Hi so my team and i are presenting on Gatrointestinal bleeding for undergraduate year 3 surgical posting and i will be talking about anatomy upper and lower gastrointestinal tract, its going to be less than 5 minutesof presentation what i should cover, provide links of images i should use too
upper gastrointestinal tract anatomy diagram
lower gastrointestinal tract colon anatomy diagram
GI tract anatomy esophagus stomach duodenum small bowel colon labeled surgical
GI Bleeding — Anatomy Segment (Under 5 Minutes)
Slide Structure & What to Say
Slide 1 — The Anatomical Landmark: Ligament of Treitz (~45 sec)
- The ligament of Treitz (suspensory muscle of the duodenum) is the dividing line between upper and lower GI bleeding.
- Upper GI bleeding (UGIB): any source proximal to the ligament of Treitz — oesophagus → stomach → duodenum (1st–4th parts)
- Lower GI bleeding (LGIB): any source distal to it — jejunum, ileum, colon, rectum, anus
This distinction drives everything clinically — how the patient presents (haematemesis vs. rectal bleeding), how you investigate, and how you manage.
Slide 2 — Upper GI Tract: Key Anatomy (~1.5 min)
| Structure | Key Anatomical Points for GI Bleeding |
|---|---|
| Oesophagus | Lower 1/3 → portal hypertension → varices (submucosal venous plexus drains via azygos → portal) |
| Gastro-oesophageal junction | Mallory-Weiss tears occur at the mucosal junction here |
| Stomach | Rich blood supply: left/right gastric, left/right gastroepiploic, short gastric arteries. Peptic ulcer disease → posterior DU can erode gastroduodenal artery (GDA) |
| Duodenum | 1st part = bulb (most common PUD site). Posterior D1 is directly adjacent to the GDA — the most dangerous arterial bleeding source in UGIB |
Slide 3 — Lower GI Tract: Key Anatomy (~1.5 min)
| Structure | Key Anatomical Points for GI Bleeding |
|---|---|
| Small bowel (jejunum/ileum) | Long vasa recta from SMA; difficult endoscopic access — LGIB here is rare but serious |
| Colon | Two distinct arterial territories — critical for understanding bleeding patterns |
| Rectum | Dual supply: superior rectal (IMA) + middle/inferior rectal (internal iliac) |
| Anal canal | Internal haemorrhoids = dilated superior rectal venous plexus (above dentate line); external haemorrhoids = inferior rectal plexus |
- SMA territory: cecum, ascending colon, proximal 2/3 transverse colon — diverticulae most common here
- IMA territory: distal transverse, descending, sigmoid — angioectasia common here
- Watershed zones (Griffiths' point at splenic flexure, Sudeck's point at rectosigmoid) — most vulnerable to ischaemia
Slide 4 — Why Anatomy Matters Clinically (~1 min)
- Haematemesis → UGIB (proximal to Treitz)
- Melaena → usually UGIB (blood digested over ~8 hours), occasionally proximal LGIB
- Haematochezia → usually LGIB, but massive UGIB can also cause it
- Knowing the arterial supply tells you where to look on angiography/CT angiography and where to embolise
- Knowing venous drainage explains portal hypertension varices (portal → azygos at GOJ)
Images to Use in Your Slides
Image 1 — Lower GI Vascular Territories (use on Slide 3)
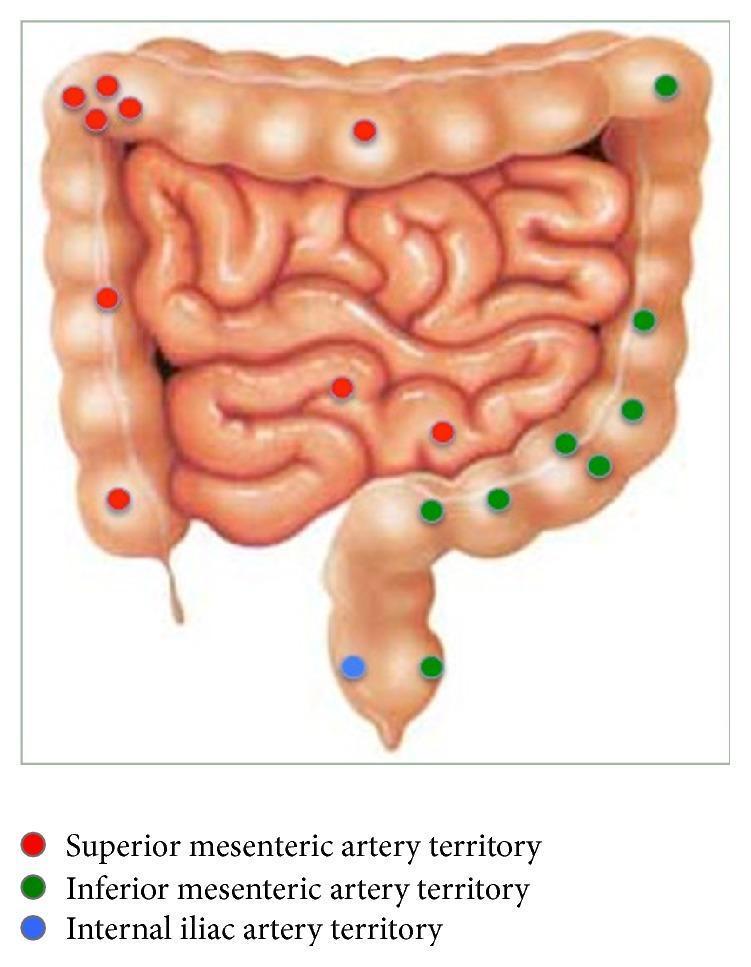
Image 2 — Upper GI Tract Schematic (use on Slide 2)
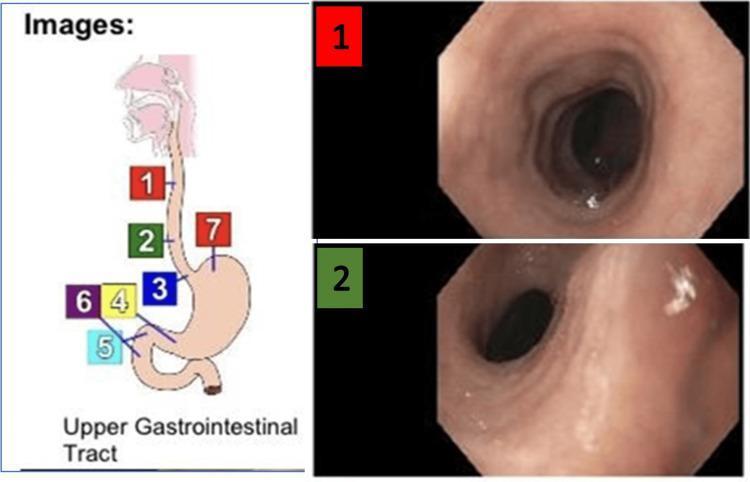
Image 3 — Suggested external resource
Timing Summary
| Section | Time |
|---|---|
| Ligament of Treitz — the dividing line | 45 sec |
| Upper GI anatomy + blood supply | 1.5 min |
| Lower GI anatomy + vascular territories | 1.5 min |
| Clinical correlation (why anatomy = presentation) | 1 min |
| Total | ~4 min 45 sec |
My friends are presenting on the pathophysiology of gi bleeding, how to avoid clashing if i havenslidenumber 4 or should i omit it
The Clash Risk
- Why varices bleed (portal hypertension → pressure → rupture)
- Why peptic ulcers bleed (mucosal breakdown → vessel erosion)
- The mechanism behind haematemesis vs. melaena vs. haematochezia
How to Reframe Slide 4 (Keep It, Change the Angle)
| Instead of saying... | Say this (anatomy framing)... |
|---|---|
| "Blood is digested over 8 hours causing melaena" | "Melaena indicates a source proximal to the splenic flexure — the transit distance is long enough for digestion" |
| "Portal hypertension causes varices" | "Varices occur at portosystemic anastomotic sites — GOJ, rectal plexus, umbilical veins — where portal and systemic circulations connect" |
| "Haematochezia means LGIB" | "Bright red blood per rectum localises the source to the distal colon or rectum — short transit, no digestion" |
Practical Tip
"I'll cover what the symptoms tell us about where the bleeding is anatomically — the why it bleeds is coming up in the next section."
Whats my overall script for slide 1 to 4
Full Presentation Script
Slide 1 — The Ligament of Treitz (~45 seconds)
"Good morning everyone. I'll be covering the anatomy of the gastrointestinal tract as it relates to GI bleeding.Before we talk about any specific structure, there is one anatomical landmark that underpins everything in GI bleeding — the ligament of Treitz, also called the suspensory muscle of the duodenum. It marks the junction between the fourth part of the duodenum and the jejunum.This single structure divides GI bleeding into two categories. Everything proximal to it — the oesophagus, stomach, and duodenum — is upper GI bleeding. Everything distal — the jejunum, ileum, colon, rectum, and anus — is lower GI bleeding.Keep that landmark in mind, because every structure I discuss from here sits on one side of that line."
Slide 2 — Upper GI Tract Anatomy (~1 min 30 seconds)
"Starting with the upper GI tract.The oesophagus is the first structure of note. Its lower third is where you find oesophageal varices — these develop in the submucosal venous plexus at the gastro-oesophageal junction, a site where the portal and systemic circulations meet. The gastro-oesophageal junction itself is also where Mallory-Weiss tears occur — linear mucosal splits at that junction.Moving into the stomach — it has an extraordinarily rich arterial supply from the coeliac axis: the left and right gastric arteries along the lesser curve, the left and right gastroepiploic arteries along the greater curve, and the short gastric arteries supplying the fundus. This is why gastric bleeding can be brisk and difficult to control.Finally the duodenum, specifically the first part or the bulb — this is the most common site for peptic ulcer disease. What makes it surgically important is the gastroduodenal artery, which runs directly posterior to the first part of the duodenum. A posterior duodenal ulcer that erodes into the GDA produces one of the most catastrophic bleeds we see — high volume, arterial, and potentially life-threatening."
Slide 3 — Lower GI Tract Anatomy (~1 min 30 seconds)
"Now the lower GI tract, distal to the ligament of Treitz.The small bowel — jejunum and ileum — is supplied by the superior mesenteric artery via long vasa recta. Bleeding here is uncommon but serious, and it's notoriously difficult to access endoscopically.The colon is where most lower GI bleeding originates, and its anatomy is best understood through two arterial territories — which you can see on this diagram.(point to image)The superior mesenteric artery supplies the small bowel, caecum, ascending colon, and proximal two-thirds of the transverse colon — shown in red. The inferior mesenteric artery supplies the distal transverse, descending, and sigmoid colon — shown in green. The rectum has a dual supply from the IMA above and the internal iliac arteries below — shown in blue.Two points on the colon worth highlighting: the splenic flexure and the rectosigmoid junction are watershed zones — where the terminal branches of two arterial systems meet. These areas are most vulnerable to ischaemia when blood pressure drops.Finally the anal canal — internal haemorrhoids arise from the superior rectal venous plexus above the dentate line. External haemorrhoids arise from the inferior rectal plexus below it. A simple anatomical line — the dentate line — separates them."
Slide 4 — Anatomy Maps the Bleeding Source (~1 minute)
"So to bring it all together — and I want to be clear this is purely the anatomical perspective, my colleagues will be explaining the mechanisms behind why these sites bleed.When a patient presents with haematemesis, you are dealing with a source proximal to the ligament of Treitz — the oesophagus, stomach, or duodenum.Melaena — dark, tarry stool — tells you the source is anatomically far enough proximal that blood undergoes digestion during transit. That typically means proximal to the splenic flexure.Bright red blood per rectum localises the source to the distal colon or rectum — short transit, no time for digestion.And knowing the arterial supply — coeliac axis for the upper tract, SMA and IMA for the lower — tells the surgical team where to look on CT angiography and where to target for embolisation.So the anatomy does not just describe the structures — it tells you where the patient is bleeding from before you even pick up a scope.I'll hand over now to my colleague who will cover the pathophysiology."
Timing Summary
| Slide | Content | Time |
|---|---|---|
| 1 | Ligament of Treitz | ~45 sec |
| 2 | Upper GI anatomy | ~1 min 30 sec |
| 3 | Lower GI anatomy | ~1 min 30 sec |
| 4 | Anatomy maps the source | ~1 min |
| Total | ~4 min 45 sec |
- Speak to the audience, not the slide — glance at the image to direct attention, then look back up
- The GDA line on Slide 2 is your "wow moment" — slow down there, surgeons love it
- Your last line is a clean handoff — it signals to the examiner that the team is coordinated and you know your scope
Give me examples of pictures to show for upper gi bleeding and lower gi bleeding for slide 2 and 3 so that i dont need to make slide 4 separately
upper gastrointestinal bleeding peptic ulcer haematemesis endoscopy
lower gastrointestinal bleeding diverticular haematochezia colonoscopy rectal bleeding
Images for Slide 2 & 3 (Replacing Slide 4)
Slide 2 — Upper GI Tract
Picture A: Anatomy diagram (already have this)
Picture B: Active duodenal ulcer bleeding (OGD view)
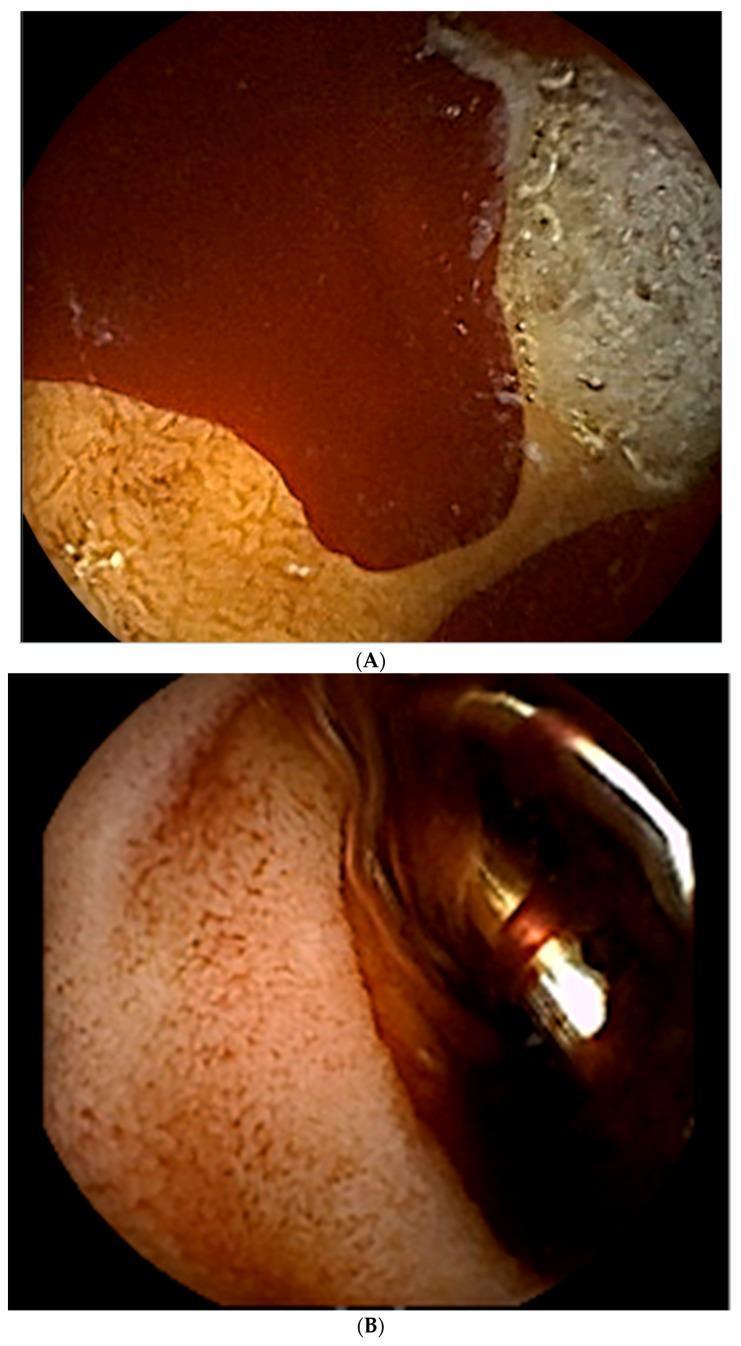
"This is what a posterior duodenal ulcer eroding the gastroduodenal artery looks like on OGD — the patient presented with haematemesis and melaena, both pointing us anatomically to a source proximal to the ligament of Treitz."
Slide 3 — Lower GI Tract
Picture A: Vascular territory diagram (already have this)
Picture B: Diverticular bleed on colonoscopy

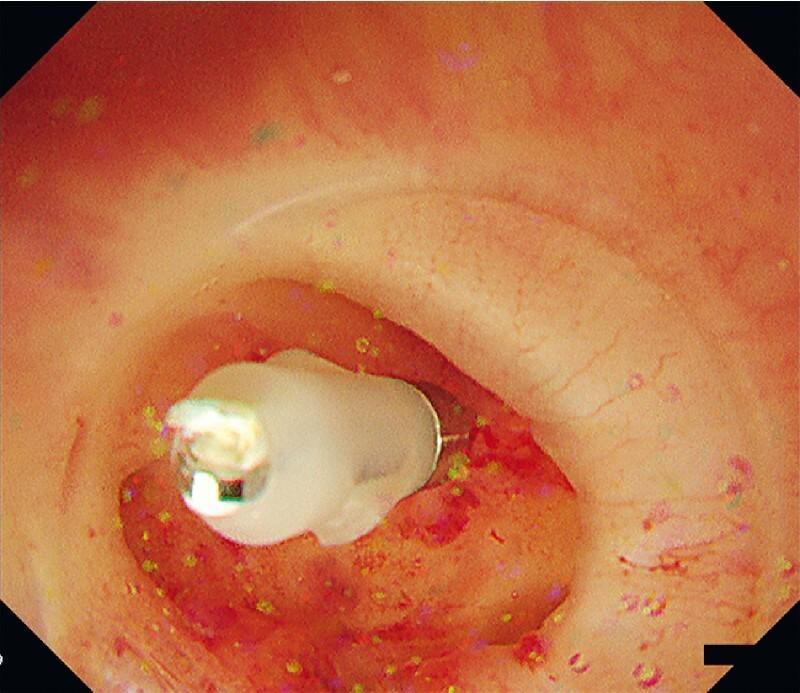
"This is diverticular bleeding on colonoscopy — the patient presented with bright red blood per rectum, haematochezia, which anatomically localises the source to the distal colon. The vascular territory diagram tells us which artery to target if this needs angioembolisation."
How to Layout Each Slide
SLIDE 2: SLIDE 3:
┌─────────────┬──────────────┐ ┌─────────────┬──────────────┐
│ Upper GI │ Duodenal │ │ Vascular │ Diverticular│
│ anatomy │ ulcer OGD │ │ territory │ bleed OGD │
│ schematic │ (bleeding) │ │ diagram │ (colonoscopy│
│ │ │ │ SMA/IMA) │ + clip) │
└─────────────┴──────────────┘ └─────────────┴──────────────┘
Caption: "Haematemesis/melaena Caption: "Haematochezia →
→ proximal to Treitz" distal to Treitz"
Should i add pictures of melena and hemotochizia or do u think it will be handled by the ones doing clinical features
Why You Should Not Include Them
The Distinction in One Line
| Image | Whose territory |
|---|---|
| Duodenal ulcer bleeding on OGD | Yours — anatomy of the bleeding source |
| Tarry black melaena stool | Clinical features team |
| Diverticular bleed on colonoscopy | Yours — anatomy of the bleeding source |
| Bright red blood per rectum | Clinical features team |
What You Can Do Instead
- You name the clinical sign just enough to connect anatomy to presentation
- You do not step into the clinical features section
- When the clinical features presenter shows their melaena photo, it reinforces your slide rather than repeating it — the audience sees the connection themselves
The pics u send could u label them on what is what in the pictures
Image 1 — Slide 2 (Upper GI)
Panel A (top):
| What you see | What it is |
|---|---|
| Dark red pooling fluid filling the lumen | Active blood — arterial haemorrhage |
| White/cream cratered area at the top | Duodenal ulcer base — fibrinous slough covering the ulcer crater |
| Orange-brown textured tissue at bottom | Normal duodenal mucosa (bulb) with villi pattern |
| Location | First part of duodenum — directly overlying the gastroduodenal artery posteriorly |
Panel B (bottom):
| What you see | What it is |
|---|---|
| Smooth pink/brown tissue | Post-treatment duodenal mucosa — bleeding controlled |
| Shiny metallic object (right side) | Haemostatic clip — deployed to mechanically compress the bleeding vessel |
| Dark tunnel in centre | Duodenal lumen — scope looking forward |
Image 2 — Slide 3 (Lower GI) — Vascular Territory Map
| What you see | What it is |
|---|---|
| Large outer frame of bowel (haustra visible) | Large intestine / colon — caecum bottom right, ascending colon right side, transverse colon top, descending + sigmoid colon left side |
| Coiled loops in the centre | Small intestine — jejunum and ileum |
| Red dots | Superior mesenteric artery (SMA) territory — small bowel, caecum, ascending colon, proximal 2/3 transverse colon |
| Green dots | Inferior mesenteric artery (IMA) territory — distal transverse, descending, sigmoid colon |
| Single blue dot (bottom centre) | Internal iliac artery territory — rectum |
| Area between last red and first green dot (top of colon) | Splenic flexure watershed zone — most vulnerable to ischaemia |
Image 3 — Slide 3 (Lower GI) — Diverticular Bleed
| What you see | What it is |
|---|---|
| Pink/red surrounding tissue | Colonic mucosa — erythematous from recent haemorrhage and inflammation |
| Dark circular opening/outpouching in centre | Colonic diverticulum — herniation of mucosa through a weak point in the bowel wall, typically where the vasa recta penetrate |
| Small metallic device applied at the opening | Haemostatic clip — placed directly onto the bleeding vessel inside the diverticulum |
| Transparent rim around the scope tip | Endoscopic hood — used to stabilise the scope and open the diverticulum for better access |
| Red streaks on mucosa | Stigmata of recent bleeding — confirms this diverticulum is the source |
So ligament of triatz is until the end of duodenum right...
The Exact Location
Quick Duodenum Reminder
| Part | Location | Clinical relevance |
|---|---|---|
| 1st (bulb) | Pylorus → superior | Most common PUD site |
| 2nd (descending) | Curves downward | Ampulla of Vater opens here |
| 3rd (horizontal) | Crosses midline | Crosses over aorta and IVC |
| 4th (ascending) | Goes back up | Ends at ligament of Treitz |
The Simple Way to Remember It
Duodenum ends → Ligament of Treitz → Jejunum beginsEverything from the mouth to that point = Upper GI Everything from that point onwards = Lower GI
One Common Mistake to Avoid
Do u think i shud add those pics u sent right now or the ones i already put is enough because i dont wanna explain slide 4 separately, could u give me a rephrase script
Revised Script — 3 Slides Only
Slide 1 — The Ligament of Treitz (~45 seconds)
"Good morning everyone. I'll be covering the anatomy of the GI tract as it relates to GI bleeding.The single most important landmark is the ligament of Treitz — it attaches at the duodenojejunal flexure, marking the end of the fourth part of the duodenum and the start of the jejunum.This divides GI bleeding into two categories. Everything proximal — oesophagus, stomach, duodenum — is upper GI bleeding. Everything distal — jejunum, ileum, colon, rectum — is lower GI bleeding.That one line drives how the patient presents, how you investigate, and where you look for the source."
Slide 2 — Upper GI Tract (~1 min 45 seconds)
"Starting proximally with the upper GI tract.The lower oesophagus — specifically the submucosal venous plexus at the gastro-oesophageal junction — is where varices develop. The GOJ itself is also where Mallory-Weiss tears occur, linear mucosal splits from forceful vomiting.The stomach has a rich arterial supply from the coeliac axis — left and right gastric arteries along the lesser curve, gastroepiploic arteries along the greater curve, and short gastric arteries to the fundus. Bleeding here can be rapid and high volume.The most surgically critical point is the first part of the duodenum. The gastroduodenal artery runs directly posterior to it. A posterior duodenal ulcer that erodes into the GDA produces one of the most dangerous bleeds we see.(point to OGD image)This is exactly that — active arterial haemorrhage pooling in the duodenal bulb on OGD. Panel A shows the bleeding ulcer crater, Panel B shows a haemostatic clip deployed onto the vessel. This patient presented with haematemesis and melaena — both pointing anatomically to a source proximal to the ligament of Treitz."
Slide 3 — Lower GI Tract (~1 min 45 seconds)
"Distal to the ligament of Treitz — the lower GI tract.The colon is best understood through its two arterial territories, which you can see on this diagram.(point to vascular territory diagram)Red is the superior mesenteric artery territory — small bowel, caecum, ascending colon, and proximal two-thirds of the transverse colon. Green is the inferior mesenteric artery territory — distal transverse, descending, and sigmoid. Blue at the bottom is the internal iliac supplying the rectum.Where the SMA and IMA territories meet — at the splenic flexure — is a watershed zone, most vulnerable when perfusion drops.The anal canal is divided by the dentate line — internal haemorrhoids above it from the superior rectal venous plexus, external haemorrhoids below from the inferior rectal plexus.(point to colonoscopy image)This is a bleeding colonic diverticulum — the weak point where vasa recta penetrate the bowel wall. A clip has been placed onto the exposed vessel. This patient came in with haematochezia — bright red blood per rectum — which anatomically localises the source to the distal colon, short transit, no digestion.Knowing which arterial territory the bleeding sits in tells the surgical team exactly where to look on CT angiography and where to embolise.I'll hand over now to my colleague who will cover the pathophysiology."
Why This Works
- Slide 4 content is now one sentence each embedded at the end of Slides 2 and 3
- You name haematemesis, melaena, and haematochezia just enough to connect anatomy to presentation — without explaining mechanisms, which is your colleagues' job
- The handoff line at the end is clean and signals the team is coordinated
- Total time is comfortably under 5 minutes
Help me understand the whole upper and lowergastrointestinal tract as though im a donkey
The Whole Ride — From Top to Bottom
🎢 The Entrance — Mouth & Oesophagus
🏊 The Big Pool — Stomach
- A fundus (the roof of the pool — top part)
- A body (the main pool)
- An antrum (the shallow end where food collects before leaving)
- A pylorus — another bouncer at the exit, controlling how fast chyme enters the next section
🌀 The Twisty Narrow Slide — Duodenum
- Bile from the liver and gallbladder enters here (via the ampulla of Vater in the 2nd part)
- Pancreatic enzymes pour in here too
- Together they neutralise the acid from the stomach and start breaking down fats and proteins properly
🌿 The Long Winding Slide — Small Bowel (Jejunum & Ileum)
- First 2.5m = jejunum (thick walls, tall folds, absorbs most nutrients here)
- Last 3.5m = ileum (thinner walls, absorbs vitamin B12 and bile salts specifically, ends at the ileocaecal valve)
🏟️ The Wide Open Section — Large Bowel (Colon)
- Caecum (bottom right) — where the ileum empties in, appendix hangs off here
- Ascending colon — goes up the right side
- Transverse colon — crosses left to right across the top
- Descending colon — goes down the left side
- Sigmoid colon — the S-shaped bendy bit at the bottom left
- SMA handles the right side (caecum → proximal 2/3 transverse)
- IMA handles the left side (distal transverse → sigmoid)
🏁 The Exit — Rectum & Anal Canal
- Internal sphincter — smooth muscle, involuntary, you cannot control it
- External sphincter — skeletal muscle, voluntary, this is what you squeeze
- Above = internal haemorrhoids, visceral pain (you do not feel them as sharply)
- Below = external haemorrhoids, somatic pain (very painful, you feel everything)
The Two Halves Summary
| Upper GI | Lower GI | |
|---|---|---|
| Boundary | Mouth → end of duodenum | Jejunum → anus |
| Landmark | Ligament of Treitz | Ligament of Treitz |
| Blood supply | Coeliac axis | SMA + IMA + internal iliac |
| Main jobs | Receive, acidify, begin digestion | Absorb nutrients + water, compact waste, expel |
| Bleeding presents as | Haematemesis, melaena | Haematochezia |