Teach me everything about liver function test
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Liver Function Tests (LFTs) - Complete Guide
Liver function tests (LFTs) are a panel of blood tests used to assess liver health, detect injury, and monitor liver disease. A key point: most "LFTs" are not actually measures of liver function - many are markers of liver injury. True synthetic function is only measured by albumin and prothrombin time (PT/INR).
1. Why the Liver is Tested
The liver performs hundreds of functions (Harrison's Principles of Internal Medicine, 22nd ed.):
- Synthesis of serum proteins: albumin, coagulation factors (except von Willebrand factor), carrier proteins, hormonal and growth factors
- Bile production: bile acids, cholesterol, lecithin, phospholipids
- Nutrient regulation: glucose/glycogen storage, lipid and amino acid metabolism
- Drug/toxin metabolism: conjugation of bilirubin, drugs, and other lipophilic compounds for excretion
- Ammonia detoxification via the urea cycle (unique to the liver)
- Immune defense via Kupffer cells (resident macrophages)
Because symptoms of liver disease often lag behind disease progression, LFTs are used to detect injury early, before clinical signs appear.
2. Components of the LFT Panel
The standard LFT panel includes:
| Test | Category | Normal Range (Adults) |
|---|---|---|
| ALT (alanine aminotransferase) | Hepatocellular injury | < 40 IU/L |
| AST (aspartate aminotransferase) | Hepatocellular injury | < 40 IU/L |
| ALP (alkaline phosphatase) | Cholestatic/biliary | 30-120 IU/L |
| GGT (gamma-glutamyl transferase) | Cholestatic/biliary | < 50 IU/L |
| Total bilirubin | Metabolic/excretory | 0.2-1.2 mg/dL |
| Direct (conjugated) bilirubin | Metabolic/excretory | 0-0.2 mg/dL |
| Albumin | Synthetic function | 3.5-5.0 g/dL |
| PT/INR | Synthetic function | INR < 1.2 |
3. Bilirubin - The Metabolic Pathway
Bilirubin is the primary metabolite of heme. Understanding its metabolism is essential for interpreting LFTs.
Production
- ~250-350 mg of bilirubin is produced daily in healthy adults
- ~85% comes from breakdown of senescent red blood cells in splenic macrophages
- Heme is cleaved by heme oxygenase → biliverdin + CO + Fe²⁺
- Biliverdin reductase (NADPH-dependent) converts biliverdin → unconjugated bilirubin
- Unconjugated bilirubin is lipid-soluble, toxic, and binds tightly to albumin in plasma
Hepatic Uptake and Conjugation
- Bilirubin-albumin complex is transported to the liver via the portal circulation
- Bilirubin enters hepatocytes through sinusoidal membrane transporters
- Inside the hepatocyte, bilirubin is conjugated with glucuronic acid by UDP-glucuronosyltransferase (UGT1A1) → conjugated (direct) bilirubin (water-soluble)
- Conjugated bilirubin is secreted into bile canaliculi via MRP2 transporters
Excretion
- Conjugated bilirubin passes through the bile ducts into the small intestine
- Gut bacteria convert it to urobilinogen; most is excreted in feces as stercobilin (brown color of stool)
- A small portion of urobilinogen is reabsorbed (enterohepatic circulation) and excreted in urine as urobilinogen
Delta Bilirubin
- In prolonged cholestasis, conjugated bilirubin covalently binds to albumin → delta bilirubin
- This explains prolonged jaundice after relief of biliary obstruction, as delta bilirubin has a long half-life (similar to albumin, ~18 days)
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 365
4. Aminotransferases (ALT and AST) - Markers of Hepatocellular Injury
Where they live in the cell (key diagram)
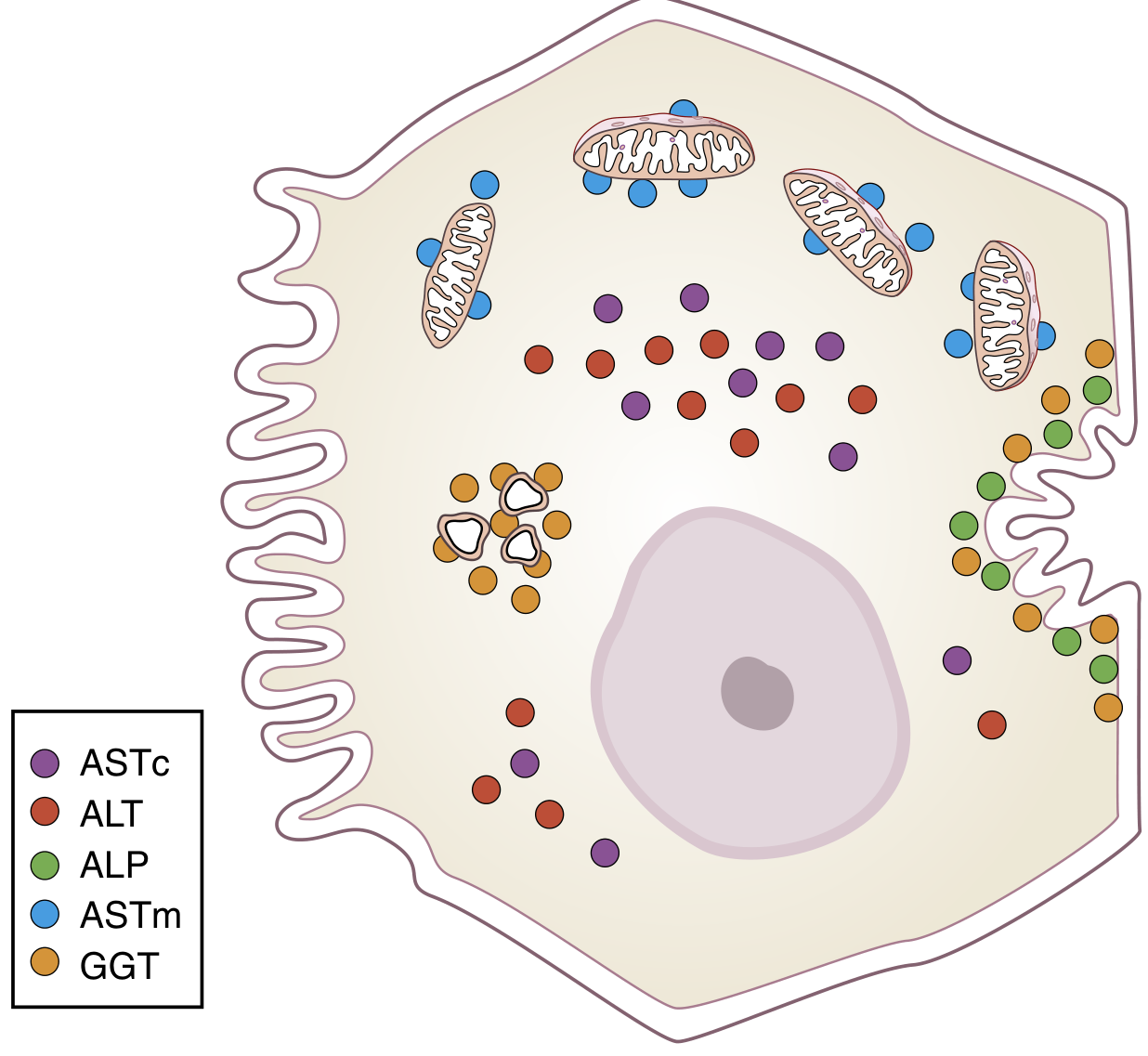
Figure: Location of hepatocellular enzymes. ALT and cytoplasmic AST (ASTc) are in the cytosol. Mitochondrial AST (ASTm) is in mitochondria. ALP and GGT are on the canalicular membrane. - Henry's Clinical Diagnosis and Management by Laboratory Methods
ALT (Alanine Aminotransferase / formerly SGPT)
- Catalyzes: Alanine + α-ketoglutarate → Pyruvate + Glutamate (requires vitamin B6/pyridoxal phosphate)
- Location: Entirely cytoplasmic - released only with membrane injury
- Tissue specificity: Highly liver-specific (much more than AST)
- Half-life: ~47 hours
- Elevated in: viral hepatitis, NAFLD/NASH, drug-induced liver injury, ischemic hepatitis
- Most sensitive marker of hepatocellular injury
AST (Aspartate Aminotransferase / formerly SGOT)
- Catalyzes: Aspartate + α-ketoglutarate → Oxaloacetate + Glutamate (also requires B6)
- Location: Both cytoplasmic and mitochondrial isoforms
- Found in: liver, heart muscle, skeletal muscle, kidney, brain - less liver-specific than ALT
- Half-life: cytoplasmic AST ~17 hours; mitochondrial AST ~87 hours
- Normal upper limit: ~40 IU/L for both
Clinical use of AST:ALT ratio
| Ratio | Interpretation |
|---|---|
| AST:ALT > 2:1 | Strongly suggests alcoholic liver disease (ethanol causes mitochondrial damage → mitochondrial AST release) |
| AST:ALT < 1 | Typical of viral hepatitis, NAFLD |
| AST:ALT > 1 with cirrhosis | Advanced fibrosis/cirrhosis (any cause) |
| Very high both (>1000 IU/L) | Ischemic hepatitis ("shock liver"), acute viral hepatitis, acute drug toxicity (e.g., acetaminophen) |
Important clinical pearl: In alcoholic patients who are vitamin B6-deficient, ALT and AST assays may give falsely low results because pyridoxal phosphate is required as a cofactor in the assay. Vitamin supplementation corrects this. (Henry's Clinical Diagnosis and Management by Laboratory Methods)
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 533
5. Alkaline Phosphatase (ALP) - Cholestatic Marker
- ALP is a canalicular membrane enzyme
- Mechanism of elevation in cholestasis: bile salt accumulation causes release of membrane fragments with attached canalicular enzymes into plasma
- Not liver-specific - also found in bone (osteoblasts), intestine, placenta, kidney
- To confirm hepatic origin, always check GGT - if GGT is also elevated, ALP is of hepatic origin
ALP Isoenzymes and Causes of Elevation
| Source | Clinical Context |
|---|---|
| Liver (hepatic ALP) | Cholestasis, biliary obstruction, infiltrative disease (sarcoidosis, lymphoma, metastases), primary biliary cholangitis |
| Bone | Paget's disease, fractures, bone metastases, hyperparathyroidism, growing children |
| Placenta | Normal pregnancy (2nd-3rd trimester) |
| Intestine | Blood groups B and O after fatty meal |
- Isolated ALP elevation (with normal GGT) usually points to a bone source
- ALP elevation with elevated bilirubin and GGT = cholestatic liver disease
6. GGT (Gamma-Glutamyl Transferase)
- Found in: bile duct epithelium, hepatocyte canalicular membrane, also in kidneys, pancreas
- Very sensitive but not specific - elevated by:
- Biliary obstruction / cholestasis
- Alcohol use (microsomal enzyme induction - even without liver damage)
- Enzyme-inducing drugs: phenytoin, phenobarbital, carbamazepine
- NAFLD
- Pancreatitis
- Primary clinical use: confirm that a raised ALP is of hepatic (not bone) origin
- GGT + ALP elevation = hepatobiliary cause confirmed
- Elevated GGT alone is a sensitive marker of alcohol use disorder
7. Albumin - Synthetic Function Marker
- Synthesized exclusively in the liver (~10-15 g/day)
- Half-life: ~18-20 days (long half-life makes it a marker of chronic rather than acute liver disease)
- Normal: 3.5-5.0 g/dL
- Low albumin (hypoalbuminaemia) in liver disease indicates:
- Reduced hepatic synthetic capacity
- Advanced/chronic liver disease (cirrhosis)
- Caveat: albumin is also lowered by protein malnutrition, nephrotic syndrome (urinary loss), protein-losing enteropathy, catabolism (infection, burns), and dilution (IV fluids)
- Not useful in acute liver failure (half-life too long to reflect acute changes)
8. Prothrombin Time (PT) / INR - Synthetic Function Marker
- The liver synthesizes all coagulation factors except von Willebrand factor (factors I, II, V, VII, VIII, IX, X, XI, XII, XIII)
- Factors II, VII, IX, X are vitamin K-dependent (require hepatic gamma-carboxylation)
- PT measures the extrinsic and common coagulation pathways
- PT/INR elevation in liver disease = reduced synthetic function
- Factor VII has the shortest half-life (~6 hours) → PT is the most sensitive and early synthetic function marker
- Acute liver failure causes rapid PT prolongation (within hours)
- PT elevation in liver disease must be distinguished from vitamin K deficiency (given IM vitamin K and recheck in 24h - if PT corrects, vitamin K deficiency; if it doesn't correct, liver synthetic failure)
9. Additional Tests Sometimes Included
| Test | What It Measures |
|---|---|
| Ammonia | Urea cycle function - elevated in hepatic encephalopathy; metabolized only by the liver |
| LDH (lactate dehydrogenase) | Hepatocellular necrosis; isoenzyme 5 specific to liver; non-specific |
| 5'-Nucleotidase | Biliary marker - confirms hepatic origin of raised ALP |
| Pseudocholinesterase | Falls in hepatocellular disease (parallel to albumin synthesis); useful in cirrhosis assessment |
| AFP (alpha-fetoprotein) | Tumor marker for hepatocellular carcinoma (HCC) |
| DCP (des-gamma-carboxyprothrombin) | Tumor marker for HCC; sensitivity 67%, specificity 92% |
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 366
10. Patterns of LFT Abnormality - Interpreting the Panel
This is the most clinically important concept. The pattern of abnormality, not any single test, guides diagnosis.
Pattern 1: Hepatocellular Pattern
- Predominant elevation: ALT and AST (often >5x-10x upper limit of normal)
- Bilirubin elevated (mixed or indirect predominance)
- ALP relatively normal or mildly elevated
- Causes: viral hepatitis (A, B, C, D, E), ischemic hepatitis ("shock liver"), drug toxicity (acetaminophen, isoniazid), autoimmune hepatitis, Wilson disease, acute fatty liver
- Massive elevation of ALT/AST (>1000 IU/L) = ischemic hepatitis, acute viral hepatitis, acute drug/toxin injury
Pattern 2: Cholestatic Pattern
- Predominant elevation: ALP and GGT (often >3-4x upper limit of normal)
- Bilirubin elevated (direct/conjugated predominant)
- ALT/AST normal or mildly elevated
- Causes: biliary obstruction (gallstones, cholangiocarcinoma, pancreatic cancer), primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), intrahepatic cholestasis of pregnancy, drug-induced cholestasis (methyltestosterone, anabolic steroids), sepsis
Pattern 3: Mixed Pattern
- Elevations of both aminotransferases and biliary enzymes
- Causes: drug-induced liver injury (sulfonamides, phenytoin), cholestatic viral hepatitis, overlap syndromes
Pattern 4: Isolated Hyperbilirubinemia
- Unconjugated (indirect) hyperbilirubinemia with normal enzymes: hemolysis, Gilbert syndrome (UGT1A1 polymorphism - benign), Crigler-Najjar syndrome
- Conjugated (direct) hyperbilirubinemia with normal enzymes: Dubin-Johnson syndrome, Rotor syndrome
- Jaundice is clinically detectable when serum bilirubin > 2.5 mg/dL (43 μmol/L)
Pattern 5: Synthetic Dysfunction Pattern
- Low albumin + prolonged PT + elevated bilirubin (hepatic decompensation)
- Normal or mildly elevated enzymes (burned-out cirrhosis)
- Causes: end-stage cirrhosis, acute liver failure, fulminant hepatic failure
- Tietz Textbook of Laboratory Medicine, 7th Edition
- Harrison's Principles of Internal Medicine 22nd ed.
11. Specific Disease Patterns
| Disease | ALT | AST | ALP | GGT | Bilirubin | Albumin | PT |
|---|---|---|---|---|---|---|---|
| Viral hepatitis (acute) | ↑↑↑ | ↑↑↑ | N or ↑ | ↑ | ↑ (mixed) | N | N or ↑ |
| Alcoholic hepatitis | ↑ | ↑↑ (>2:1) | ↑↑ | ↑↑↑ | ↑ | ↓ | ↑↑ |
| Biliary obstruction | N or ↑ | N or ↑ | ↑↑↑ | ↑↑↑ | ↑↑ (direct) | N | N |
| Cirrhosis (compensated) | ↑ | ↑ | ↑ | ↑ | N or ↑ | ↓ | ↑ |
| Ischemic hepatitis | ↑↑↑ | ↑↑↑ | N | N or ↑ | ↑ | N | N or ↑ |
| NAFLD/NASH | ↑ | ↑ | N or ↑ | ↑ | N | N | N |
| PBC | N or ↑ | N or ↑ | ↑↑↑ | ↑↑ | ↑ (direct) | ↓ (late) | ↑ (late) |
12. Causes of Liver Disease (from Harrison's)
The full classification of liver diseases includes:
- Inherited hyperbilirubinemia: Gilbert, Crigler-Najjar, Dubin-Johnson, Rotor syndrome
- Viral hepatitis: A, B, C, D, E; EBV, CMV, HSV
- Immune/autoimmune: Primary biliary cholangitis, autoimmune hepatitis, PSC
- Genetic: Wilson disease, hemochromatosis, alpha-1 antitrypsin deficiency, Gaucher's disease
- Alcohol: Acute fatty liver, alcoholic hepatitis, Laennec's cirrhosis
- Non-alcoholic fatty liver disease (NAFLD/NASH)
- Drug-induced: Hepatocellular (isoniazid, acetaminophen), cholestatic (methyltestosterone), mixed (sulfonamides, phenytoin)
- Cholestatic: Gallstones, extrahepatic obstruction, biliary atresia
- Vascular: Budd-Chiari syndrome, sinusoidal obstruction syndrome, ischemic hepatitis
- Systemic disease: Sarcoidosis, amyloidosis, celiac disease, glycogen storage diseases
- Mass lesions: HCC, metastases
- Harrison's Principles of Internal Medicine 22nd ed., Table 347-1
13. Key Clinical Pearls
- ALT is more liver-specific than AST; an elevated AST could be from heart or skeletal muscle
- AST:ALT > 2:1 + elevated GGT + elevated ALP = alcoholic liver disease until proven otherwise
- Isolated elevated GGT in an otherwise normal panel = alcohol use or enzyme-inducing drug (phenytoin, phenobarbital)
- ALP elevated in isolation (GGT normal) = likely bone disease or normal pregnancy
- Low albumin + prolonged PT = significant hepatic synthetic failure; marker of prognosis
- Delta bilirubin explains why jaundice persists even after biliary obstruction is relieved
- >80% of liver must be destroyed before liver function is abolished due to massive regenerative capacity
- Vitamin B6 deficiency (common in alcoholics) can cause falsely low ALT and AST - always consider
- A single reading of any enzyme is less useful than serial measurements showing a trend (rising vs. falling)
- Liver biopsy remains the gold standard for staging fibrosis, but carries risks: serious morbidity 0.6%, mortality 0.01%; sampling error in up to 20% of biopsies
14. Noninvasive Markers of Fibrosis
Because liver biopsy is invasive, several blood-based biomarker panels have been developed:
- FIB-4 score (age × AST / platelet count × √ALT) - widely used
- APRI (AST to Platelet Ratio Index)
- FibroTest / FibroSure - commercial panel
- Transient elastography (FibroScan) - measures liver stiffness
These supplement but do not fully replace liver biopsy because they do not give morphological information.
- Tietz Textbook of Laboratory Medicine, 7th Edition, p. 2022
Summary in one sentence: LFTs are a panel of serum tests that together distinguish hepatocellular injury (high ALT/AST), cholestatic disease (high ALP/GGT/direct bilirubin), and hepatic synthetic failure (low albumin, prolonged PT) - and the pattern, not any single test, is what guides clinical diagnosis.
Complete it
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have all the content needed. Here is the complete continuation of the LFT guide:
Liver Function Tests - Completion
15. Diagnostic Algorithm for Abnormal LFTs
This is the systematic, step-by-step approach every clinician uses when faced with an abnormal LFT result.
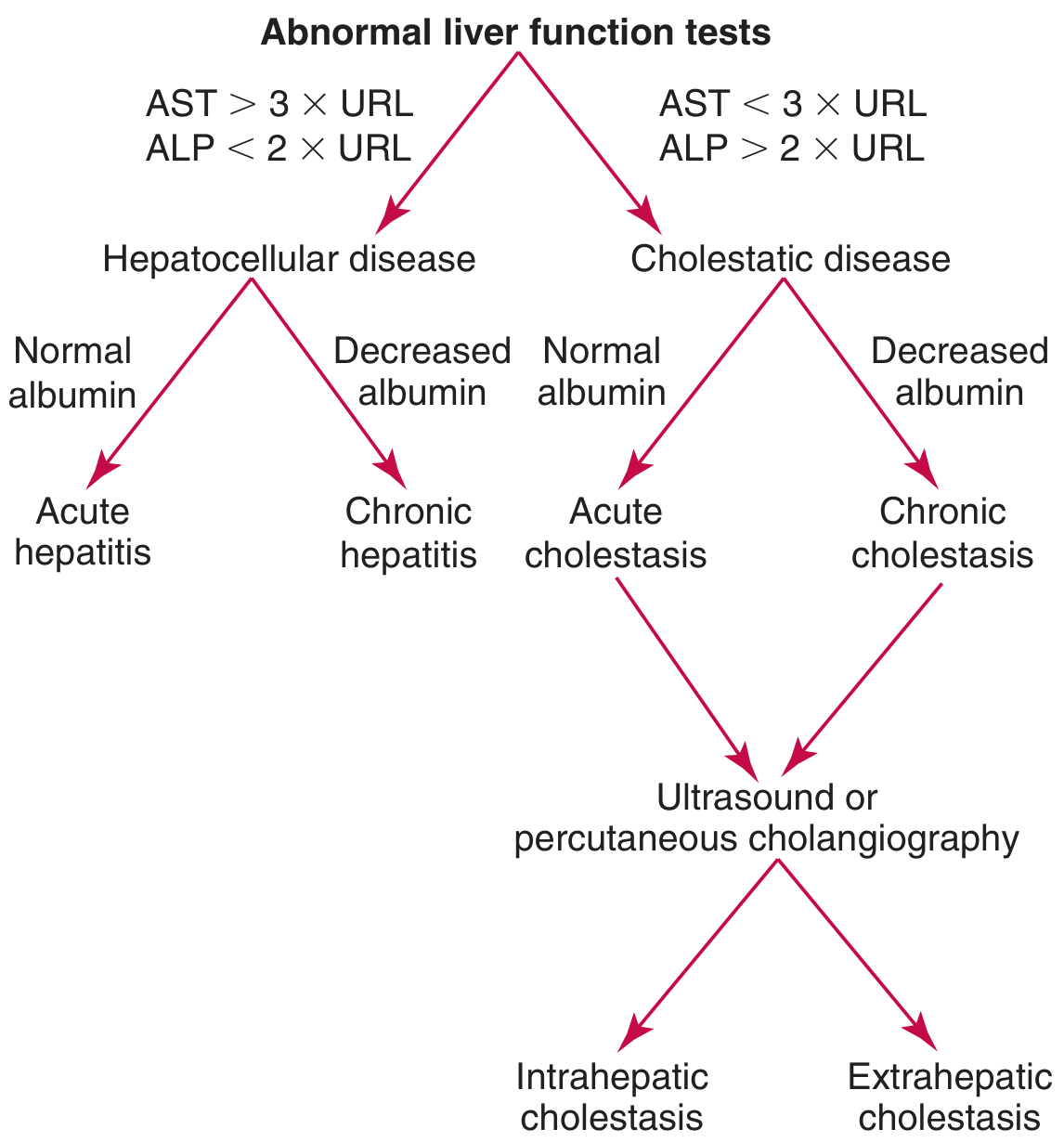
Figure: Algorithm for using abnormal LFTs to classify and diagnose liver disease. Start with the AST and ALP levels, determine the pattern (hepatocellular vs cholestatic), then use albumin to distinguish acute from chronic, and imaging to separate intra- from extrahepatic cholestasis. - Tietz Textbook of Laboratory Medicine, 7th Ed.
Step-by-Step Approach
Step 1: Identify the dominant pattern
- AST > 3× URL AND ALP < 2× URL → Hepatocellular pattern
- AST < 3× URL AND ALP > 2× URL → Cholestatic pattern
- Both elevated → Mixed pattern (assume cholestatic and rule out biliary obstruction first)
Step 2: Add albumin to gauge acuity
- Hepatocellular + normal albumin → Acute hepatitis
- Hepatocellular + low albumin → Chronic hepatitis (albumin takes weeks to fall)
- Cholestatic + normal albumin → Acute cholestasis
- Cholestatic + low albumin → Chronic cholestasis
Step 3: For cholestatic pattern - do ultrasound
- Dilated bile ducts → Extrahepatic (mechanical) obstruction - stone, stricture, malignancy
- Normal bile ducts → Intrahepatic cholestasis - drug, PBC, PSC, intrahepatic causes
Step 4: Severity and chronicity
- Check PT/INR: prolonged = synthetic failure (poor prognosis marker)
- Check bilirubin trend: higher bilirubin correlates with poorer prognosis in most chronic liver diseases
- Check albumin trend: falling albumin = progressive synthetic failure
Step 5: Etiology work-up (based on pattern and clinical context)
| Pattern | First-Line Tests |
|---|---|
| Acute hepatocellular | Hepatitis A IgM, HBsAg, anti-HBc IgM, anti-HCV, drug history |
| Chronic hepatocellular | HBsAg, anti-HCV, ANA/ASMA (autoimmune hepatitis), serum ferritin + transferrin saturation (hemochromatosis), ceruloplasmin (Wilson's in young), alpha-1 antitrypsin |
| Cholestatic | Ultrasound, AMA (primary biliary cholangitis), MRCP/ERCP for duct anatomy |
| Isolated ALP rise | GGT to confirm hepatic origin; bone-specific ALP or X-ray if GGT normal |
- Tietz Textbook of Laboratory Medicine, 7th Edition, p. 2020
16. Non-Hepatic Causes of Abnormal LFTs
A critical concept: abnormal LFT results occur in up to one-third of those screened, and only 1% indicate clinically significant liver disease. Many abnormalities are from non-hepatic sources.
| LFT | Non-Hepatic Cause |
|---|---|
| Low albumin | Protein-losing enteropathy, malnutrition, nephrotic syndrome, burns, sepsis, dilution |
| Elevated ALP | Bone disease (Paget's, fractures, metastases), pregnancy (placental isoenzyme), growing children, renal disease |
| Elevated AST | Acute myocardial infarction (cardiac AST), rhabdomyolysis (skeletal muscle), hypothyroidism, vigorous exercise |
| Elevated ALT | Skeletal muscle disease (but ALT is largely liver-specific compared to AST) |
| Elevated bilirubin | Hemolysis, ineffective erythropoiesis, sepsis, resorption of large hematoma, neonatal physiological jaundice |
| Prolonged PT | Vitamin K deficiency (poor diet, fat malabsorption, antibiotic suppression of gut flora, cholestasis), warfarin therapy, DIC |
| Elevated GGT | Alcohol (even without liver damage), enzyme-inducing drugs (phenytoin, phenobarbital, carbamazepine), pancreatitis |
Key differentiating test: If PT is prolonged and you're unsure whether it's due to vitamin K deficiency or hepatic synthetic failure - give parenteral vitamin K. If PT normalizes within 24-48 hours, the cause was vitamin K deficiency. If PT remains prolonged, it indicates hepatocyte dysfunction.
- Tintinalli's Emergency Medicine, p. 559
17. Inherited Hyperbilirubinaemia Syndromes
These are isolated hyperbilirubinaemia disorders with no structural liver disease - all other LFTs are normal.
Unconjugated (Indirect) Hyperbilirubinaemia
| Syndrome | Defect | Bilirubin Level | Features |
|---|---|---|---|
| Gilbert syndrome | UGT1A1 activity 10-33% of normal (UGT1A1*28 promoter polymorphism - A(TA)7TAA) | 1.5-4 mg/dL | Most common; benign; worsens with fasting, illness, exercise; autosomal recessive |
| Crigler-Najjar type 1 | UGT1A1 absent (< trace activity); ~59 different mutations | 18-45 mg/dL | Neonatal unconjugated jaundice; kernicterus and death without phototherapy; liver transplant required |
| Crigler-Najjar type 2 | UGT1A1 up to 10% activity | 6-25 mg/dL | Responds to phenobarbital (reduces to 3-5 mg/dL); generally benign |
Conjugated (Direct) Hyperbilirubinaemia
| Syndrome | Defect | Feature |
|---|---|---|
| Dubin-Johnson syndrome | Defect in canalicular MRP2 transporter (ABCC2 gene) | Liver appears black/dark (melanin-like pigment); benign; coproporphyrin ratio reversed |
| Rotor syndrome | Defects in SLCO1B1 and SLCO1B3 (sinusoidal uptake transporters) | No dark pigment; coproporphyrin total elevated; benign |
- Goldman-Cecil Medicine, p. 1552-1557
18. Hereditary Cholestatic Syndromes
Progressive Familial Intrahepatic Cholestasis (PFIC) - genetic defects in bile transport:
| Type | Gene | Protein Defect | Features |
|---|---|---|---|
| PFIC-1 | ATP8B1 | Phosphatidylserine flippase | Cholestasis, diarrhea, stunted growth, pruritus |
| PFIC-2 | ABCB11 | Canalicular bile salt translocase | Canalicular cholestasis; high risk of HCC |
| PFIC-3 | ABCB4 | Phosphatidylcholine flippase | Cholestasis; bile duct injury |
| PFIC-4 | TJP2 | Tight junction protein | Cholestasis; progressive early childhood |
| PFIC-5 | NR1H4 | Nuclear bile acid receptor FXR | Neonatal cholestasis; severe vitamin K-independent coagulopathy |
Treatment of cholestatic pruritus:
- Odevixibat (apical bile salt transporter blocker) - for PFIC patients ≥3 months
- Maralixibat - for Alagille syndrome cholestasis ≥1 year
- Partial biliary external diversion as surgical option
- Goldman-Cecil Medicine, p. 1557
19. Prognostic Scoring Systems Using LFT Components
Child-Pugh Score (Child-Turcotte-Pugh / CTP)
Used to grade severity of cirrhosis. Each component scored 1-3:
| Component | Score 1 | Score 2 | Score 3 |
|---|---|---|---|
| Bilirubin | ≤2 mg/dL | 2-3 mg/dL | ≥3 mg/dL |
| INR | ≤1.6 | 1.7-2.2 | ≥2.3 |
| Albumin | ≥3.5 g/dL | 2.8-3.5 g/dL | ≤2.7 g/dL |
| Ascites | None | Slight | Moderate |
| Hepatic encephalopathy | None | Grade 1-2 | Grade 3-4 |
Class A = 5-6 points (compensated cirrhosis - surgery possible)
Class B = 7-9 points (decompensated - elective surgery avoided)
Class C = 10-15 points (decompensated - surgery contraindicated, transplant listing)
Child-Pugh ≥7 (class B) = criterion for liver transplantation listing.
MELD Score (Model for End-Stage Liver Disease)
Uses 3 objective LFT-based variables:
MELD = 3.78 × ln[bilirubin mg/dL] + 11.2 × ln[INR] + 9.57 × ln[creatinine mg/dL] + 6.43
- Range: 6 (less ill) to 40 (gravely ill)
- Best predictor of short-term (3-month) mortality in cirrhosis
- Used for organ allocation for liver transplantation in the US
- MELD-Na adds sodium concentration (hyponatraemia worsens prognosis)
- MELD < 16 = lower postoperative mortality; MELD > 16 = substantially higher surgical risk
- PELD (Pediatric MELD) used for children under 12
Advantage of MELD over Child-Pugh: more objective (no subjective assessment of ascites severity or encephalopathy grade), wider range of values, better discrimination.
- Harrison's Principles of Internal Medicine 22nd ed., p. 2675
- Sabiston Textbook of Surgery
20. Ammonia and Hepatic Encephalopathy
- Ammonia is a byproduct of amino acid metabolism and is detoxified exclusively by the liver via the urea (Krebs-Henseleit) cycle
- In liver failure or portosystemic shunting: ammonia accumulates → hepatic encephalopathy (HE)
- Serum ammonia is used to confirm a diagnosis of HE - but it does not reliably correlate with encephalopathy grade (brain sensitivity to ammonia varies)
- Best measured on a rapidly processed iced arterial blood sample (ammonia is unstable ex-vivo)
- Elevated ammonia also from: intestinal bacterial overgrowth, GI bleeding (blood in gut → ammonia source), metabolic alkalosis, hypokalemia (renal ammonia production), rare urea cycle enzyme deficiencies
- Management: lactulose (traps ammonia in colon), rifaximin (reduces gut bacteria ammonia production), protein restriction (no longer recommended routinely)
Complications of decompensated cirrhosis tracked by LFTs:
- Hepatic encephalopathy: 20-40% cumulative 1-year survival; 15% at 3 years
- Ascites: 2-year median survival (non-malignant); 4-month survival (malignant)
- Hepatorenal syndrome type 1: median survival 2 weeks; type 2: 4-6 months
- Goldman-Cecil Medicine, p. 1560
21. LFTs in Specific Clinical Contexts
In Acute Liver Failure (ALF)
- Daily monitoring required
- PT/INR is the most sensitive early marker (factor VII - 6h half-life)
- Rising bilirubin + falling ALT/AST in the context of clinical deterioration = liver necrosis (enzymes are "used up" - a paradox called the "enzyme burnout" sign)
- ALF criteria: acute onset, encephalopathy, PT > 15-20 sec (or INR > 1.5) in a patient without pre-existing liver disease
In Alcoholic Liver Disease
- AST:ALT ratio > 2:1 (classically > 2) - key diagnostic clue
- GGT markedly elevated
- AST rarely > 300 IU/L in pure alcoholic hepatitis (values > 1000 IU/L suggest another cause like acetaminophen toxicity added to alcohol injury)
- Low AST/ALT despite severe alcoholic hepatitis can occur with pyridoxine (B6) deficiency
In NAFLD/NASH
- ALT typically > AST (early disease)
- When AST > ALT in NAFLD → suggests progression to cirrhosis
- GGT elevated (correlates with metabolic syndrome)
- GGT is an independent prognostic indicator of cardiovascular and all-cause mortality
In Drug-Induced Liver Injury (DILI)
- Hepatocellular pattern: isoniazid, acetaminophen, statins, antivirals
- Cholestatic pattern: methyltestosterone, anabolic steroids, amoxicillin-clavulanate, chlorpromazine
- Mixed pattern: sulfonamides, phenytoin
- Roussel Uclaf Causality Assessment Method (RUCAM) is used to score probability of DILI
In Cardiac Disease ("Cardiac Hepatopathy")
- Right heart failure → hepatic congestion → elevated ALP + mild elevation of aminotransferases + elevated bilirubin
- Acute right heart failure or shock → "ischemic hepatitis" or "shock liver": massive rise in AST/ALT (often > 1000-10,000 IU/L), resembles acute viral hepatitis
- AST often rises faster than ALT in ischemic hepatitis (cardiac AST contributing)
In Pregnancy
- Physiological: ALP elevated (placental isoenzyme) from 2nd trimester - normal finding
- Albumin mildly falls (dilutional)
- Abnormal: intrahepatic cholestasis of pregnancy (raised bile acids + ALP + GGT + bilirubin + pruritus), HELLP syndrome (Haemolysis + Elevated Liver enzymes + Low Platelets), acute fatty liver of pregnancy
22. Urine Tests Related to LFTs
Urine tests are sometimes used as bedside screening tools:
| Urine Test | Significance |
|---|---|
| Urine bilirubin (dipstick) | Only conjugated (direct) bilirubin appears in urine; positive = conjugated hyperbilirubinaemia (hepatocellular or obstructive jaundice). Absent in pure haemolysis (only indirect bilirubin) |
| Urine urobilinogen | Elevated in hepatocellular disease and haemolysis; absent in complete biliary obstruction (no bilirubin reaching gut) |
| Dark urine + pale stools | Classic sign of obstructive jaundice (conjugated bilirubin in urine, no stercobilin in stool) |
Note: Urine bilirubin/urobilinogen dipstick tests have sensitivity of only 70-74% for elevated serum bilirubin and are not recommended as standalone screening tests for liver disease.
- Tintinalli's Emergency Medicine, p. 559
23. Imaging Investigations After Abnormal LFTs
After LFTs, imaging is the next step for cholestatic patterns or suspected structural disease:
| Modality | Primary Use | Notes |
|---|---|---|
| Ultrasound (US) | First-line for suspected biliary obstruction | Cheap, no radiation, identifies dilated ducts, gallstones, liver lesions, portal hypertension |
| CT abdomen | Mass lesions, staging, vascular anatomy | Radiation; excellent for large lesions; low sensitivity for mild steatosis |
| MRCP | Non-invasive biliary tree imaging | Best for bile duct anatomy; no radiation; superior to CT for duct stones |
| ERCP | Diagnostic + therapeutic biliary intervention | Invasive; used when intervention (stent, stone removal) needed |
| MRI/MRS | Fat quantification, hepatic iron, fibrosis | MRI-PDFF is test of choice for quantitative liver fat; MR elastography for fibrosis |
| Transient elastography (FibroScan) | Liver stiffness = indirect fibrosis assessment | Non-invasive; can eliminate need for biopsy in many cases |
| Liver biopsy | Histological diagnosis, staging fibrosis | Gold standard but invasive; 15-20mm specimen with ≥10 portal tracts needed; mortality 0.01% |
24. Summary Table: Complete LFT Reference
| Test | What It Measures | Key Elevations | Key Reductions |
|---|---|---|---|
| ALT | Hepatocellular integrity | Viral hepatitis, NAFLD, drug toxicity, ischemic hepatitis | Vitamin B6 deficiency (false low) |
| AST | Hepatocellular + mitochondrial injury | Alcoholic hepatitis (>2:1 ratio), MI, rhabdomyolysis, viral hepatitis | Vitamin B6 deficiency (false low) |
| ALP | Biliary/canalicular integrity; bone | Cholestasis, biliary obstruction, PBC, bone disease, pregnancy | - |
| GGT | Biliary induction; microsomal activity | Alcohol, enzyme-inducing drugs, cholestasis, NAFLD | - |
| Total bilirubin | Bilirubin production vs clearance | Haemolysis (indirect), hepatitis, obstruction (direct) | - |
| Direct bilirubin | Conjugation and excretion | Cholestasis, hepatocellular disease | - |
| Albumin | Chronic hepatic synthesis | - | Cirrhosis, malnutrition, nephrotic syndrome, protein-losing enteropathy |
| PT/INR | Acute hepatic synthesis (factor VII most sensitive) | Liver failure, vitamin K deficiency, warfarin | - |
| Ammonia | Urea cycle function | Hepatic encephalopathy, portosystemic shunting, GI bleeding | - |
| AFP | Hepatocellular carcinoma surveillance | HCC, germ cell tumors | - |
25. One-Line Rules to Remember
- ALT > AST = viral hepatitis, NAFLD (liver-dominant injury)
- AST > ALT (> 2:1) = alcoholic hepatitis (mitochondrial injury + B6 deficiency)
- ALP + GGT both up = hepatobiliary cholestasis
- ALP up, GGT normal = bone or placental source
- GGT up alone = alcohol use or enzyme-inducing drug - not necessarily liver disease
- Low albumin + high INR + high bilirubin = decompensated liver failure
- Jaundice visible at bilirubin > 2.5 mg/dL (43 μmol/L)
- Dark urine + pale stools + itching = conjugated (obstructive) jaundice
- Isolated indirect hyperbilirubinaemia in young person = think Gilbert syndrome first
- Massive ALT/AST (>1000 IU/L) = ischemic hepatitis, acetaminophen toxicity, or acute viral hepatitis
- Normal LFTs do not exclude significant liver disease - cirrhosis can exist with a near-normal panel
- Trend matters more than any single value - rising or falling values predict trajectory
Sources: Harrison's Principles of Internal Medicine 22nd Ed., Henry's Clinical Diagnosis and Management by Laboratory Methods, Tietz Textbook of Laboratory Medicine 7th Ed., Goldman-Cecil Medicine, Tintinalli's Emergency Medicine, Sabiston Textbook of Surgery, Sleisenger and Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.