Adrenal function test short note
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough short note. Here it is:
Adrenal Function Tests - Short Note
The adrenal gland has two functionally distinct parts: the cortex (producing glucocorticoids, mineralocorticoids, and androgens) and the medulla (producing catecholamines). Function tests are designed to confirm either hyperfunction or hypofunction of these zones.
I. Tests for Glucocorticoid (Cortisol) Function
A. Basal Cortisol Measurement
- Cortisol secretion shows diurnal variation: highest at 8 AM, lowest around midnight.
- Loss of this diurnal variation is one of the earliest signs of adrenal hyperfunction.
- Serum cortisol at 8 AM and midnight can be compared; a flat or elevated midnight level is abnormal.
- A random single measurement is generally inadequate due to pulsatile secretion.
B. Dexamethasone Suppression Test (DST)
Dexamethasone is a potent synthetic glucocorticoid that suppresses ACTH and cortisol via negative feedback in normal individuals.
1. Overnight (Low-Dose) DST - Screening Test for Cushing Syndrome
- Protocol: 1 mg dexamethasone orally at 11 PM; serum cortisol measured at 8-9 AM next morning.
- Normal response: Cortisol suppressed to < 1.8 µg/dL (50 nmol/L)
- Abnormal (positive): Failure to suppress = suggestive of Cushing syndrome.
- False positives: Oral contraceptive pills (OCP - estrogen increases cortisol-binding globulin; OCPs must be stopped 6 weeks before testing), acute illness, depression, alcoholism.
2. Two-Day Low-Dose DST (Confirmatory)
- 0.5 mg dexamethasone every 6 hours for 2 days.
- 24-hour urine free cortisol (UFC) is measured.
- UFC suppressed to < 50% of baseline rules out Cushing syndrome.
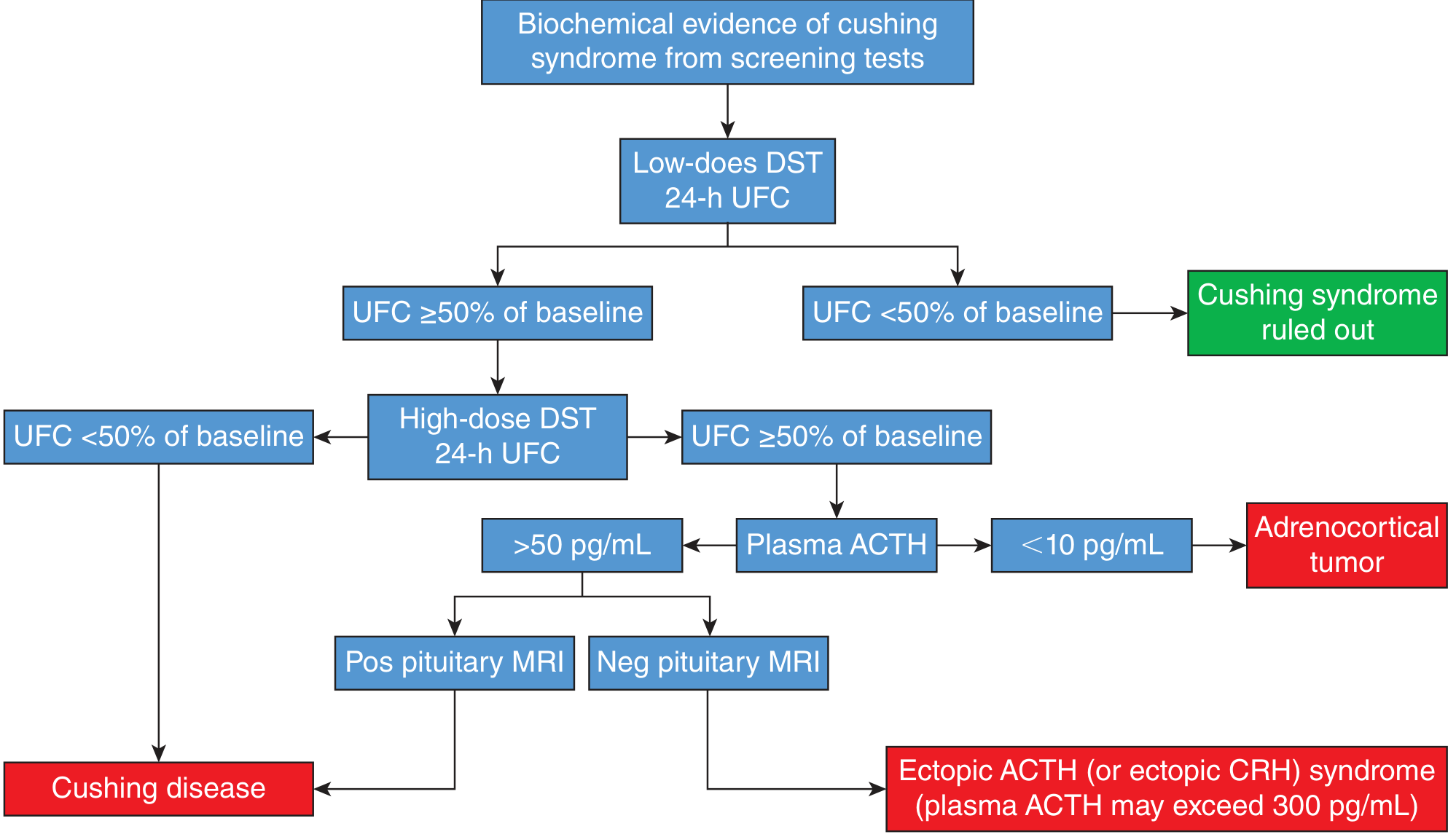
3. High-Dose DST (Differential Diagnosis)
- 2 mg dexamethasone every 6 hours for 2 days (total 8 mg) - or overnight 8 mg version.
- Interpretation:
- UFC suppressed to < 50% of baseline → Cushing disease (pituitary adenoma - ACTH still responds to high-dose suppression)
- UFC not suppressed + ACTH < 10 pg/mL → Adrenocortical tumor (ACTH-independent)
- UFC not suppressed + ACTH > 50 pg/mL → Ectopic ACTH syndrome (ACTH > 300 pg/mL in ectopic tumors - resistant to suppression)
Diagnostic algorithm for Cushing syndrome:
C. 24-Hour Urine Free Cortisol (UFC)
- Provides an integrated assessment of cortisol secretion over 24 hours.
- Not affected by conditions that alter serum cortisol levels (e.g., protein binding changes).
- Multiple collections may be needed since patients with Cushing disease can have cyclic hypercortisolism.
- Uses assay-specific upper limit of normal as cutoff.
D. Late-Night Salivary Cortisol
- Normally cortisol reaches a nadir around midnight; Cushing patients lose this nadir.
- Normal (ELISA): salivary cortisol < 145 ng/dL at bedtime.
- Convenient: can be done at home.
- Accuracy similar to 24-hr UFC.
- False positives possible in hypertension and diabetes.
E. CRH Stimulation Test
- Corticotropin-releasing hormone (CRH) is administered IV; ACTH and cortisol responses are measured.
- Useful in combination with DST to differentiate pituitary Cushing disease from ectopic ACTH syndrome.
- Pituitary adenomas typically show an exaggerated ACTH/cortisol response to CRH; ectopic tumors do not.
F. Inferior Petrosal Sinus Sampling (IPSS)
- Gold standard for localizing ACTH source when MRI is negative or equivocal.
- Central-to-peripheral ACTH gradient > 2 (basal) or > 3 (post-CRH) confirms pituitary source.
II. Tests for Adrenal Hypofunction
A. Short (Rapid) Cosyntropin Stimulation Test
The most widely used test for adrenal insufficiency.
- Rationale: ACTH (cosyntropin = synthetic ACTH) stimulates the adrenal cortex to produce cortisol. Patients with adrenal destruction (Addison disease) show no or inadequate cortisol rise.
- Protocol:
- Baseline morning cortisol drawn.
- Cosyntropin 250 µg given IM or IV.
- Cortisol measured at 30 and 60 minutes.
- Normal response: Peak cortisol ≥ 18-20 µg/dL (500-550 nmol/L), or a rise (Δ) of 7-10 µg/dL. (The peak value is more diagnostic than the delta.)
- Abnormal: Inadequate rise suggests primary adrenal insufficiency.
- Note: Patients with pituitary/hypothalamic dysfunction (secondary/tertiary insufficiency) may show a partial rise, as some adrenal function is preserved initially.
- Low-dose variation: 1 µg cosyntropin (more physiologic); slightly greater sensitivity for mild adrenal insufficiency; comparable overall diagnostic accuracy to the 250 µg test.
B. Prolonged (Multi-day) Cosyntropin Stimulation Test
- Cosyntropin infusion over 2-5 days with plasma/urine cortisol measured.
- Useful when chronic ACTH deficiency has caused adrenal cortical atrophy (secondary insufficiency).
- Primary adrenal insufficiency: no rise even with prolonged stimulation.
- Secondary insufficiency: cortisol rises progressively as atrophied adrenal cortex is "re-trained."
C. Insulin Tolerance Test (ITT) / Insulin-Induced Hypoglycemia
- Insulin is administered to induce hypoglycemia (blood glucose < 40 mg/dL), which is a powerful stress stimulus for ACTH and GH release.
- Normal response: Serum cortisol rises to > 18-20 µg/dL.
- Tests the entire HPA axis (hypothalamus → pituitary → adrenal), unlike cosyntropin which only tests adrenal reserve.
- Contraindicated in coronary artery disease, epilepsy, or severe hypopituitarism.
- Considered the gold standard for diagnosing secondary/tertiary adrenal insufficiency.
III. Metyrapone Test
- Metyrapone blocks steroid 11-hydroxylation, inhibiting cortisol and corticosterone synthesis.
- In a normal person, falling cortisol removes negative feedback → pituitary releases more ACTH → adrenal produces more 11-deoxycortisol (cortisol precursor that accumulates).
- Protocol: 300-500 mg every 4 hours for 6 doses; 24-hr urine 17-hydroxycorticoids (17-OHCS) measured before and after. Alternatively, 2-3 g orally at midnight with 8 AM measurement of plasma 11-deoxycortisol or ACTH.
- Normal response: ≥ 2-fold increase in urinary 17-OHCS; 11-deoxycortisol rises in blood.
- Uses:
- Assesses pituitary ACTH reserve (secondary adrenal insufficiency).
- In Cushing syndrome: a normal metyrapone response rules out autonomous cortisol-secreting adrenal adenoma/carcinoma (those suppress ACTH and atrophy the normal adrenal cortex).
IV. Tests for Mineralocorticoid (Aldosterone) Function
Primary Hyperaldosteronism (Conn Syndrome) Screening
- Plasma Aldosterone-to-Renin Ratio (ARR):
- ARR > 20 with plasma aldosterone > 15 ng/dL is suggestive of primary hyperaldosteronism.
- An aldosterone:PRA ratio > 50 is highly suggestive.
- Primary hyperaldosteronism: high aldosterone + low renin (volume expansion suppresses renin).
- Secondary hyperaldosteronism: high aldosterone + high renin.
Fludrocortisone Suppression / Salt Loading Test (Confirmatory)
- Aldosterone should suppress with sodium loading in normal individuals.
- Failure to suppress aldosterone confirms primary hyperaldosteronism.
V. Tests for Adrenal Medullary Function
- 24-hour urine catecholamines and metanephrines: primary screening for pheochromocytoma.
- Plasma free metanephrines: high sensitivity for pheochromocytoma (preferred screening in high-risk patients).
- Normal: urine metanephrines < 1.3 mg/day; plasma normetanephrine < 0.9 nmol/L, plasma metanephrine < 0.5 nmol/L.
Summary Table
| Test | Purpose | Key Result |
|---|---|---|
| Overnight 1 mg DST | Screen for Cushing | Cortisol < 1.8 µg/dL = normal |
| 24-hr UFC | Confirm hypercortisolism | Above assay ULN = abnormal |
| Late-night salivary cortisol | Screen for Cushing | > 145 ng/dL = abnormal |
| High-dose DST | Differentiate Cushing causes | Suppression → pituitary; no suppression → ectopic/adrenal |
| Short cosyntropin test | Diagnose adrenal insufficiency | Peak cortisol ≥ 18-20 µg/dL = normal |
| Insulin tolerance test | Assess full HPA axis | Cortisol > 18-20 µg/dL = normal |
| Metyrapone test | Pituitary ACTH reserve | 2× rise in 17-OHCS = normal |
| Aldosterone:Renin ratio | Screen for primary hyperaldosteronism | ARR > 20 + aldosterone > 15 ng/dL = suspicious |
| Plasma metanephrines | Screen for pheochromocytoma | Elevated = suspicious |
Sources: Harper's Illustrated Biochemistry 32e; Smith & Tanagho's General Urology 19e; Tietz Textbook of Laboratory Medicine 7e; Katzung's Basic & Clinical Pharmacology 16e; Harrison's Principles of Internal Medicine 22e (2025)
This is a shared conversation. Sign in to Orris to start your own chat.