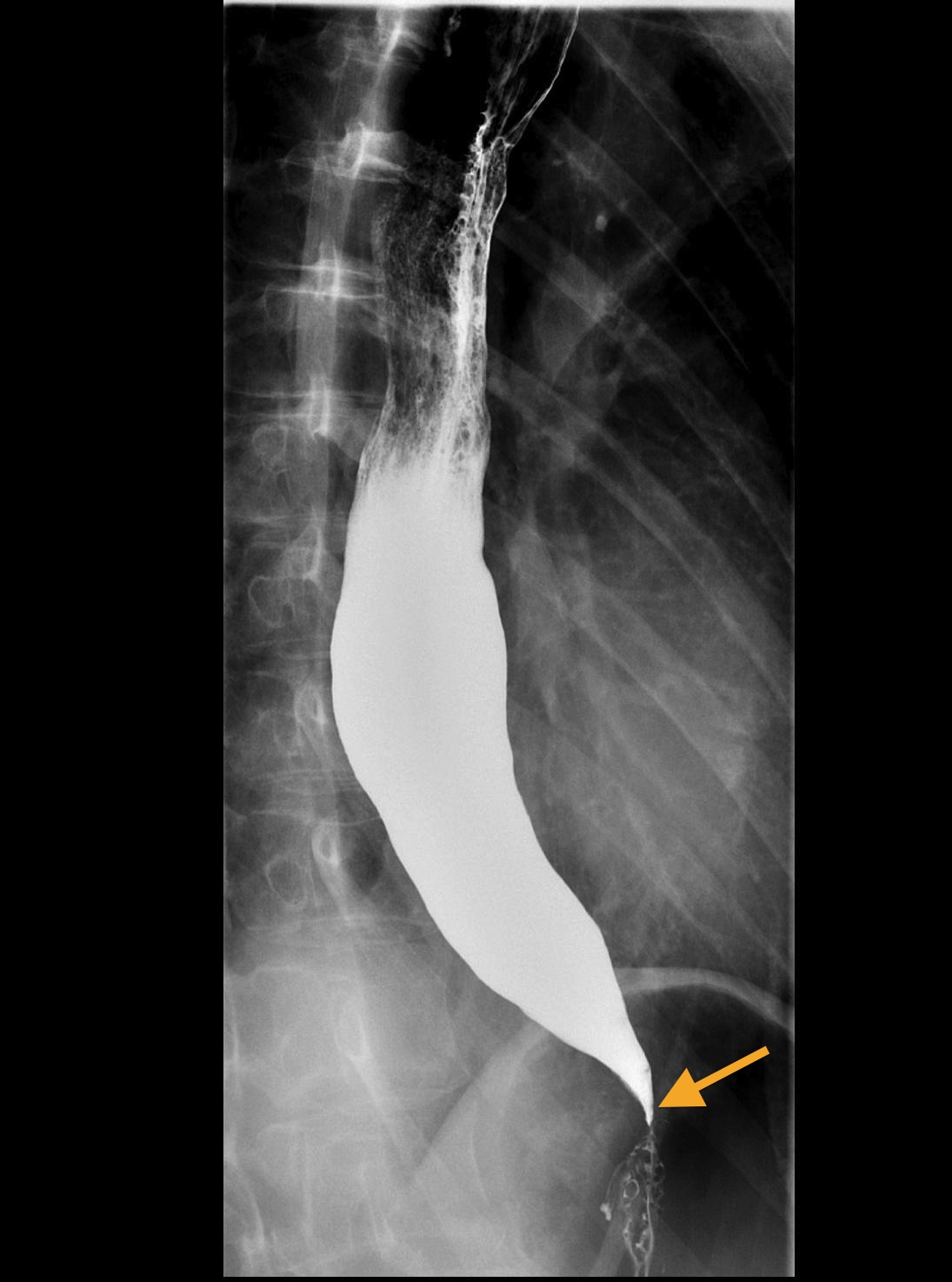


- Diagnosis:
- Barium swallow: "Bird's beak" or "rat tail" appearance at GEJ, dilated esophagus (megaesophagus)
- Esophageal manometry (Gold standard): Aperistalsis, incomplete LES relaxation, elevated resting LES pressure
- Endoscopy: To rule out pseudoachalasia (malignancy at the GEJ)
- Treatment: Pneumatic balloon dilation, Heller myotomy (laparoscopic), Peroral endoscopic myotomy (POEM), botulinum toxin injection into LES (temporary)
- Complication: Increased risk of squamous cell carcinoma of the esophagus (chronic stasis and irritation)
🔴 Clinical Correlation: Chagas Disease (American Trypanosomiasis)
- Caused by Trypanosoma cruzi (transmitted by reduviid bug — "kissing bug")
- The parasite destroys myenteric plexus neurons → secondary achalasia, megaesophagus, megacolon
- Endemic in Central and South America
- Also causes dilated cardiomyopathy
🔴 Clinical Correlation: Diffuse Esophageal Spasm
- Simultaneous, high-amplitude, non-peristaltic contractions of the esophageal body
- Manometry: Simultaneous contractions in >20% of swallows
- Barium swallow: "Corkscrew esophagus" or "rosary bead" esophagus
- Symptoms: Intermittent dysphagia and severe chest pain (can mimic angina)
- Treatment: Calcium channel blockers (nifedipine), nitrates, tricyclic antidepressants
Gastric Peristalsis
- Peristaltic waves originate from the pacemaker zone located in the mid-body of the stomach on the greater curvature
- Frequency: 3 waves per minute (set by the slow wave frequency)
- Waves become progressively stronger and faster as they move toward the pylorus
- The antrum has the strongest contractions
- Functions:
- Mixing of food with gastric secretions → formation of chyme
- Grinding of food particles (antral mill)
- Propulsion of chyme through the pylorus
- As the peristaltic wave approaches the pylorus, the pylorus closes
- The bolus of chyme is forced back into the body of the stomach (retropulsion)
- This creates powerful mixing and grinding — the antral mill
- Only particles smaller than 1-2 mm can pass through the pylorus into the duodenum
- The rate of gastric emptying is controlled by:
- Gastric factors: Volume of gastric contents (more volume = faster emptying), gastrin
- Duodenal factors (feedback inhibition):
- Fat in duodenum (most potent inhibitor) → releases CCK, GIP → slows gastric emptying
- Acid in duodenum → releases secretin → slows gastric emptying
- Hypertonicity/hypotonicity in duodenum → osmoreceptors → slows emptying
- Protein digestion products
- Distension of duodenum
- These duodenal factors act via:
- Enterogastric reflex (neural)
- Hormones: CCK, secretin, GIP, peptide YY
🔴 Clinical Correlation: Gastroparesis
- Definition: Delayed gastric emptying without mechanical obstruction
- Causes:
- Diabetic gastroparesis (most common cause) — due to vagal neuropathy and damage to ICC
- Post-surgical (vagotomy)
- Idiopathic (second most common)
- Medications (opioids, anticholinergics, GLP-1 agonists)
- Parkinson's disease, scleroderma, amyloidosis
- Symptoms: Early satiety, nausea, vomiting of undigested food, bloating, weight loss
- Diagnosis:
- Gastric emptying scintigraphy (gold standard): Retention of >10% at 4 hours is diagnostic
- Treatment:
- Dietary: Small, frequent, low-fat, low-fiber meals
- Prokinetic agents: Metoclopramide (D2 antagonist + 5-HT4 agonist; extrapyramidal side effects), Domperidone (D2 antagonist, fewer CNS effects), Erythromycin (motilin receptor agonist — most potent prokinetic, but tachyphylaxis limits long-term use)
- Gastric electrical stimulation (Enterra device)
- Pyloromyotomy (G-POEM)
🔴 Clinical Correlation: Dumping Syndrome
- Occurs after gastric surgery (gastrectomy, pyloroplasty, gastric bypass)
- Early dumping (within 15-30 minutes of eating): Rapid emptying of hyperosmolar chyme into small intestine → osmotic fluid shift → hypovolemia → cramping, diarrhea, nausea, tachycardia, diaphoresis, dizziness
- Late dumping (1-3 hours after eating): Rapid glucose absorption → exaggerated insulin release → reactive hypoglycemia → tremor, weakness, sweating, confusion
- Treatment: Small, frequent meals; avoid simple carbohydrates; lie down after meals; octreotide in refractory cases
Small Intestinal Peristalsis
- Normal peristalsis in the small intestine moves chyme at 0.5-2 cm/sec
- Each peristaltic wave dies out after 3-5 cm — transit through the entire small intestine takes 3-5 hours
- Peristalsis is markedly increased after a meal — gastroileal reflex (gastric distension enhances ileal motility and relaxes the ileocecal valve via vagus nerve and gastrin)
- A powerful peristaltic wave that travels long distances rapidly
- Caused by intense irritation of the intestinal mucosa (e.g., infectious enteritis, castor oil)
- Represents a protective mechanism to sweep irritating material quickly through the gut
- Results in diarrhea
🔴 Clinical Correlation: Paralytic Ileus (Adynamic Ileus)
- Definition: Temporary cessation of peristalsis without mechanical obstruction
- Causes:
- Post-surgical (most common — especially after abdominal surgery)
- Peritonitis, pancreatitis, retroperitoneal hemorrhage
- Hypokalemia, hypomagnesemia
- Opioid use (activate μ-receptors on myenteric neurons → inhibit ACh release)
- Anticholinergic drugs, spinal cord injury
- Presentation: Abdominal distension, absent bowel sounds, no passage of flatus/stool, nausea, vomiting
- Diagnosis: X-ray shows diffusely dilated loops of bowel (both small and large) with air-fluid levels; no transition point
- Treatment:
- NPO, nasogastric decompression, IV fluids, electrolyte correction
- Minimize opioids
- Alvimopan (peripheral μ-opioid receptor antagonist) for post-surgical ileus
- Methylnaltrexone (peripheral μ-opioid antagonist) for opioid-induced constipation
- Neostigmine especially for Ogilvie's syndrome (acute colonic pseudo-obstruction)
- Early ambulation, chewing gum (sham feeding stimulates vagal-mediated GI motility)
🔴 Clinical Correlation: Mechanical Intestinal Obstruction
- Unlike ileus, there IS a physical obstruction
- SBO: Most common cause = adhesions (prior surgery), hernias, tumors
- LBO: Most common cause = colorectal carcinoma, volvulus, diverticulitis
- Above obstruction: Vigorous peristalsis (hyperperistalsis) → high-pitched, tinkling bowel sounds
- Below obstruction: Quiet/absent bowel sounds
- Can lead to: Bowel ischemia, perforation, sepsis, death
Colonic Peristalsis
- The primary mixing movements of the colon (but also have a slow propulsive component)
- Circular muscle contracts in isolated segments creating haustra (sacculations)
- Slow, sluggish contractions
- Move contents slowly — contribute to the 12-24 hours transit time through the colon
- Allow maximum absorption of water and electrolytes
- A modified type of peristalsis unique to the colon
- A constrictive ring forms (usually in the transverse colon), and a long segment (20 cm or more) contracts as a unit, forcing fecal material en masse toward the rectum
- Duration: Contraction builds over ~30 seconds, lasts about 2-3 minutes
- Frequency: Occurs only 1-3 times per day, usually after meals
- Triggered by:
- Gastrocolic reflex: Distension of the stomach → vagal and hormonal signals → mass movement in the colon
- Duodenocolic reflex: Distension of the duodenum → colonic motility
- Both reflexes are strongest after breakfast (after the overnight fast)
- Hormones involved: Gastrin, CCK
🔴 Clinical Correlation: Irritable Bowel Syndrome (IBS)
- Functional disorder — no structural/biochemical abnormality identifiable
- Altered GI motility and visceral hypersensitivity
- IBS-D: Increased propulsive contractions, rapid transit
- IBS-C: Increased non-propulsive (segmenting) contractions, slow transit
- Rome IV criteria: Recurrent abdominal pain ≥1 day/week in the last 3 months, associated with ≥2 of: related to defecation, change in stool frequency, change in stool form
- Treatment: Low FODMAP diet, fiber, antispasmodics, loperamide (IBS-D), linaclotide/lubiprostone (IBS-C), rifaximin, psychological therapies
🔴 Clinical Correlation: Volvulus
- Twisting of the colon around its mesenteric axis → obstruction + vascular compromise
- Sigmoid volvulus (most common in adults; elderly, nursing home patients)
- X-ray: "Coffee bean sign" or "inverted U sign"
- Treatment: Sigmoidoscopic decompression + elective sigmoid resection
- Cecal volvulus (younger patients, mobile cecum)
- Treatment: Surgical (right hemicolectomy)
MIXING MOVEMENTS
Segmentation Contractions (Small Intestine)
- The primary mixing movement of the small intestine
- Mechanism: Localized, concentric contractions of circular muscle divide the intestine into small ovoid segments
- The contractions appear and disappear rhythmically at different points — chyme is "chopped" and "churned"
- Frequency: Set by the slow wave frequency:
- Duodenum: 12 per minute
- Ileum: 8-9 per minute
- This frequency gradient (higher in duodenum, lower in ileum) contributes to slow net aboral movement of chyme
- Purpose:
- Thorough mixing of chyme with digestive enzymes, bile, pancreatic juice
- Exposure of all parts of chyme to the mucosal surface for absorption
- Slows transit to allow adequate time for digestion
Pendular Movements
- Rhythmic longitudinal contractions causing intestinal segments to shorten and lengthen alternately
- Moves chyme back and forth without significant net propulsion
- Contributes to mixing; less important than segmentation
Gastric Mixing Movements
- In the stomach, mixing is achieved primarily through retropulsion with the antral mill
- When peristaltic waves reach the closed pylorus, chyme is forced backward → vigorous mixing
- The fundus and body exhibit tonic contractions that maintain steady pressure on gastric contents
SPECIFIC MOVEMENTS IN DIFFERENT REGIONS
Movements of the Esophagus
- Primary peristalsis — continuation of swallowing
- Secondary peristalsis — local distension reflex
- LES relaxation — receptive relaxation (mediated by VIP and NO via vagus nerve and myenteric plexus)
Deglutition (Swallowing)
- Oral (voluntary) phase: Tongue pushes bolus posteriorly → triggers swallowing reflex
- Pharyngeal (involuntary) phase: ~1 second; coordinated by swallowing center (NTS and nucleus ambiguus in medulla); soft palate elevation, epiglottic closure, UES relaxation
- Esophageal (involuntary) phase: Primary peristalsis propels bolus; LES relaxes via vagus-mediated receptive relaxation
🔴 Clinical Correlation: Dysphagia
- Oropharyngeal dysphagia: Difficulty initiating swallow; causes: stroke (most common), myasthenia gravis, Parkinson's, ALS, Zenker's diverticulum
- Esophageal dysphagia:
- Mechanical obstruction: Dysphagia to solids first, then liquids; causes: strictures, Schatzki ring, esophageal cancer, eosinophilic esophagitis
- Motility disorders: Dysphagia to BOTH solids AND liquids from the beginning; causes: achalasia, diffuse esophageal spasm, scleroderma (CREST syndrome)
Movements of the Stomach
- When food enters the stomach, the fundus and body relax to accommodate increasing volumes without a significant rise in intragastric pressure
- Mediated by vagovagal reflex (both afferent and efferent via vagus nerve)
- Neurotransmitter: VIP and NO
- Normal stomach accommodates up to 1.5 L with minimal pressure rise
- Further relaxation triggered by gastric wall distension (local reflex)
🔴 Clinical Correlation: Post-Vagotomy Syndromes
- Truncal vagotomy:
- Loss of receptive relaxation → rapid rise in intragastric pressure → rapid emptying of liquids
- Requires drainage procedure (pyloroplasty or gastrojejunostomy)
- Complications: dumping syndrome, diarrhea, gallstone formation
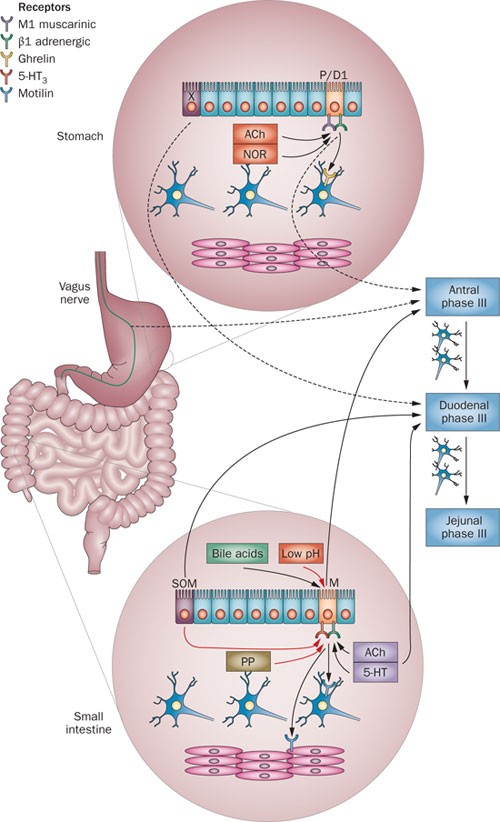
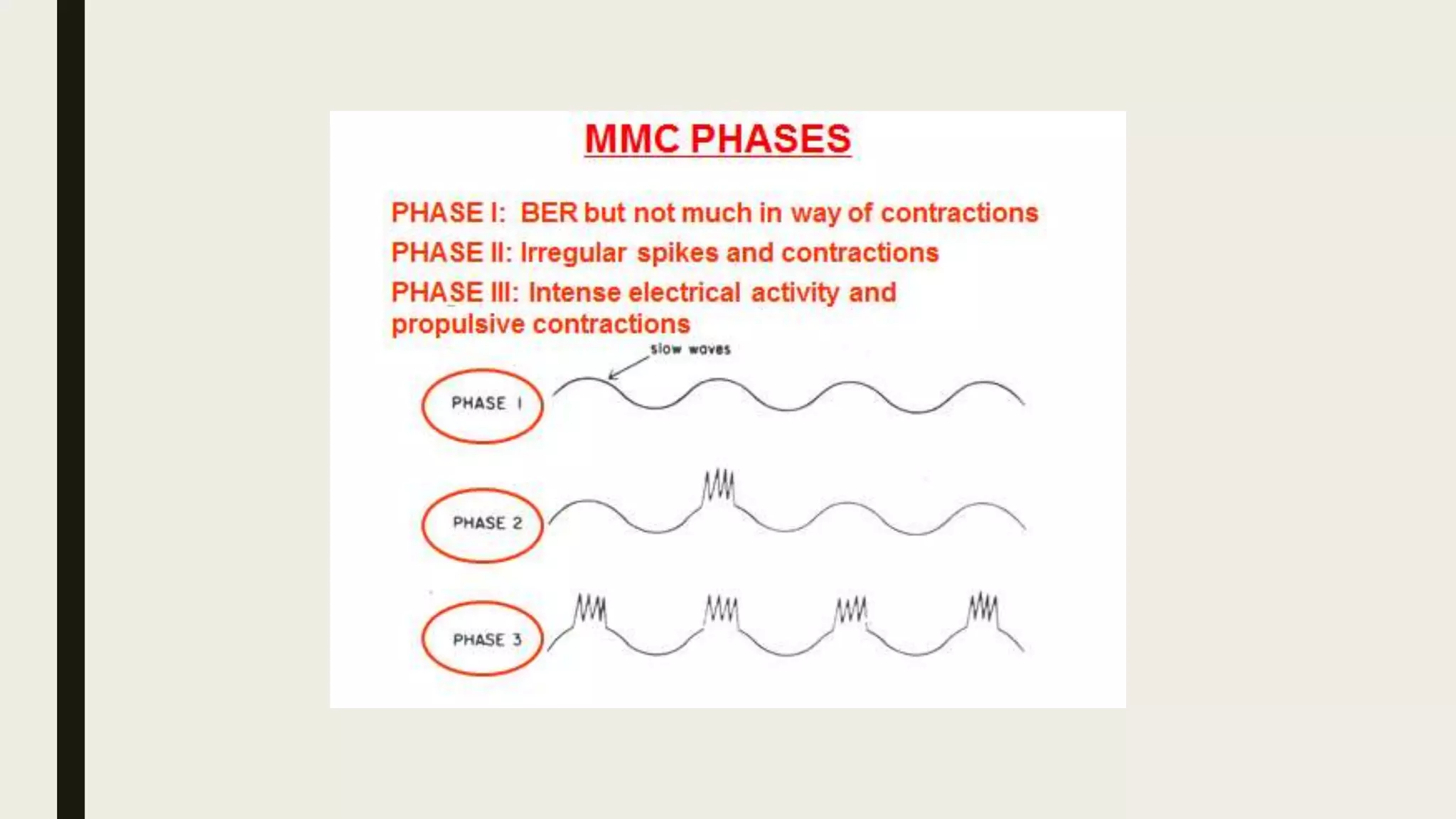
Migrating Motor Complex (MMC) / Migrating Myoelectric Complex
- A pattern of electromechanical activity that occurs during fasting (interdigestive period)
- Described by Szurszewski in 1969
- Originates in the stomach/duodenum and migrates slowly down the entire small intestine (~90-120 minutes to traverse)
- Phase I (Quiescence): ~40-60% of the cycle; no contractile activity; only slow waves, no spikes
- Phase II (Intermittent irregular contractions): ~20-30% of the cycle; increasing frequency; random spikes on slow waves
- Phase III (Regular, intense contractions): ~5-10 minutes; maximum contractile activity; every slow wave has spike bursts; the "activity front" that sweeps the gut clean
- Phase IV (Declining activity): Brief transition back to Phase I
- "Housekeeper of the gut" — Phase III sweeps residual food, bacteria, desquamated cells, and secretions from the stomach and small intestine into the colon
- Regulation:
- Motilin is the primary hormonal mediator of Phase III (released cyclically from Mo cells in duodenum and jejunum during fasting)
- Erythromycin is a motilin receptor agonist — mimics Phase III activity → prokinetic effect
- Fed state abolishes the MMC — eating triggers the "fed pattern" (segmentation + short peristaltic waves) mediated by gastrin, CCK, insulin, and vagal activity
🔴 Clinical Correlation: Small Intestinal Bacterial Overgrowth (SIBO)
- Disruption of the MMC → bacterial accumulation in the small intestine (normally <10⁴ organisms/mL)
- Causes: Diabetes (dysmotility), scleroderma, post-surgical blind loops, opioid use, achlorhydria, immunodeficiency
- Consequences: Bacterial deconjugation of bile salts → fat malabsorption → steatorrhea; B12 deficiency (folate may be elevated); carbohydrate fermentation → bloating, diarrhea
- Diagnosis: Glucose or lactulose hydrogen breath test; gold standard = jejunal aspirate with >10⁵ CFU/mL
- Treatment: Rifaximin (non-absorbable antibiotic), dietary modification, treat underlying cause, prokinetics
Movements of the Large Intestine
- Normally slightly constricted (tonic contraction) — prevents backflow of colonic contents into ileum
- Relaxed by: Gastrin (via gastroileal reflex), food in stomach
- Contracted by: Distension of cecum (cecoileal reflex), irritants in cecum
- Prevents bacterial contamination of the small intestine
Defecation Reflex
- Feces enter rectum → rectal wall distension → myenteric plexus activation → peristaltic waves in descending colon, sigmoid, and rectum → internal anal sphincter relaxation
- This reflex alone is weak — usually insufficient for complete defecation
- Afferent signals travel via pelvic nerves (S2-S4) to the sacral spinal cord
- Efferent signals return via pelvic nerves → intensify peristalsis + relax internal anal sphincter (NO and VIP)
- This is the dominant reflex
- Internal anal sphincter (IAS): Smooth muscle, autonomic (involuntary) control; normally tonically contracted (sympathetic via hypogastric nerve); relaxes during defecation (parasympathetic + enteric NO/VIP)
- External anal sphincter (EAS): Skeletal (striated) muscle, voluntary (somatic) control via pudendal nerve (S2-S4); can voluntarily contract to delay defecation
- Puborectalis muscle: Maintains anorectal angle (~90°); must relax during defecation to straighten the angle (to ~130-140°)
- Mass movement delivers feces to rectum
- Rectal distension → urge to defecate → RAIR (IAS relaxes)
- Sampling reflex: Small amount of rectal contents contacts anal canal epithelium → discriminate gas vs liquid vs solid
- If conditions are appropriate: Voluntary relaxation of EAS and puborectalis, squatting position (straightens anorectal angle), Valsalva maneuver, peristalsis evacuates rectum
- If not appropriate: Voluntary contraction of EAS → rectal accommodation → urge temporarily subsides
🔴 Clinical Correlations Related to Defecation
- Loss of EAS tone: Pudendal nerve damage (obstetric injury, surgery, diabetes)
- Loss of IAS tone: Scleroderma, aging, surgery
- Rectal prolapse
- Neurological: Cauda equina syndrome, spinal cord injury below S2
- Lesion above S2-S4 (UMN): Loss of voluntary EAS control, BUT sacral parasympathetic reflex arc is intact → reflex defecation (spastic bowel); managed with digital stimulation, suppositories
- Lesion at/below S2-S4 (LMN; cauda equina): Loss of both parasympathetic defecation reflex AND EAS voluntary control → flaccid, atonic bowel → constipation + overflow incontinence; requires manual evacuation
- Functional (most common): Inadequate fiber/fluid, sedentary lifestyle
- Slow-transit constipation: Reduced colonic motility, decreased ICC density
- Dyssynergic defecation/anismus: Failure to relax puborectalis and EAS → paradoxical contraction → diagnosed by anorectal manometry and balloon expulsion test → biofeedback treatment
SPHINCTERS OF THE GI TRACT
| Sphincter | Location | Tonic State | Key Controllers |
|---|---|---|---|
| Upper Esophageal Sphincter (UES) | Cricopharyngeus | Closed | Vagus, glossopharyngeal; opens with swallowing |
| Lower Esophageal Sphincter (LES) | GE junction | Closed (15-25 mmHg) | Intrinsic myogenic tone; VIP/NO → relaxation; ACh → contraction |
| Pyloric Sphincter | Gastroduodenal junction | Partially closed | CCK → contraction; vagal stimulation → relaxation during gastric emptying |
| Sphincter of Oddi | Ampulla of Vater | Closed | CCK → relaxation; opioids → contraction |
| Ileocecal Valve | Ileal-cecal junction | Partially closed | Discussed above |
| Internal Anal Sphincter | Anal canal | Closed | Sympathetic → contraction; parasympathetic/NO → relaxation |
| External Anal Sphincter | Anal canal | Closed | Pudendal nerve (voluntary) |
🔴 Clinical Correlation: GERD (Gastroesophageal Reflux Disease)
- Primary mechanism: Transient lower esophageal sphincter relaxations (TLESRs) — inappropriate relaxation of LES not associated with swallowing
- Other factors: Low resting LES pressure, hiatal hernia, delayed gastric emptying, impaired esophageal clearance
- Factors that DECREASE LES pressure: Chocolate, caffeine, alcohol, smoking, fatty foods, peppermint, progesterone (pregnancy), anticholinergics, calcium channel blockers, nitrates, theophylline
- Factors that INCREASE LES pressure: Gastrin, motilin, substance P, prostaglandin F2α, protein meals
- Complications: Erosive esophagitis, stricture, Barrett's esophagus (intestinal metaplasia → goblet cells → risk of esophageal adenocarcinoma), aspiration pneumonia
- Treatment: Lifestyle modifications, PPIs, H2 blockers, fundoplication (Nissen) for refractory cases
🔴 Clinical Correlation: Sphincter of Oddi Dysfunction
- Stenosis or spasm → recurrent biliary/pancreatic-type pain, elevated liver enzymes, dilated CBD
- Opioids (especially morphine) cause contraction → contraindicated in biliary colic
- CCK causes sphincter of Oddi relaxation
- Diagnosis: Sphincter of Oddi manometry
- Treatment: Endoscopic sphincterotomy
NEURAL CONTROL OF GI MOTILITY — SUMMARY
Intrinsic (Enteric) Nervous System
- "Brain of the gut" — can function independently of CNS
- ~100 million neurons
- Myenteric (Auerbach's) plexus: Between longitudinal and circular muscle layers; primarily controls motility
- Submucosal (Meissner's) plexus: In submucosa; primarily controls secretion and local blood flow
- Excitatory: ACh, Substance P (promote contraction)
- Inhibitory: NO, VIP, ATP (promote relaxation)

Extrinsic Nervous System
- Vagus nerve: Innervates esophagus through proximal 2/3 of transverse colon (entire foregut and midgut)
- Pelvic nerves (S2-S4): Innervate distal 1/3 of transverse colon through rectum and anus (hindgut)
- Generally excitatory (increases motility, relaxes sphincters, increases secretion)
- T5-L2 → celiac, superior mesenteric, inferior mesenteric, and hypogastric ganglia → post-ganglionic fibers to gut wall
- Generally inhibitory (decreases motility, contracts sphincters, decreases secretion)
- Norepinephrine acting on β2 receptors → smooth muscle relaxation
- Norepinephrine acting on α1 receptors → sphincter contraction
- Also inhibits ACh release from enteric neurons (presynaptic α2 receptors)
- Vasoconstriction of GI blood vessels (α1)
SUMMARY TABLE: GI MOVEMENTS BY REGION
| Region | Primary Mixing Movement | Primary Propulsive Movement | Frequency of Slow Waves | Special Features |
|---|---|---|---|---|
| Esophagus | None significant | Primary/secondary peristalsis | No slow waves in striated portion | Striated→smooth muscle transition |
| Stomach (fundus/body) | Tonic contraction, retropulsion | Peristalsis (weak in body) | 3/min | Receptive relaxation, reservoir |
| Stomach (antrum) | Antral mill (retropulsion) | Strong peristalsis toward pylorus | 3/min | Grinding of food |
| Duodenum | Segmentation | Peristalsis | 12/min (highest) | Origin of MMC |
| Jejunum | Segmentation | Peristalsis | 10-11/min | |
| Ileum | Segmentation | Peristalsis | 8-9/min | Gastroileal reflex |
| Colon | Haustral contractions | Mass movements (1-3/day) | 2-6/min | Gastrocolic reflex |
| Rectum | — | Defecation reflex | — | RAIR |
PART 2: GASTROINTESTINAL BLOOD FLOW — SPLANCHNIC CIRCULATION
OVERVIEW AND ANATOMY
Definition
- The GI tract (stomach, small intestine, large intestine)
- Spleen
- Pancreas
- Liver
Arterial Supply
-
Celiac trunk (artery) — supplies foregut derivatives:
- Left gastric artery → lesser curvature of stomach, lower esophagus
- Common hepatic artery → liver, gallbladder, duodenum, stomach
- Splenic artery → spleen, body/tail of pancreas, stomach (short gastric arteries)
-
Superior Mesenteric Artery (SMA) — supplies midgut derivatives:
- Inferior pancreaticoduodenal artery
- Jejunal and ileal branches
- Middle colic artery (transverse colon)
- Right colic artery (ascending colon)
- Ileocolic artery (terminal ileum, cecum, appendix)
- Supplies from lower duodenum to proximal 2/3 of transverse colon
-
Inferior Mesenteric Artery (IMA) — supplies hindgut derivatives:
- Left colic artery (descending colon)
- Sigmoid arteries
- Superior rectal artery
- Supplies from distal 1/3 of transverse colon to upper rectum
Collateral Circulation — Critical Anastomoses
- Marginal artery of Drummond: Continuous arterial arcade along the mesenteric border of the colon connecting SMA and IMA territories
- Arc of Riolan (meandering mesenteric artery): Direct connection between the middle colic artery (SMA) and left colic artery (IMA) — may be absent
- Pancreaticoduodenal arcades: Connect celiac and SMA territories
🔴 Clinical Correlation: Watershed Areas
- Splenic flexure (Griffith's point): Junction of SMA and IMA territories — most vulnerable to ischemia during low-flow states (shock, cardiac surgery, aortic surgery)
- Rectosigmoid junction (Sudeck's point): Junction of IMA (superior rectal) and internal iliac (middle and inferior rectal) territories
- These watershed areas are most susceptible to ischemic colitis
Venous Drainage — The Portal System
- Superior Mesenteric Vein (SMV) + Splenic Vein = Portal Vein (behind the neck of the pancreas)
- Inferior Mesenteric Vein (IMV) usually joins the splenic vein (or SMV, or the junction)
- Length: ~8 cm
- Carries 75% of total hepatic blood flow (~1050 mL/min) but only 50% of oxygen delivery
- Contains nutrient-rich, partially deoxygenated blood
- Pressure: 5-10 mmHg normally
- Carries 25% of total hepatic blood flow (~300 mL/min) but 50% of oxygen delivery
- Contains fully oxygenated blood
- Reciprocal relationship: If portal flow decreases, hepatic arterial flow increases (hepatic arterial buffer response — mediated by adenosine washout mechanism)
🔴 Clinical Correlation: Portal Hypertension
- Definition: Portal vein pressure >12 mmHg (or hepatic venous pressure gradient >5 mmHg; clinically significant if >10 mmHg)
- Most common cause: Liver cirrhosis (intrahepatic, sinusoidal)
- Classification:
- Pre-hepatic: Portal vein thrombosis, splenic vein thrombosis
- Intrahepatic:
- Pre-sinusoidal: Schistosomiasis (most common cause worldwide), primary biliary cholangitis, sarcoidosis
- Sinusoidal: Cirrhosis (most common cause in Western countries)
- Post-sinusoidal: Veno-occlusive disease (sinusoidal obstruction syndrome)
- Post-hepatic: Budd-Chiari syndrome (hepatic vein thrombosis), constrictive pericarditis, right heart failure

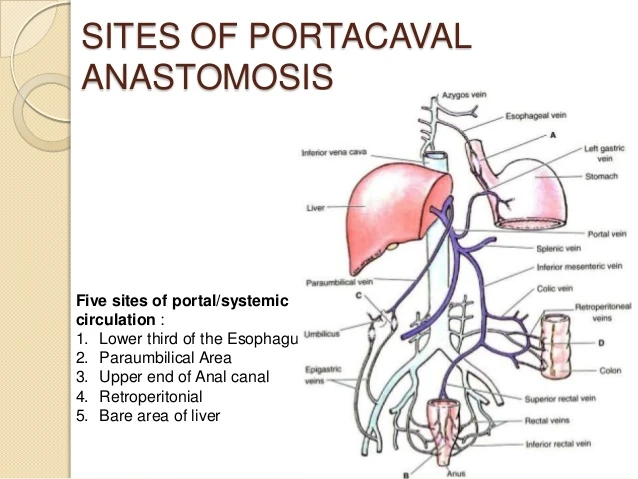
| Site | Portal Vessel | Systemic Vessel | Clinical Manifestation |
|---|---|---|---|
| Lower esophagus/gastric fundus | Left gastric vein (coronary vein) | Esophageal branches of azygos vein | Esophageal/gastric varices (most dangerous — rupture → massive upper GI bleeding) |
| Rectum | Superior rectal vein | Middle and inferior rectal veins (internal iliac) | Anorectal varices (NOT hemorrhoids) |
| Periumbilical | Paraumbilical veins (via round ligament) | Superficial epigastric veins | Caput medusae |
| Retroperitoneal | Colic/intestinal veins | Renal, lumbar, gonadal veins | Retroperitoneal varices |
| Bare area of liver | Portal branches | Diaphragmatic veins | — |

- Other manifestations: Splenomegaly (congestive), ascites, hepatorenal syndrome, hepatic encephalopathy (portosystemic shunting of ammonia)
- Treatment of variceal bleeding: Resuscitation, octreotide/terlipressin (reduce splanchnic blood flow), emergent endoscopy with band ligation or sclerotherapy, balloon tamponade (Sengstaken-Blakemore tube) as bridge, TIPS (transjugular intrahepatic portosystemic shunt), propranolol/nadolol (non-selective β-blockers) for primary/secondary prophylaxis
BLOOD FLOW DISTRIBUTION IN THE GI TRACT
Magnitude
- Total splanchnic blood flow at rest: approximately 1400-1800 mL/min (25-30% of cardiac output)
- After a meal: Can increase to 2000-2500 mL/min or more
- Distribution:
- Liver: ~1350 mL/min (portal 1050 + hepatic arterial 300)
- Small intestine: Receives the largest share of mesenteric flow
- Stomach, colon, pancreas, spleen: Remainder
Microcirculation of the Intestinal Villus
- A single arteriole ascends in the center of the villus to the tip
- Blood flows up the arteriole and returns via venules/capillaries surrounding it, flowing downward
- The arteriole and venules run in close proximity in a countercurrent arrangement
- Oxygen diffuses from the ascending arteriole to the descending venules at every level of the villus
- This creates an oxygen gradient: highest at the base, lowest at the tip
- The tip of the villus is relatively hypoxic even under normal conditions (PO₂ at villus tip can be as low as 10-20 mmHg vs. 60-70 mmHg at the base)
- The villus tip is the most vulnerable to ischemic injury
- During reduced blood flow (shock, hypotension), villus tip undergoes ischemic necrosis first
- This manifests as villus sloughing and loss of mucosal barrier
🔴 Clinical Correlation: Neonatal Necrotizing Enterocolitis (NEC)
- Primarily affects premature infants
- Ischemic necrosis of intestinal mucosa (especially terminal ileum and proximal colon)
- Pathogenesis: Immature gut + immature circulation + bacterial colonization → intestinal ischemia → necrosis → bacterial translocation → sepsis
- Pneumatosis intestinalis (gas within the bowel wall) on X-ray is pathognomonic
- Portal venous gas on X-ray indicates severe disease
- Treatment: NPO, nasogastric decompression, IV antibiotics, surgery if perforation
REGULATION OF SPLANCHNIC BLOOD FLOW
Intrinsic (Local) Regulation
1. Metabolic Autoregulation (Functional Hyperemia)
- Most important mechanism for increasing GI blood flow after a meal
- Active digestion and absorption → increased metabolic activity → local release of vasodilator metabolites:
- Adenosine (most important)
- CO₂
- K⁺
- H⁺
- Decreased O₂
- These cause arteriolar dilation → increased blood flow
- Blood flow can increase 50-100% or more after a meal (postprandial hyperemia)
2. Myogenic Autoregulation (Bayliss Effect)
- Smooth muscle in arteriolar walls responds to stretch (increased transmural pressure) by contracting
- Maintains relatively constant blood flow when arterial pressure changes
- Effective over MAP range of approximately 60-140 mmHg
- Below 60 mmHg → autoregulation fails → flow becomes pressure-dependent
3. Mucosal Blood Flow and the "Villus Pump"
- Rhythmic contractions of the villus (via muscularis mucosae) create a pumping action
- Promotes blood flow through the villus capillaries
Hormonal Regulation
| Hormone | Effect on GI Blood Flow |
|---|---|
| Gastrin | Increases mucosal blood flow (stomach) |
| CCK | Increases blood flow to pancreas and small intestine |
| Secretin | Increases pancreatic blood flow |
| Glucagon | Vasodilation → increases splanchnic blood flow |
| VIP | Potent vasodilator → increases mucosal blood flow |
| Substance P | Vasodilation |
| Vasopressin (ADH) | Splanchnic vasoconstriction (used therapeutically in variceal bleeding) |
| Angiotensin II | Splanchnic vasoconstriction |
- Kinins (bradykinin, kallidin): Released by exocrine glands during secretory activity → potent vasodilation → increased glandular blood flow during secretion
Neural Regulation
Parasympathetic (Vagus and Pelvic Nerves)
- Indirect vasodilation: Stimulates glandular secretion and motility → increased metabolic activity → local metabolic vasodilation
- Also releases VIP from enteric neurons → direct vasodilation
- The parasympathetic effect on blood flow is primarily indirect (via increased metabolic activity)
Sympathetic
- Direct innervation of arterioles, venules, and arteries in the GI tract
- Neurotransmitter: Norepinephrine
- α₁ receptors (predominant) → vasoconstriction
- During sympathetic activation (exercise, hemorrhage, shock):
- Intense splanchnic vasoconstriction → shunts blood to skeletal muscles, heart, brain
- Splanchnic circulation serves as a blood reservoir (~20-30% of blood volume can be mobilized)
- Splanchnic venoconstriction (α₁ on venous capacitance vessels) → mobilizes blood from the splanchnic venous reservoir → increases venous return to the heart
- During sustained sympathetic stimulation, the initial vasoconstriction of gut arterioles gradually wanes after 1-3 minutes
- Blood flow partially returns toward normal despite continued sympathetic discharge
- Mechanism: Local metabolic vasodilators (adenosine, etc.) accumulate due to ischemia and overcome the sympathetic vasoconstrictor effect
- Significance: Protects the gut from prolonged ischemia during sympathetic activation (e.g., exercise)
- However, during severe, prolonged shock, autoregulatory escape may be overwhelmed → mucosal ischemia → barrier breakdown → bacterial translocation → sepsis → MODS
🔴 Clinical Correlation: Shock and GI Tract (Ischemic Gut)
- During hemorrhagic/cardiogenic/septic shock:
- Intense sympathetic-mediated splanchnic vasoconstriction redistributes blood to vital organs
- Prolonged ischemia → mucosal barrier breakdown → bacterial translocation (bacteria and endotoxin cross into portal blood and systemic circulation)
- Contributes to SIRS (Systemic Inflammatory Response Syndrome) and MODS
- The gut has been called the "motor of MODS" or "motor of multiple organ failure"
- Non-occlusive mesenteric ischemia (NOMI): Mesenteric vasoconstriction without arterial/venous occlusion, seen in:
- Low-flow states (heart failure, shock)
- Vasopressor use (norepinephrine, vasopressin, digitalis)
- Cocaine use, hemodialysis
- Treatment: Papaverine infusion via mesenteric catheter, correct underlying cause
MESENTERIC ISCHEMIA — DETAILED CLINICAL CORRELATIONS
Acute Mesenteric Ischemia
- SMA embolism (50%) — most common cause
- Source: Left atrial thrombus (AF), LV mural thrombus (post-MI), valvular disease
- Sudden onset; embolus typically lodges just distal to the origin of the middle colic artery
- SMA thrombosis (15-25%)
- Usually on pre-existing atherosclerotic plaque at the origin of the SMA
- History of chronic mesenteric ischemia (intestinal angina) may precede
- Mesenteric venous thrombosis (5-15%)
- Associated with hypercoagulable states (Factor V Leiden, protein C/S deficiency, antiphospholipid syndrome), portal hypertension, intra-abdominal inflammation
- More insidious onset
- Non-occlusive mesenteric ischemia (NOMI) (20-30%)
- Severe, diffuse, periumbilical abdominal pain
- Early: Pain is severe but abdomen is soft and non-tender (the discrepancy is the hallmark)
- Late: Peritonitis (guarding, rigidity, rebound) — indicates bowel infarction
- Bloody diarrhea (if hemorrhagic infarction)
- Nausea, vomiting
- Leukocytosis, elevated lactate, metabolic acidosis (late findings indicating infarction)
- CT angiography (best initial test) — shows vascular occlusion and bowel wall changes
- Conventional angiography (gold standard for diagnosis AND treatment of NOMI)
- Elevated serum lactate, D-dimer (sensitive but not specific)
- Fluid resuscitation, broad-spectrum antibiotics
- SMA embolism/thrombosis: Surgical embolectomy/thrombectomy + resection of necrotic bowel; catheter-directed thrombolysis if no peritonitis; anticoagulation
- NOMI: Intra-arterial papaverine; optimize cardiac output; avoid vasoconstrictors
- Venous thrombosis: Anticoagulation (heparin → warfarin)
Chronic Mesenteric Ischemia (Intestinal Angina)
- Atherosclerotic narrowing of at least 2 of 3 mesenteric arteries (celiac, SMA, IMA)
- Postprandial abdominal pain ("intestinal angina") — 15-30 minutes after eating
- Weight loss (patients develop sitophobia — fear of eating due to pain)
- Diagnosis: CTA or MRA, duplex ultrasound of mesenteric vessels
- Treatment: Mesenteric revascularization (angioplasty + stenting or surgical bypass)
Ischemic Colitis
- Most common form of mesenteric ischemia overall
- Usually affects watershed areas (splenic flexure, rectosigmoid junction)
- Typical patient: Elderly with cardiovascular disease, after aortic surgery
- Presentation: Sudden onset of crampy left-sided abdominal pain, urgency to defecate, bloody diarrhea
- Usually non-gangrenous (transient/self-limited in ~85% of cases)
- Diagnosis: CT, colonoscopy (edema, hemorrhage, ulceration; "thumbprinting" on barium enema or CT = submucosal hemorrhage/edema)
- Treatment: Supportive (IV fluids, bowel rest, antibiotics if severe); surgery if gangrenous/perforated
HEPATIC CIRCULATION IN DETAIL
Dual Blood Supply
- Portal vein: 75% of flow, 50% of O₂
- Hepatic artery: 25% of flow, 50% of O₂
- Total hepatic blood flow: ~1350-1500 mL/min (25-30% of cardiac output)
Hepatic Sinusoids
- Specialized capillaries of the liver
- Receive mixed blood from both portal venules and hepatic arterioles
- Fenestrated endothelium (discontinuous) with no basement membrane → allows free exchange of plasma proteins and nutrients with hepatocytes
- Contain Kupffer cells (resident macrophages) — phagocytose bacteria, endotoxins, old RBCs from portal blood
- Blood flows from portal triads (at periphery of lobule) → through sinusoids → to central vein (center of lobule) → hepatic veins → IVC
Hepatic Zones (Rappaport Acinus Model)
- Zone 1 (periportal): Closest to blood supply; most oxygenated; highest metabolic activity for gluconeogenesis, urea synthesis, bile formation; most resistant to ischemia
- Zone 2 (mid-zone): Intermediate
- Zone 3 (pericentral/centrilobular): Farthest from blood supply; most hypoxic; most susceptible to ischemic necrosis (centrilobular necrosis — seen in shock, CHF, hepatic vein obstruction); most active in drug metabolism (cytochrome P450), lipogenesis, glycolysis; where acetaminophen toxicity damage is worst
Hepatic Arterial Buffer Response (HABR)
- If portal blood flow decreases, hepatic arterial flow automatically increases to compensate
- Mechanism: Adenosine washout hypothesis
- Adenosine is constitutively produced in the space of Mall (periportal space)
- Normal portal flow washes it away → keeps hepatic arterioles at baseline tone
- When portal flow decreases → adenosine accumulates → causes hepatic arteriolar vasodilation → increased hepatic arterial flow
- This is NOT reciprocal — hepatic arterial flow changes do NOT affect portal flow
- Clinical significance: Maintains hepatic oxygen delivery when portal flow is compromised
🔴 Clinical Correlation: Budd-Chiari Syndrome
- Thrombosis/obstruction of hepatic veins (or IVC at the hepatic level)
- Classic triad: Hepatomegaly, ascites, abdominal pain
- Causes: Myeloproliferative neoplasms (most common; especially polycythemia vera — JAK2 mutation), hypercoagulable states, oral contraceptives, pregnancy, paroxysmal nocturnal hemoglobinuria
- Nutmeg liver on pathology (centrilobular congestion and necrosis)
- Diagnosis: Doppler ultrasound (absence of hepatic venous flow), CT/MRI, hepatic venography
- Treatment: Anticoagulation, TIPS, liver transplantation (severe cases)
BLOOD RESERVOIR FUNCTION OF THE SPLANCHNIC CIRCULATION
- The splanchnic venous system (especially the liver, spleen, and mesenteric veins) is a major capacitance reservoir
- Normally holds 20-30% of total blood volume (~1000-1500 mL)
- During hemorrhage/shock:
- Sympathetic activation → α₁-mediated venoconstriction → mobilizes up to 500-1000 mL of blood from the splanchnic reservoir into the systemic circulation
- One of the most important compensatory mechanisms to maintain cardiac output and blood pressure
- During exercise:
- Splanchnic vasoconstriction redistributes blood to skeletal muscles
- Splanchnic blood flow can decrease by 50-80% during vigorous exercise
- Explains why vigorous exercise after a meal causes GI cramps ("side stitches")
🔴 Clinical Correlation: Exercise-Related GI Symptoms
- Common in endurance athletes: "Runner's diarrhea," abdominal cramps, nausea, GI bleeding
- Mechanisms: Splanchnic hypoperfusion during exercise + mechanical trauma (running)
- Can cause ischemic colitis in extreme cases
- Prevention: Avoid eating close to exercise, adequate hydration, training adaptation
POSTPRANDIAL HYPEREMIA — INTEGRATED RESPONSE
- Metabolic factors (most important): Increased mucosal metabolic activity → adenosine, CO₂, K⁺, H⁺ → arteriolar dilation
- GI hormones: Gastrin, CCK, secretin, VIP, glucagon → vasodilation
- Parasympathetic activation: Vagal stimulation → increased secretion and motility → increased metabolic activity → indirect vasodilation; also VIP release → direct vasodilation
- Kinins: Released during glandular secretion → vasodilation
- Decreased sympathetic tone to splanchnic bed after eating
- Serotonin (5-HT): Released from enterochromaffin cells during mucosal stimulation → local vasodilation
- Food enters stomach → gastrin release → gastric mucosal blood flow increases
- Chyme enters duodenum → CCK, secretin release → pancreatic, duodenal blood flow increases
- As chyme moves along small intestine → local metabolic hyperemia follows the wave of digestion/absorption
🔴 Clinical Correlation: Postprandial Hypotension
- Seen in elderly, patients with autonomic dysfunction (diabetes, Parkinson's, multiple system atrophy), dialysis patients
- After a meal → splanchnic vasodilation → blood pooling in splanchnic bed → if sympathetic compensation is impaired → drop in systemic BP → syncope, falls
- Defined as: Drop in systolic BP ≥20 mmHg within 2 hours of a meal
- Management: Small, frequent meals; low carbohydrate content; adequate hydration; caffeine (adenosine antagonist — reduces splanchnic vasodilation); minimize antihypertensives before meals; octreotide (inhibits release of vasodilatory GI peptides)
🔴 Clinical Correlation: Abdominal Angina / Chronic Mesenteric Ischemia (revisited)
- Postprandial hyperemia cannot be achieved due to stenotic mesenteric arteries → supply-demand mismatch → ischemic pain after eating
SPECIAL CIRCULATIONS WITHIN THE SPLANCHNIC BED
Splenic Circulation
- Splenic artery (from celiac trunk) → enters hilum → branches into trabecular arteries → central arteries → penicillar arteries → open circulation (blood spills into splenic cords of red pulp → percolates through → re-enters splenic sinuses → splenic vein)
- Functions: Filtration of old/abnormal RBCs, immune surveillance, blood reservoir (~250 mL in normal spleen)
- Splenomegaly (e.g., in portal hypertension) → increased blood sequestration → hypersplenism (pancytopenia)
Pancreatic Circulation
- Dual blood supply: Branches from celiac trunk (via splenic artery and gastroduodenal → superior pancreaticoduodenal) and SMA (inferior pancreaticoduodenal)
- Blood flow increases significantly during secretion (stimulated by CCK, secretin)
- Islets of Langerhans have a specialized microvasculature: insulo-acinar portal system — blood flows from islets → surrounding exocrine tissue → insulin modulates exocrine function
KEY CLINICAL CORRELATIONS — SUMMARY TABLE
| Condition | Pathophysiology | Key Finding |
|---|---|---|
| Achalasia | Loss of inhibitory neurons (NO/VIP) in LES | Bird's beak on barium swallow; aperistalsis on manometry |
| Hirschsprung's | Absent ganglion cells in distal colon | Absent RAIR; transition zone on barium enema |
| GERD | Transient LES relaxations; low LES pressure | Heartburn; Barrett's esophagus |
| Gastroparesis | Impaired gastric emptying (vagal neuropathy, loss of ICC) | Delayed gastric emptying on scintigraphy |
| Paralytic ileus | Absent peristalsis without obstruction | Diffuse dilated bowel; no bowel sounds |
| SIBO | Loss of MMC "housekeeper" function | B12 deficiency with elevated folate |
| Acute mesenteric ischemia | SMA embolism/thrombosis, NOMI | Pain out of proportion to exam; elevated lactate |
| Ischemic colitis | Watershed ischemia | Thumbprinting; splenic flexure involvement |
| Portal hypertension | Increased resistance to portal flow | Varices, ascites, caput medusae, splenomegaly |
| Dumping syndrome | Rapid gastric emptying post-surgery | Early (osmotic) and late (hypoglycemic) symptoms |
| Diffuse esophageal spasm | Simultaneous non-peristaltic contractions | Corkscrew esophagus |
| Chagas disease | Trypanosoma cruzi destroys myenteric plexus | Megaesophagus, megacolon |
| Postprandial hypotension | Impaired sympathetic compensation for splanchnic vasodilation | Syncope after meals in elderly/dysautonomia |
| Autoregulatory escape | Local metabolites overcome sympathetic vasoconstriction | Partial restoration of gut blood flow during sustained sympathetic stimulation |
| Budd-Chiari syndrome | Hepatic vein thrombosis | Hepatomegaly, ascites, pain; nutmeg liver |
| NEC | Villus tip ischemia in premature infants | Pneumatosis intestinalis on X-ray |
Images integrated throughout this document include:
- ICC network and slow wave genesis (electrical basis of GI motility)
- GI smooth muscle action potential diagram (slow waves + spikes + contraction)
- Enteric neural circuitry for the peristaltic reflex (ascending excitatory, descending inhibitory)
- Peristaltic mechanism diagram (law of the intestine - contraction/relaxation pattern)
- Achalasia: barium swallow bird's beak sign (2 radiological images)
- Achalasia: high-resolution manometry subtypes
- Migrating Motor Complex: Phase diagram from Nature Reviews Gastroenterology
- MMC cyclical phases diagram
- Enteric nervous system wall layers diagram
- Portal hypertension: portosystemic anastomoses full diagram
- Portal hypertension: AMBOSS clinical diagram (varices, caput medusae, splenomegaly, ascites)
- Portacaval anastomosis labeled vessels diagram