Pottasium of 6.5.how to correct
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
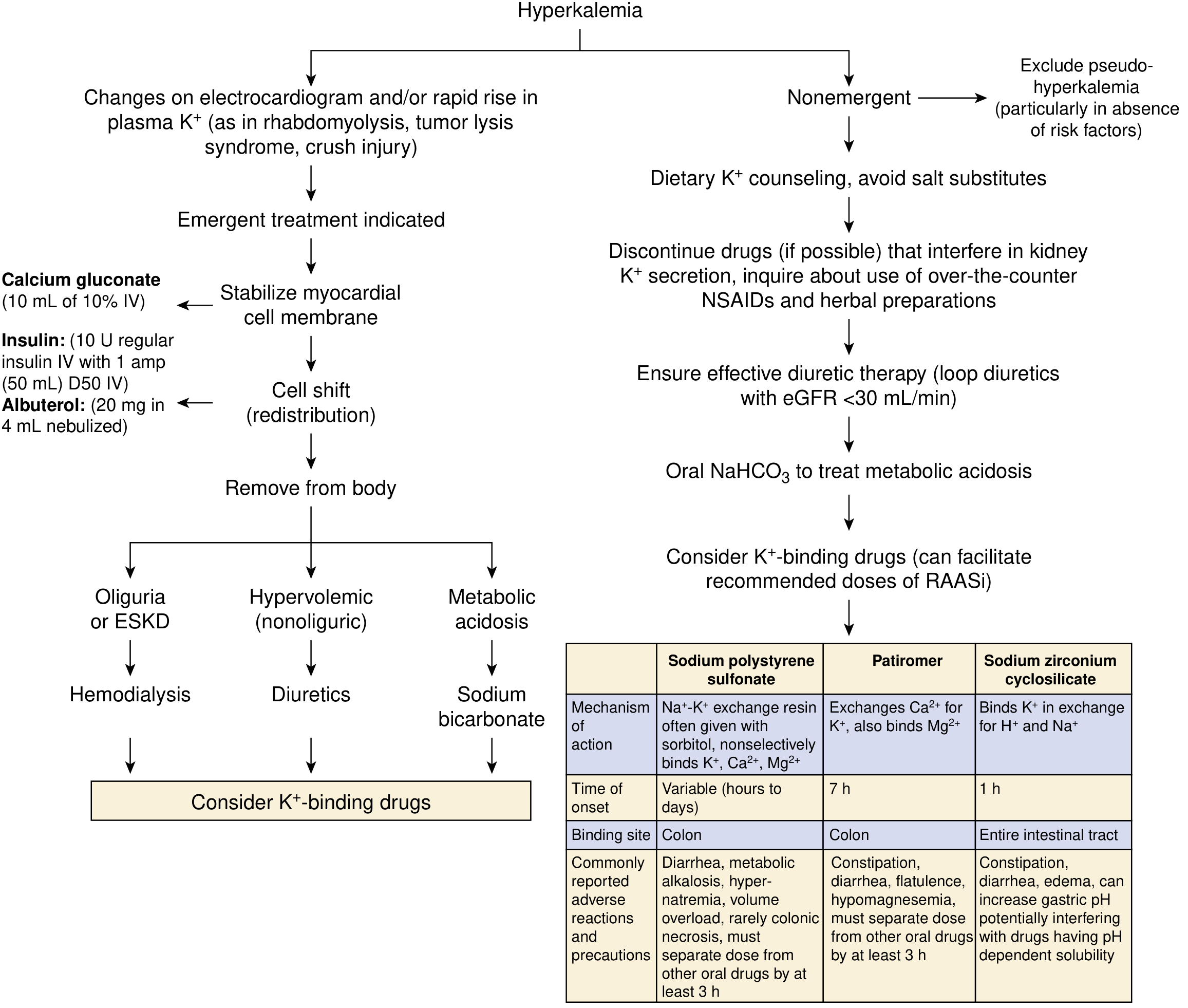
A potassium of 6.5 mEq/L is severe hyperkalemia requiring emergent management. Treatment follows three sequential goals:
Step 1 — Stabilize the Myocardium (Immediate)
IV Calcium (does NOT lower K⁺, only protects the heart)
- Calcium gluconate 10%: 10 mL IV over 2–3 min with cardiac monitoring
- Calcium chloride 10%: 3–5 mL IV (higher elemental calcium, but causes skin necrosis if it extravasates — avoid peripheral lines)
- Onset: 1–3 min | Duration: 30–60 min
- Repeat if no ECG improvement within 3–5 min, or if changes recur
- ⚠️ Use with extreme caution in patients on digoxin (calcium potentiates digoxin toxicity — dilute in 100 mL D5W and infuse over 20–30 min)
Step 2 — Shift K⁺ into Cells (Rapid Redistribution)
A. Insulin + Glucose (fastest, most reliable)
- Regular insulin 10 units IV + D50W 50 mL (25 g glucose) bolus immediately after
- Follow with 10% dextrose infusion at 50–75 mL/h to prevent hypoglycemia
- Onset: 15–20 min | Peak: 30–60 min | Duration: 4–6 h
- If glucose >200–250 mg/dL, give insulin without glucose
- ⚠️ Never give dextrose alone — can paradoxically worsen hyperkalemia via osmotic effect
- Monitor glucose closely (hypoglycemia is a common complication, especially in renal failure)
B. Nebulized Albuterol (additive to insulin)
- 20 mg nebulized over 10 min (much higher dose than for asthma)
- Onset: ~30 min | Peak: ~90 min | Duration: 2–6 h
- ~20% of ESRD patients are resistant — do not use alone without insulin
- Side effects: tachycardia, hyperglycemia
C. Sodium Bicarbonate (limited role in acute setting)
- Not recommended for acute emergent treatment
- Useful only if severe metabolic acidosis (bicarbonate <10 mmol/L) is present
- May lower K⁺ slowly over 4–6 h with isotonic infusion (150 mEq NaHCO₃ in 1 L D5W)
Step 3 — Remove K⁺ from the Body
| Method | Indication | Notes |
|---|---|---|
| Loop diuretics (furosemide) | Adequate kidney function, fluid overload | Effective if urine output preserved |
| Sodium polystyrene sulfonate (Kayexalate) | Adjunct/transition | 50 g PO in sorbitol or enema; onset hours–days; risk of colonic necrosis |
| Patiromer | Chronic/adjunct management | 8.4 g once daily; onset ~7 h; avoid within 3 h of other meds |
| Sodium zirconium cyclosilicate | Chronic/adjunct | Onset ~1 h; higher K⁺ binding capacity than SPS |
| Hemodialysis | Oliguria, ESKD, AKI, refractory hyperkalemia | Most effective method; cannot be started fast enough to replace Steps 1–2 |
Treatment Algorithm
Quick Summary for K⁺ = 6.5
- Admit + continuous cardiac monitoring
- ECG immediately — if peaked T waves, sine wave, wide QRS → treat as emergency
- Calcium gluconate 10 mL of 10% IV → cardiac protection
- Insulin 10U + D50W → lower K⁺
- Albuterol 20 mg nebulized → additive K⁺ lowering
- Remove K⁺: diuretics if urine output present; dialysis if ESKD/AKI
- Identify and treat the cause (ACE inhibitors, ARBs, NSAIDs, adrenal insufficiency, AKI, CKD)
— Harrison's Principles of Internal Medicine 22E, p. 404 | NKF Primer on Kidney Diseases, 8e, pp. 128–129
This is a shared conversation. Sign in to Orris to start your own chat.