What is the cause of acne and its treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from authoritative sources. Here is a complete answer.
Acne Vulgaris — Causes and Treatment

What Is Acne?
Acne vulgaris is a multifactorial disorder of the pilosebaceous unit (the hair follicle and its associated sebaceous gland). It affects ~85% of people aged 12–24, making it nearly a physiologic occurrence in adolescence, and affects ~40–50 million individuals annually in the US alone. It can cause significant psychosocial harm including anxiety, social isolation, and depression. — Dermatology 2-Volume Set 5e
Causes and Pathogenesis
Four main factors interact to produce acne:
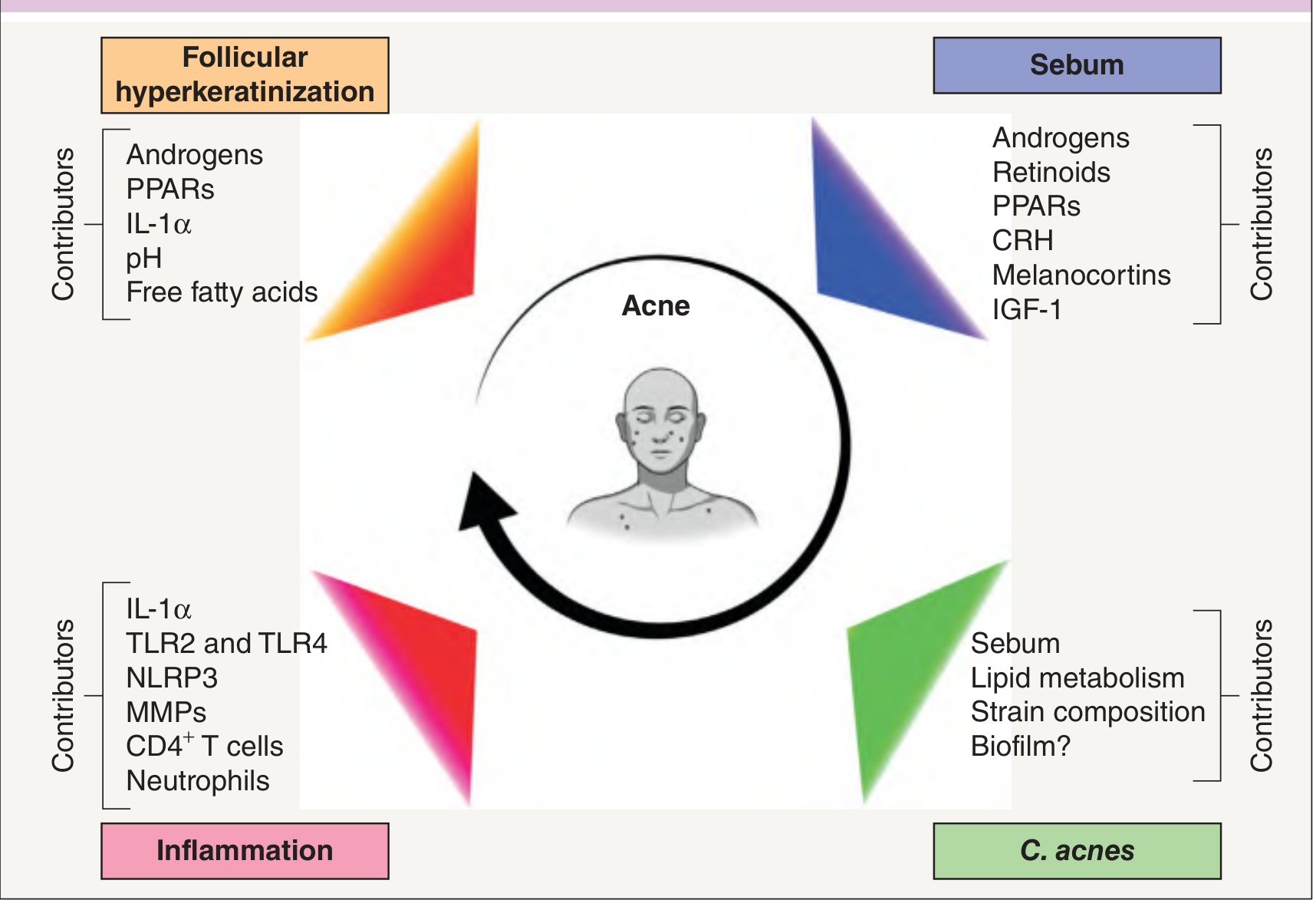
1. Sebaceous Gland Hyperactivity & Excess Sebum Production
Androgens (particularly dihydrotestosterone/DHT) stimulate sebaceous glands to produce excess sebum. Sebum production is the permissive factor — the rise in androgens at puberty is what triggers acne in adolescents. Factors amplifying sebum include IGF-1, CRH, melanocortins, and PPARs. High-glycemic diets and skim milk/whey protein intake may further increase sebum via IGF-1 signaling. — Harrison's 22e; Dermatology 5e
2. Follicular Hyperkeratinization
The follicular canal becomes plugged by abnormal shedding and retention of keratinocytes. Instead of desquamating normally, these cells stick together and accumulate, forming the microcomedone — the earliest, invisible precursor lesion. Androgens, IL-1α, free fatty acids, and PPARs all contribute to this process. — Dermatology 5e
3. Cutibacterium acnes (formerly P. acnes)
This Gram-positive anaerobic bacterium colonizes the sebum-rich follicle. It:
- Hydrolyzes sebum triglycerides into free fatty acids, which are comedogenic and inflammatory
- Activates toll-like receptors (TLR2 and TLR4) on keratinocytes and monocytes
- Triggers NLRP3 inflammasome activation
- Promotes biofilm formation
- Specific strains are associated with acne-prone vs. healthy skin
4. Inflammation
Inflammation is now understood to be present from the very start of acne lesion formation — not just a secondary event. Key mediators include IL-1α (initiates the cascade), TLR2/TLR4 activation, NLRP3 inflammasome, matrix metalloproteinases (MMPs), CD4⁺ T cells, and neutrophils. Rupture of the comedone wall releases oily and keratinous debris, triggering a foreign-body inflammatory reaction. — Harrison's 22e; Dermatology 5e
Contributing / Aggravating Factors
| Factor | Effect |
|---|---|
| Genetics | Sebaceous gland number/size/activity is inherited; concordance in twins is very high |
| High-glycemic diet & skim milk | May worsen acne via IGF-1/insulin axis |
| Medications | Glucocorticoids, lithium, isoniazid, androgenic steroids, progestin-only OCP, phenytoin, halogens |
| Mechanical trauma | Headbands, helmets, chin straps (acne mechanica) |
| Comedogenic topicals | Certain cosmetics and hair products |
| Endocrine disorders | PCOS, hyperandrogenism, hypercortisolism → more severe, treatment-resistant acne |
Treatment
Treatment is guided by acne severity (mild, moderate, severe/nodulocystic) and lesion type (comedonal vs. inflammatory vs. mixed).
Topical Therapies
| Agent | Mechanism | Use |
|---|---|---|
| Benzoyl peroxide (BPO) | Bactericidal (reduces C. acnes), mild keratolytic | First-line for all inflammatory acne; prevents antibiotic resistance |
| Topical retinoids (tretinoin, adapalene, tazarotene) | Normalize follicular keratinization, prevent microcomedone formation, anti-inflammatory | First-line for comedonal acne; should anchor most regimens |
| Topical antibiotics (clindamycin, erythromycin) | Reduce C. acnes, anti-inflammatory | Always combined with BPO to prevent resistance |
| Azelaic acid | Anti-inflammatory, bacteriostatic, comedolytic | Alternative, good for post-inflammatory hyperpigmentation |
| Dapsone gel | Anti-inflammatory | Particularly effective in adult women |
| Salicylic acid | Keratolytic, comedolytic | Mild comedonal acne |
Oral Therapies
| Agent | Indication | Notes |
|---|---|---|
| Oral antibiotics (doxycycline, minocycline, sarecycline) | Moderate–severe inflammatory acne | Use for ≤3–6 months; always combine with BPO; resistance is a growing problem |
| Combined oral contraceptives (COC) | Moderate acne in females | Anti-androgenic effect; FDA-approved agents include norgestimate/ethinyl estradiol |
| Spironolactone | Moderate–severe acne in adult women | Anti-androgen; not for use in males (feminizing effects) |
| Isotretinoin (13-cis retinoic acid) | Severe nodulocystic or scarring acne; acne failing other therapies | Highly effective; targets all four pathogenic factors; teratogenic — requires iPLEDGE program in US; side effects include cheilitis, xerosis, elevated triglycerides, mood monitoring |
Adjunctive / Procedural Approaches
- Comedone extraction — for persistent closed comedones
- Intralesional corticosteroid injection — for large, painful cysts (speeds resolution)
- Chemical peels (salicylic acid, glycolic acid)
- Photodynamic therapy — for recalcitrant inflammatory acne
- Laser/light therapies — blue light (targets porphyrins of C. acnes)
Treatment by Severity (Summary)
| Severity | Recommended Approach |
|---|---|
| Mild comedonal | Topical retinoid ± salicylic acid |
| Mild–moderate inflammatory | Topical retinoid + BPO ± topical antibiotic |
| Moderate–severe inflammatory | Above + oral antibiotic (short course); oral contraceptive or spironolactone in women |
| Severe / nodulocystic / scarring | Oral isotretinoin |
Key principles:
- Topical retinoids are the backbone of most regimens — they address the root cause (microcomedone formation)
- BPO should almost always be included to prevent antibiotic resistance
- Isotretinoin is the only treatment that can produce prolonged remission by targeting all four pathogenic factors simultaneously
- Treatment takes 6–8 weeks to show meaningful improvement; patience is essential
Sources: Harrison's Principles of Internal Medicine 22e; Dermatology 2-Volume Set 5e (Griffiths et al.)
This is a shared conversation. Sign in to Orris to start your own chat.