Transverse mylites its causes , clinical features and gold standard clinical features , physiotherapy treatment in acute phase and immediately
Reading File
Finding Sources
Searching the Web
transverse myelitis causes clinical features gold standard diagnosis physiotherapy treatment acute phase
Searching PubMed
"transverse myelitis"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC8896909
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Transverse Myelitis (TM)
Definition
Transverse myelitis is an acute or subacute focal inflammatory disorder of the spinal cord causing demyelination and/or necrosis that interrupts ascending and descending pathways. The term "transverse" refers to involvement of the full cross-section of the cord at a given level. It affects approximately 1 in 100,000 people.
- ROSEN's Emergency Medicine, p. 1508
Causes / Etiology
TM is pathogenetically heterogeneous. A cause is not identified in ~30% of patients (idiopathic TM).
1. Post-infectious / Para-infectious (most common, ~30%)
- Follows viral infection (e.g., herpes simplex, varicella-zoster, cytomegalovirus, Epstein-Barr virus, HIV, West Nile virus, COVID-19)
- Bacterial: mycoplasma, Lyme disease (rare)
- Post-vaccination (rare)
2. Autoimmune / Demyelinating CNS Diseases
- Multiple sclerosis (MS) - partial/asymmetric TM is a common presenting feature
- Neuromyelitis Optica Spectrum Disorder (NMOSD) - associated with anti-aquaporin-4 (anti-AQP4) antibodies; causes longitudinally extensive TM (LETM) spanning 3+ vertebral levels
- MOG Antibody Disease (MOGAD) - anti-myelin oligodendrocyte glycoprotein antibodies
- Acute disseminated encephalomyelitis (ADEM)
3. Systemic Autoimmune / Connective Tissue Diseases
- Systemic lupus erythematosus (SLE)
- Sjogren syndrome
- Antiphospholipid antibody syndrome
- Vasculitis, sarcoidosis
- Mixed connective tissue disease, rheumatoid arthritis, scleroderma, Behcet disease
- Goldman-Cecil Medicine, p. 3995
4. Vascular
- Spinal cord ischemia / infarction (dural venous fistula, antiphospholipid syndrome)
5. Paraneoplastic
- Associated with occult malignancy
Clinical Features
Symptoms typically develop rapidly - 66% of patients reach maximal deficit within 24 hours, though progression can occur over days to weeks. The thoracic cord is most frequently affected (60-70% of cases).
1. Motor Deficits
- Bilateral weakness (paraparesis or paraplegia) - may be asymmetrical
- Progresses to spasticity with upper motor neuron signs: hypertonia, hyperreflexia, clonus, positive Babinski response
- In early/acute phase: spinal shock may produce flaccid paralysis with hyporeflexia
2. Sensory Deficits
- Clearly defined sensory level on the trunk - hallmark finding
- Ascending paresthesias (numbness, tingling, burning)
- Loss of deep sensation (proprioception, vibration) in feet
- All modalities below the lesion affected in complete TM
3. Autonomic / Sphincter Dysfunction
- Urinary retention or incontinence (bladder is involved in nearly all patients)
- Fecal retention or incontinence
- Sexual dysfunction
- Autonomic instability in high cervical/thoracic lesions: hyper- or hypotension, tachy- or bradycardia
4. Pain
- Neck or back pain is common at onset
- Low-grade fever may be present (raises concern for septic epidural abscess as differential)
Complete vs. Partial TM
- Complete (LETM): total loss of all motor, sensory, and sphincter function below the level - hallmark of NMOSD
- Partial TM: incomplete, asymmetric deficits - more associated with MS
Gold Standard Diagnosis
Primary Investigation: MRI Spine with Gadolinium
MRI with gadolinium contrast is the diagnostic modality of choice for suspected TM. It serves dual purposes: confirming cord inflammation and excluding compressive/structural causes.
MRI findings:
- T2-weighted images: focal hyperintense (bright) signal within the spinal cord - present in 50-90% of adults
- T1-weighted images: iso- or mildly hypointense signal; cord swelling over several segments
- Gadolinium enhancement: indicates active inflammation (enhancement occurs within 7 days of onset)
- LETM: T2 signal spanning 3 or more vertebral levels - strongly suggests NMOSD
Supporting Investigations
| Investigation | Finding |
|---|---|
| CSF analysis | Lymphocytic pleocytosis + elevated protein (normal in 40% of cases) |
| CSF IgG index | Elevated in demyelinating TM |
| Serum anti-AQP4 antibodies | Positive in NMOSD |
| Serum anti-MOG antibodies | Positive in MOGAD |
| ANA, anti-dsDNA, antiphospholipid antibodies | Screen for connective tissue disease |
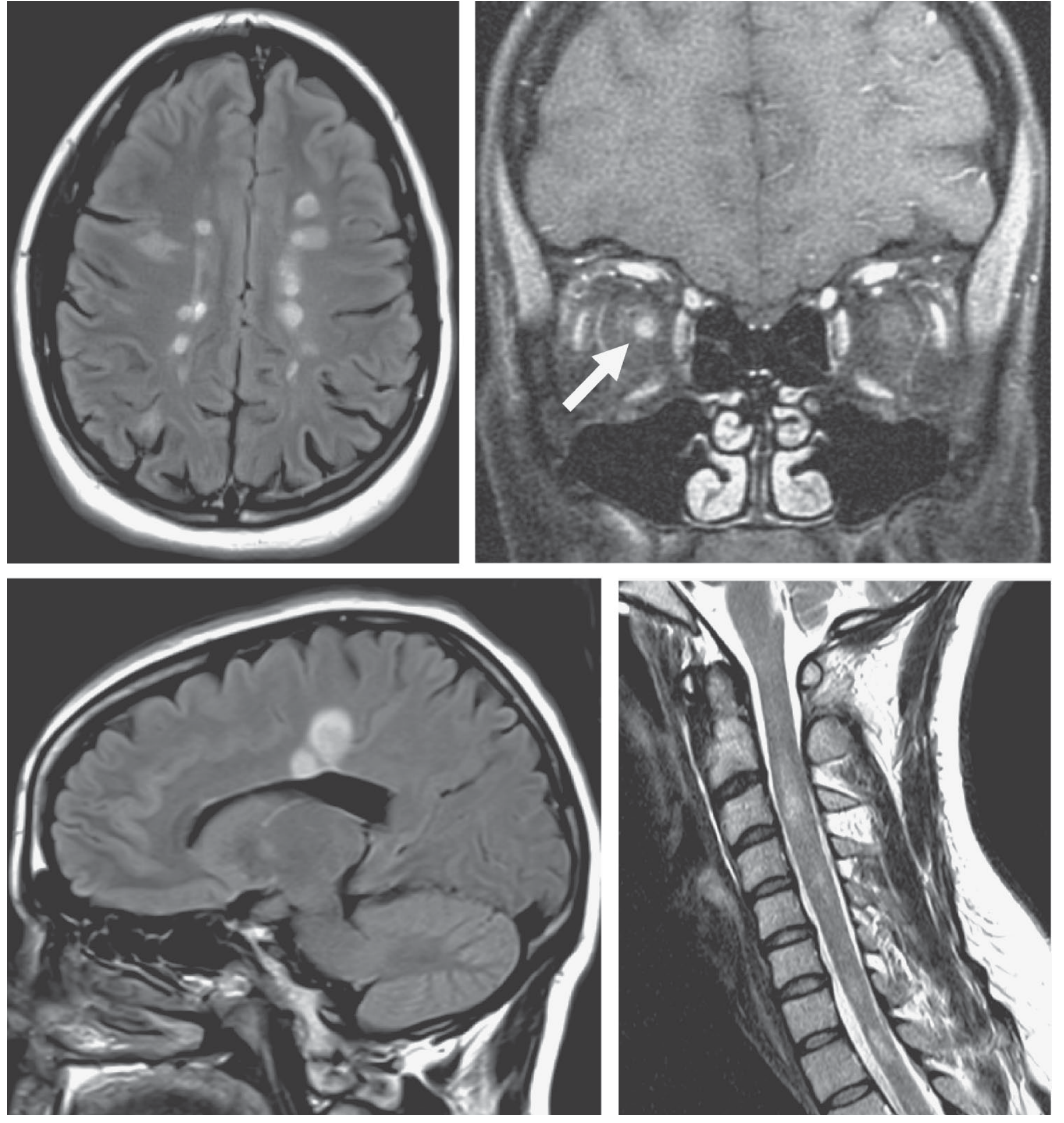
| Brain MRI | Periventricular lesions suggest MS |
| Visual evoked potentials | May show subclinical optic pathway involvement |
Diagnostic Criteria (Transverse Myelitis Consortium Working Group 2002)
- Neurologic symptoms attributable solely to the spinal cord
- Bilateral signs/symptoms (may be asymmetric)
- Clearly defined sensory level
- MRI exclusion of cord compression
- Inflammation in cord: CSF pleocytosis, elevated IgG index, OR gadolinium enhancement (within 7 days)
- Progressive worsening peaking between 4 hours and 21 days after onset
- No other etiology (infection, neoplasm, trauma, vascular, nutritional deficiency)
ROSEN's Emergency Medicine, p. 1508; MedLink Neurology
Physiotherapy Treatment
Acute Phase - Immediate Goals
In the acute phase, physiotherapy begins as soon as the patient is medically stable. The overarching strategy is activity-based rehabilitation with emphasis on impairment management and prevention of secondary complications.
1. Positioning and Skin Care
- Correct limb positioning to prevent contractures and pressure injuries
- Regular 2-hourly turning schedule
- Use of pressure-relieving mattresses/cushions
- Splinting of ankles/wrists in neutral to prevent deformity
2. Passive Range of Motion (PROM) Exercises
- All paralyzed limb joints taken through full range of motion daily
- Maintains joint mobility and prevents contractures
- Prevents deep vein thrombosis (DVT) by promoting venous return
- Focus on: hip, knee, ankle (dorsiflexion), shoulder, elbow, wrist
3. Respiratory Physiotherapy (especially cervical/high thoracic lesions)
- Intercostal and diaphragmatic breathing exercises
- Assisted coughing techniques (manual costal compression)
- Incentive spirometry
- Postural drainage and percussion if secretions present
- Aim: prevent pneumonia and respiratory failure
4. Edema Management
- Elevation of limbs
- Compression stockings/bandaging to prevent dependent edema
- Early gentle massage
5. Spasticity Management
- Stretching programs (sustained slow stretching)
- Neutral positioning
- Splinting
- Preparation for pharmacological management (baclofen, tizanidine - to be coordinated with medical team)
6. Neuromuscular Stimulation
- Electrical stimulation (NMES/FES) to maintain muscle bulk and facilitate motor return
- Sensory stimulation to affected areas
7. Active Exercises (when voluntary movement present)
- Active-assisted to active range of motion exercises as tolerated
- Strengthening of partially preserved muscle groups
- Neuromuscular re-education
8. Bladder and Bowel Management
- Bladder rehabilitation: timed voiding, pelvic floor exercises if possible
- Intermittent catheterization program coordination with nursing
9. Early Mobilization (when hemodynamically stable)
- Head-of-bed elevation to prevent orthostatic hypotension
- Tilt table standing (graded)
- Transfer training (bed to chair)
- Wheelchair mobility if applicable
10. Psychological Support
- Reassurance and education of patient and family
- Goal setting and explanation of recovery trajectory
Summary Table: Acute Phase Physiotherapy
| Problem | Physiotherapy Intervention |
|---|---|
| Paralysis / weakness | PROM, AROM, strengthening, neuromuscular re-education |
| Contracture risk | Positioning, stretching, splinting |
| Pressure sores | Turning schedule, positioning aids |
| Respiratory compromise | Breathing exercises, assisted cough |
| Spasticity | Sustained stretch, positioning, splinting |
| DVT risk | PROM, compression, early mobilization |
| Orthostatic hypotension | Graded tilt, abdominal binders |
| Bladder/bowel | Pelvic floor re-education, program coordination |
Medical Treatment (for context)
- First-line: IV methylprednisolone 1000 mg/day for 3-5 days
- Refractory cases: Plasma exchange (IVIG or plasmapheresis), cyclophosphamide
- NMOSD: Long-term immunosuppression (azathioprine, rituximab, satralizumab, eculizumab)
Prognosis
- ~30% good recovery, 25% fair, 30% poor, 15% mortality in severe cases
- Recovery begins within 1-3 months; maximal improvement by 3-6 months
- Poor prognostic factors: rapid onset to nadir (<24 hours), complete cord involvement, NMOSD
Sources: Bradley and Daroff's Neurology in Clinical Practice | ROSEN's Emergency Medicine | Goldman-Cecil Medicine | Adams and Victor's Principles of Neurology | Tintinalli's Emergency Medicine | PMC physiotherapy case report | BMJ Best Practice (reviewed June 2026)
This is a shared conversation. Sign in to Orris to start your own chat.