Explain anatomy and clinical correlates of perineum in full detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content needed to write a comprehensive, detailed answer. Let me compile it.
Anatomy and Clinical Correlates of the Perineum
1. Definition and Overview
The perineum is a diamond-shaped region positioned inferiorly to the pelvic floor, between the thighs. It is the space that lies below the pelvic diaphragm and between the lower limbs. Its:
- Peripheral boundary (floor): The pelvic outlet
- Ceiling (roof): The pelvic diaphragm - formed by the levator ani and coccygeus muscles
- Narrow lateral walls: Walls of the pelvic cavity below the attachment of the levator ani
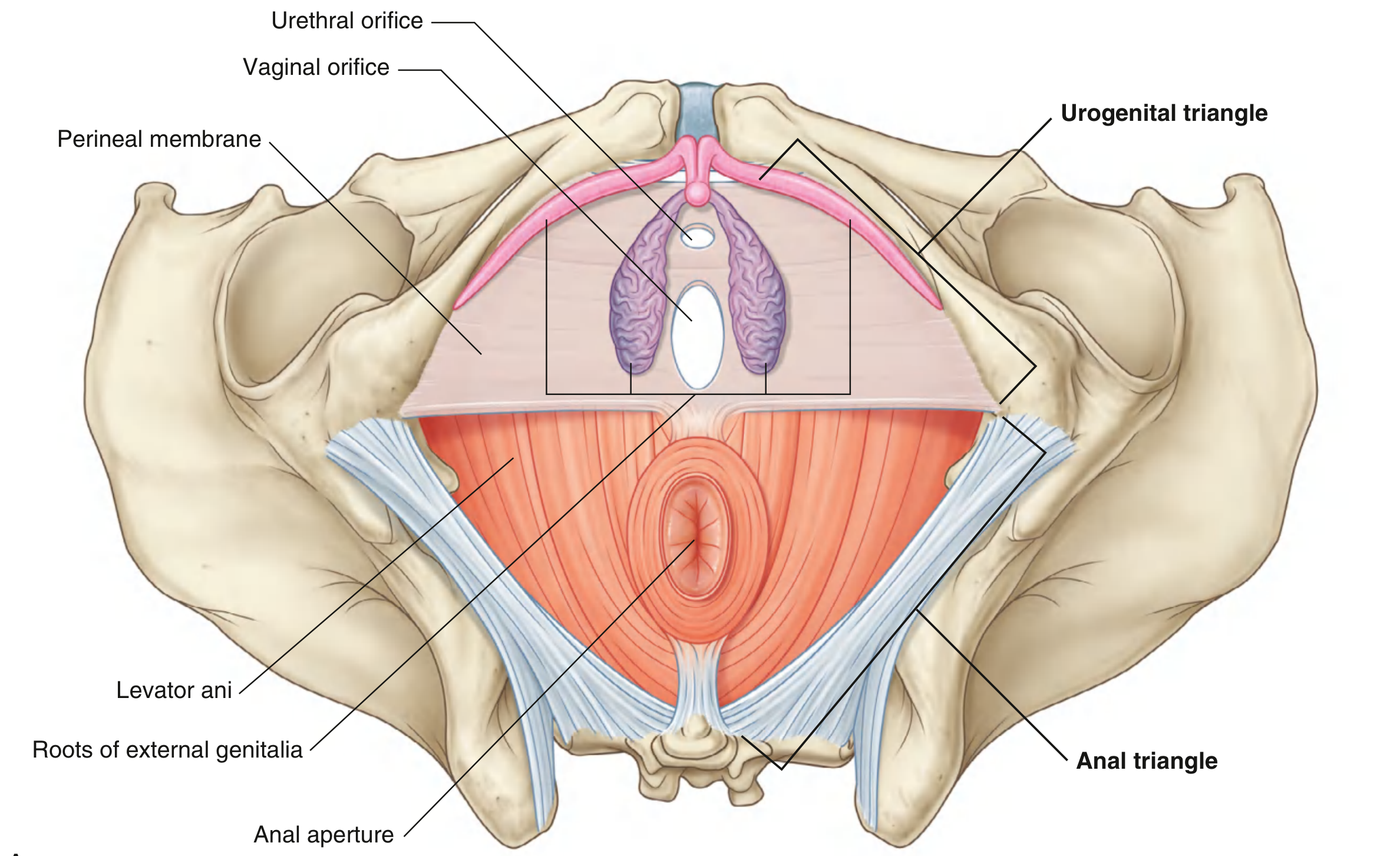
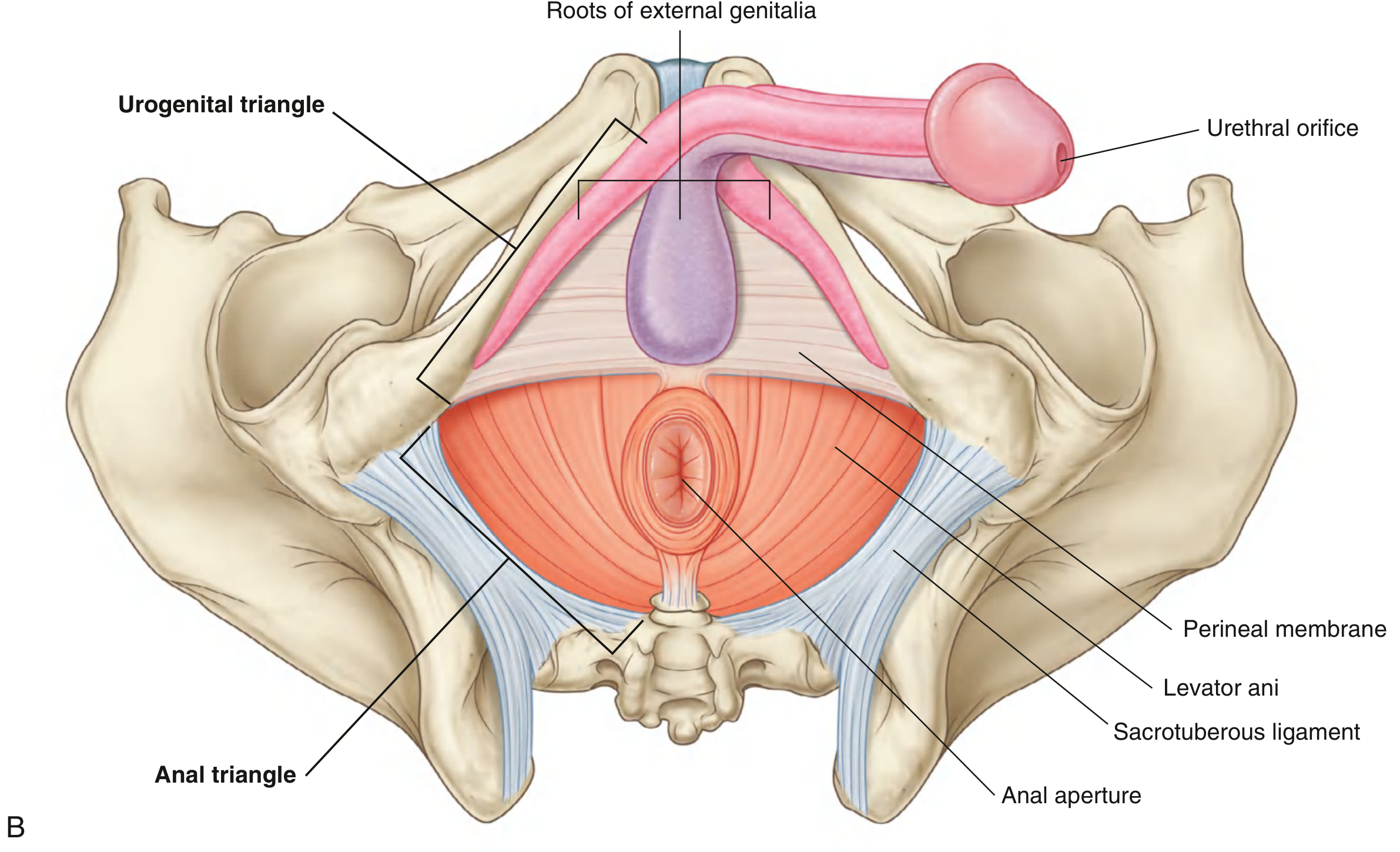
The two triangles of the perineum are not coplanar - in the anatomical position, the urogenital triangle is oriented horizontally (facing inferiorly), while the anal triangle is tilted upward at the transtubercular line, facing more posteriorly.
- Gray's Anatomy for Students, p. 579
2. Boundaries
| Landmark | Point of the Diamond |
|---|---|
| Inferior border of pubic symphysis | Anterior apex |
| Tip of coccyx | Posterior apex |
| Ischial tuberosities (bilateral) | Lateral corners |
| Ischiopubic rami | Anterolateral margins |
| Sacrotuberous ligaments | Posterolateral margins |
Clinical note: The pubic symphysis, ischial tuberosities, and coccyx are all palpable on the patient and are used to define perineal boundaries in the lithotomy position. - Gray's Anatomy for Students, p. 600
3. Division into Two Triangles
An imaginary transverse line connecting the two ischial tuberosities divides the perineum into two triangles:
| Triangle | Location | Contents |
|---|---|---|
| Urogenital triangle | Anterior | External genitalia, urethra (+ vagina in women) |
| Anal triangle | Posterior | Anus, external anal sphincter, ischio-anal fossae |
4. Fasciae of the Perineum
4.1 Superficial Perineal Fascia
Has two layers:
- Superficial fatty layer (Camper's fascia equivalent): Greatly diminished in males (replaced by dartos smooth muscle in the penis and scrotum). Continuous with the superficial fatty layer of the abdominal wall.
- Deep membranous layer (Colles fascia): A tough membranous sheet with specific attachments:
- Posterior: To the posterior margin of the perineal membrane
- Lateral: To the fascia lata of the medial thigh (at the ischiopubic ramus) - defines the perineal-thigh crease
- Anterior: Continuous with dartos fascia of the penis/scrotum and Scarpa's fascia of the abdomen
- In females, it covers the clitoris (analogous to dartos in the male) and fuses posteriorly with the inferior fascia of the urogenital diaphragm at the perineal body
Clinical correlate - Colles fascia and urethral rupture: Because Colles fascia is attached posteriorly to the perineal membrane and laterally to the fascia lata, extravasated urine from a ruptured bulbar urethra is confined to the perineum and lower abdominal wall. It cannot track into the thighs (fascial barrier) or above the inguinal ligaments. This explains the characteristic "butterfly" bruising pattern of perineal hematoma.
4.2 Perineal Membrane (formerly Urogenital Diaphragm)
A thick triangular fibrous sheet that spans between the two inferior ischiopubic rami, filling the urogenital triangle. Key features:
- Free posterior border anchored in the midline to the perineal body
- Lateral attachments to the pubic arch
- Perforated by the urethra (and vagina in women)
- Anterior portion supports the external urethral sphincter
- External genitalia attach to its inferior surface
- Provides support for pelvic viscera above the urogenital hiatus
4.3 Denonvilliers Fascia
The perineal body blends superiorly with the rectovesical septum, which is contiguous with Denonvilliers fascia - important in pelvic surgery.
5. The Perineal Body
The perineal body (central tendon of the perineum) is a fibromuscular mass located in the midline at the junction of the urogenital and anal triangles - between the posterior vaginal wall (or bulb of the penis) anteriorly and the anal canal posteriorly.
Muscles converging into the perineal body:
- Bulbospongiosus (bilateral)
- External anal sphincter (subcutaneous portion)
- Superficial transverse perineal muscles (bilateral)
- Deep transverse perineal muscles
- Fibers from the levator ani (puboanalis)
Clinical correlate - Obstetric injury: Damage to the perineal body during parturition can injure fibers of the external anal sphincter, leading to fecal incontinence. This is why episiotomy is angled mediolaterally (not midline) to avoid damage to the anal sphincter and perineal body. Disruption of the perineal body during perineal prostatectomy also risks postoperative urinary (and possibly fecal) incontinence. - Campbell Walsh Wein Urology, p. 3234
6. The Urogenital Triangle
6.1 Perineal Pouches
The urogenital triangle is divided into two pouches by the perineal membrane:
Superficial Perineal Pouch
Located between the perineal membrane (above) and Colles fascia (below). Contains:
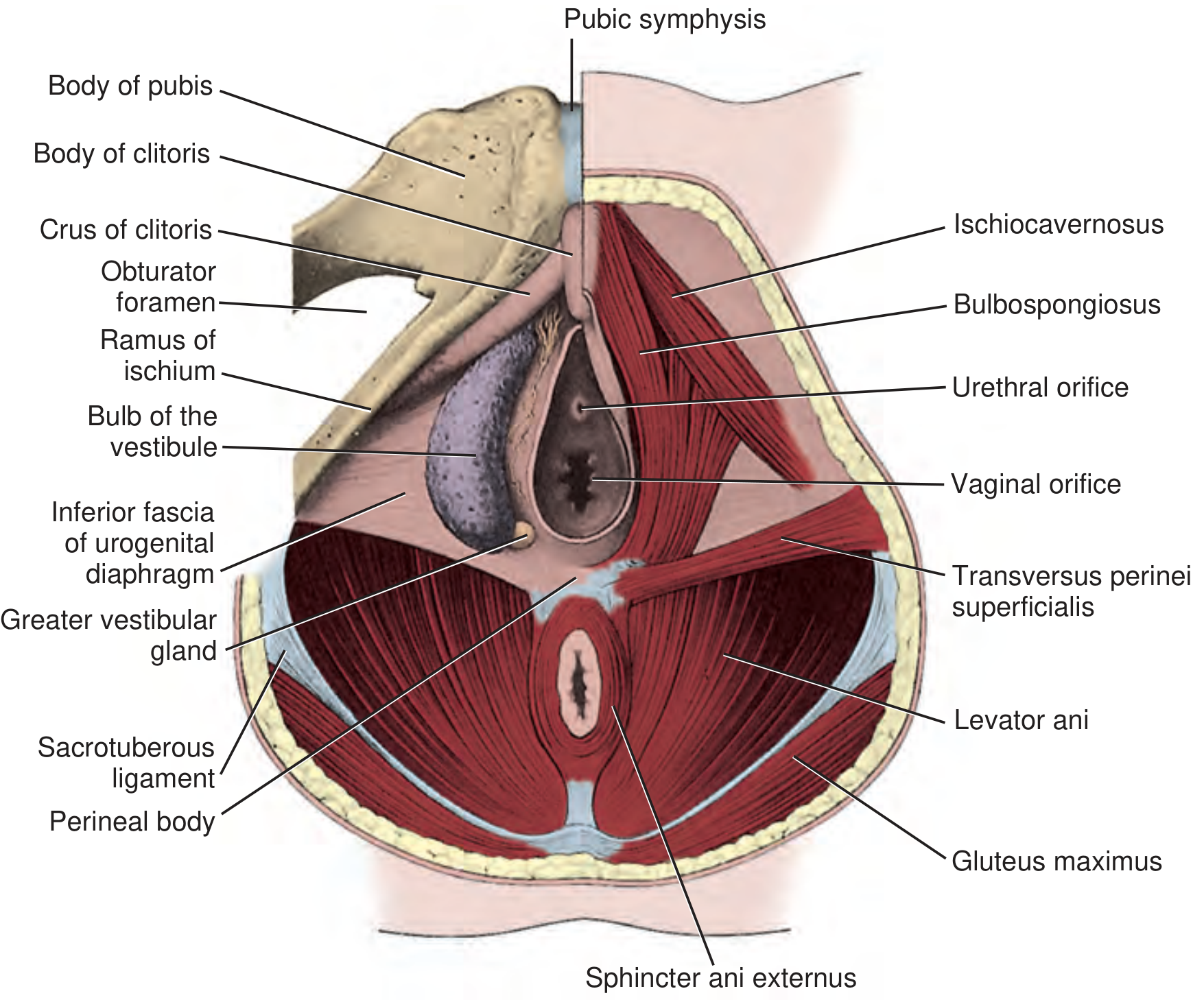
Erectile structures:
- Paired corpora cavernosa - cylindrical, anchored by their proximal ends (crura) to the ischiopubic rami
- In women: crura form the body of the clitoris
- In men: join to form the dorsal part of the penile body
- Second erectile set (around urogenital openings):
- In women: paired bulbs of the vestibule - anchored to the perineal membrane on either side of the vaginal opening; connected anteriorly to the glans clitoris via small bands
- In men: single corpus spongiosum (equivalent to bulbs + interconnecting bands fused at midline) - enclosing the urethra, expanding distally to form the glans penis
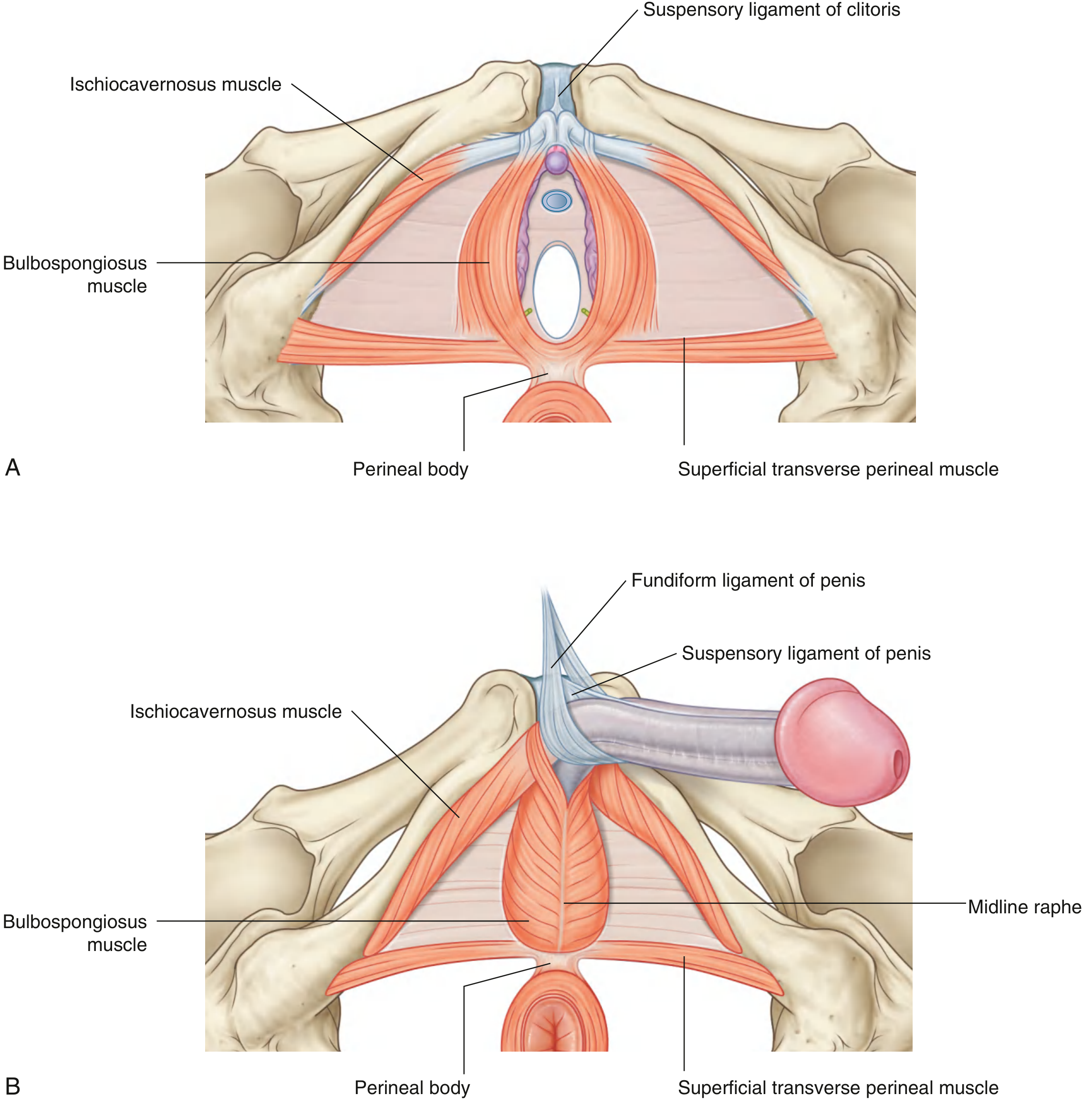
Skeletal muscles of the superficial pouch:
| Muscle | Origin | Insertion | Innervation | Function |
|---|---|---|---|---|
| Ischiocavernosus | Ischial tuberosity and ramus | Crus of penis/clitoris | Pudendal n. (S2-S4) | Forces blood from crura into penile/clitoral body during erection |
| Bulbospongiosus | Perineal body (+ midline raphe in men) | Bulb of vestibule, perineal membrane, clitoral body (female); perineal membrane, corpus cavernosum (male) | Pudendal n. (S2-S4) | Forces blood distally to glans; in men: expels residual urine + pulsatile ejaculation |
| Superficial transverse perineal | Ischial tuberosity and ramus | Perineal body | Pudendal n. (S2-S4) | Stabilizes perineal body |
Other structures in the superficial pouch:
- Greater vestibular glands (Bartholin's glands) in women - positioned at the posterior ends of the bulbs of the vestibule
- Bulbo-urethral glands (Cowper's glands) in men (technically in the deep pouch)
Deep Perineal Pouch
A thin region immediately superior to the perineal membrane, containing skeletal muscle and neurovascular tissue.
Muscles of the deep pouch:
| Muscle | Notes |
|---|---|
| External urethral sphincter | Skeletal (voluntary) muscle; surrounds the urethra; in women also called urethrovaginalis |
| Compressor urethrae | Female only; compresses urethra |
| Deep transverse perineal | Spans between ischiopubic rami; supports perineal body |
The urethra (and vagina in women) traverse both the deep perineal pouch and perineal membrane to reach the perineum. The deep pouch also contains terminal portions of the internal pudendal vessels and pudendal nerve.
7. The Anal Triangle
7.1 Boundaries
- Anterior: Transverse line between ischial tuberosities
- Lateral: Medial margins of sacrotuberous ligaments
- Posterior: Coccyx
- Ceiling: Pelvic diaphragm (levator ani + coccygeus)
7.2 External Anal Sphincter
A voluntary (skeletal muscle) sphincter with three parts arranged sequentially from above downward:
| Part | Attachments | Notes |
|---|---|---|
| Deep | Blends with levator ani fibers (puborectalis) | Thick ring at upper anal canal |
| Superficial | Anchored to perineal body anteriorly, anococcygeal ligament + coccyx posteriorly | True voluntary sphincter |
| Subcutaneous | Attached to perineal body via central tendon | Horizontally flattened disc encircling anal aperture just beneath skin |
The external sphincter is innervated by the inferior rectal nerve (branch of pudendal, S2-S4).
7.3 Internal Anal Sphincter
- Involuntary (smooth muscle)
- Thickening of the inner circular muscle layer of the rectum
- Surrounds the upper two-thirds of the anal canal
- Autonomic innervation: Tonic contraction maintained by sympathetic nerves; relaxed by parasympathetics during defecation
Continence depends on: Integrated function of the internal and external sphincters, puborectalis, intact neurosensory pathways, rectal compliance, anorectal sensation, and anal sphincter resting tone.
7.4 Ischio-anal (Ischiorectal) Fossa
- Paired inverted wedge-shaped fat-filled spaces on either side of the anal canal
- Walls:
- Medial wall: levator ani muscle
- Lateral wall: ischium, obturator internus muscle, and sacrotuberous ligament
- Roof: levator ani attached to obturator internus fascia
- Contents: Fat, pudendal vessels and nerve (in Alcock's canal on lateral wall), inferior rectal vessels and nerves crossing medially
- Anteriorly continuous with recesses that project into the urogenital triangle, superior to the deep perineal pouch (pyramid-shaped, apex pointing toward pubis)
- Posteriorly continuous with the pelvic cavity through the sciatic foramina
Clinical correlate - Anorectal abscesses and fistulas: The anal mucosa is vulnerable to tearing by hard feces. Infection of anal sinuses/crypts spreads between the internal and external sphincters creating intersphincteric fistulas. This can track superiorly into the pelvis or laterally into the ischio-anal fossae, producing perianal abscesses. Because the fossae communicate posteriorly through the post-anal space, infection can pass from one side to the other creating a "horseshoe abscess." - Gray's Anatomy for Students, p. 581
7.5 Anococcygeal Ligament
Fibrous band running between the external anal sphincter and the coccyx, supporting the anal canal.
8. Pudendal Nerve (S2-S4) - The Master Nerve of the Perineum
The pudendal nerve is the principal somatic nerve of the perineum. It arises from the sacral plexus (S2-S4).
Course:
- Leaves pelvis through the greater sciatic foramen, below piriformis
- Crosses the ischial spine (lateral to sacrospinous ligament)
- Re-enters the perineum through the lesser sciatic foramen
- Travels in Alcock's canal (pudendal canal) - a fascial tunnel on the medial surface of obturator internus muscle along the lateral wall of the ischio-anal fossa
- Gives off three terminal branches:
| Branch | Area Supplied |
|---|---|
| Inferior rectal nerve (often multiple) | Penetrates pudendal canal fascia; crosses ischio-anal fossa medially → external anal sphincter, levator ani fibers, skin of anal triangle |
| Perineal nerve | Motor to superficial and deep perineal pouches; sensory via posterior scrotal/labial nerves |
| Dorsal nerve of penis/clitoris | Enters deep perineal pouch; exits through perineal membrane near pubic symphysis; sensory to the glans (most important for orgasm) |
Other somatic nerves entering the perineum:
- Ilio-inguinal nerve (L1)
- Genitofemoral nerve (L1-L2)
- Posterior femoral cutaneous nerve (S1-S3)
- Anococcygeal nerves
Visceral (autonomic) innervation:
- Erection (parasympathetic): Pelvic splanchnic nerves (S2-S4) → inferior hypogastric plexus → cavernous nerves → erectile tissues in deep perineal pouch
- Ejaculation/orgasm (sympathetic): Postganglionic sympathetics via gray rami → delivered into perineum along pudendal nerve; also L1-L2 via hypogastric nerve
- Bladder neck (sympathetic): Adrenergic fibers close bladder neck allowing antegrade ejaculation
Clinical correlate - Pudendal nerve block: The pudendal nerve is blocked at the ischial spine, where it is accessible as it crosses between the sacrospinous and sacrotuberous ligaments. A needle is directed toward the ischial spine transperineally or transvaginally. This provides analgesia for perineal repairs, instrumental deliveries, and minor perineal procedures.
Clinical correlate - Pudendal neuralgia (Alcock's canal syndrome): Chronic perineal pain from pudendal nerve entrapment within Alcock's canal or at the ischial spine. Classic: pain worsened by sitting, relieved by standing; no nocturnal pain. Treated with nerve blocks or surgical decompression.
9. Blood Supply
9.1 Arteries
Internal pudendal artery - the principal artery:
- Origin: Anterior trunk of internal iliac artery
- Course: Leaves pelvis via greater sciatic foramen (with pudendal nerve) → crosses ischial spine → re-enters via lesser sciatic foramen → travels in Alcock's canal
| Branch | Supply |
|---|---|
| Inferior rectal artery(ies) | Cross ischio-anal fossa → external anal sphincter + anal skin; anastomose with middle and superior rectal arteries |
| Perineal artery | Transverse perineal branch + posterior scrotal/labial artery |
| Artery to bulb of penis/vestibule | Corpus spongiosum / bulbs of vestibule |
| Urethral artery | Penile urethra and surrounding erectile tissue |
| Deep artery of penis/clitoris | Penetrates perineal membrane → enters crus → corpora cavernosa (responsible for corporal engorgement) |
| Dorsal artery of penis/clitoris | Dorsal surface of penile/clitoral body → glans; anastomoses with deep artery |
External pudendal arteries (from femoral artery): Supply skin of penis/scrotum or clitoris/labia majora anteriorly.
Testicular arteries (from aorta): Descend via inguinal canal to testes.
9.2 Veins
- Perineal veins generally accompany arteries → drain into internal pudendal veins → internal iliac vein
- Deep dorsal vein of the penis: unpaired, runs in midline dorsum of penis, drains into the dorsal venous complex (Santorini's plexus) in the pelvis
- Internal rectal venous plexus (between rectum, puborectalis, and levator ani) and external rectal plexus (deep to sphincters) both drain into middle rectal vein
- Superior rectal vein drains into the inferior mesenteric vein (portal system); inferior rectal vein drains into the pudendal vein (systemic) - a portosystemic anastomosis site
Clinical correlate - Haemorrhoids: The portosystemic anastomosis at the anorectal junction is the anatomical basis for haemorrhoidal venous engorgement in portal hypertension.
9.3 Lymphatics
- Superficial perineal skin and external genitalia: Drain to superficial inguinal lymph nodes
- Deep structures (deep perineal pouch, erectile tissues): Drain to internal iliac lymph nodes
- Exception: The testes drain directly to para-aortic nodes (not inguinal), which is clinically important in testicular tumours
10. Deep Perineal Pouch and External Urethral Sphincter - Clinical Significance
The external urethral sphincter (skeletal, voluntary) in the deep perineal pouch is the mechanism of voluntary micturition control. In men, the bladder neck also contributes an internal sphincter (smooth, involuntary, sympathetically maintained). After radical prostatectomy, the internal sphincter is removed, leaving only the external sphincter for continence - hence post-prostatectomy incontinence occurs when the external sphincter is also damaged.
11. External Genitalia - Surface Features
In Women (Vulva)
- Labia majora: Two large skin folds on either side of the midline
- Labia minora: Two thinner skin folds medial to the labia majora; enclose the vestibule
- Vestibule: Region between labia minora into which the urethra and vagina open, plus the openings of the greater vestibular (Bartholin's) glands
- Clitoris: Anterior apex; the prepuce (hood) is formed by fusion of labia minora; the frenulum attaches posteriorly to the glans
- Hymen: Remnant of tissue at the vaginal opening
- Posterior fourchette (frenulum of labia): Posterior commissure of the labia minora
In Men
- Scrotum: Divided by median raphe into two compartments, each containing a testis, epididymis, and spermatic cord
- Penis: Body formed by paired corpora cavernosa (dorsal) + corpus spongiosum (ventral, enclosing urethra); glans penis at tip with external urethral meatus; prepuce covers glans when uncircumcised
12. Key Clinical Correlates
12.1 Straddle Injuries (Perineal Trauma)
Straddle injuries compress the perineum against the ischiopubic rami. The bulbar urethra is the most commonly injured structure as it lies in the superficial perineal pouch against the perineal membrane. Extravasation of urine is confined by Colles fascia - classically spreading to the scrotum, perineum, and anterior abdominal wall (deep to Scarpa's fascia) but NOT into the thighs or buttocks.
12.2 Episiotomy
Surgical incision of the perineum during childbirth. Mediolateral technique (angled 45-60° from the midline) is preferred over median episiotomy to avoid damage to the external anal sphincter fibers and perineal body, which would cause 3rd and 4th degree perineal tears.
12.3 Bartholin's Gland Cyst/Abscess
The greater vestibular (Bartholin's) glands lie at the posterior ends of the vestibular bulbs, in the superficial perineal pouch. Obstruction causes Bartholin's cyst; secondary infection causes Bartholin's abscess. Treatment is incision + drainage or marsupialization.
12.4 Erectile Dysfunction
Erection requires intact parasympathetic (S2-S4) pelvic splanchnic nerve supply via the cavernous nerves. At-risk in:
- Radical prostatectomy (nerve-sparing vs. non-nerve-sparing approach)
- Radiation for pelvic malignancy
- Diabetes (autonomic neuropathy)
- Cardiovascular disease (arterial insufficiency to internal pudendal)
- Spinal cord injuries
- Multiple sclerosis
Ejaculation is absent after radical prostatectomy (seminal vesicles and prostate removed) but orgasm remains possible because the pudendal nerve (S2-S4) is preserved - the sensation pathways are separate from the emission/ejaculation pathways.
12.5 Perineal Prostatectomy (Surgical Approach)
The prostate can be approached perineally via:
- Young procedure: Divides the central tendon (perineal body) and sphincteric attachments, leaving the external sphincter on the rectum
- Belt procedure: Goes under the external sphincter along the anterior rectal wall
Disruption of the perineal body risks postoperative urinary and fecal incontinence.
12.6 Fournier's Gangrene
Necrotizing fasciitis of the perineum - a urological emergency. Infection (often polymicrobial) spreads rapidly along perineal fascial planes (Colles fascia, Buck's fascia). Spreads to scrotum, perineum, and lower abdominal wall. Requires emergency wide surgical debridement.
12.7 Fecal Incontinence
Complex, multifactorial. The key anatomical components:
- External anal sphincter integrity (pudendal nerve damage in obstetric injury, surgery)
- Internal sphincter tone
- Puborectalis sling
- Intact anorectal sensation Obstetric injury is the most common cause in women.
12.8 Lithotomy Position
The standard position for perineal examination and surgery. Thighs are flexed and abducted to expose the perineum. Prolonged lithotomy carries risk of compartment syndrome of the leg and common peroneal nerve palsy (from lateral leg compression).
12.9 Perianal/Ischiorectal Abscess
Because the ischio-anal fossae communicate posteriorly behind the external sphincter (post-anal space), infection can track from one side to the other producing a horseshoe abscess - requiring bilateral drainage.
13. Summary Table - Compartments at a Glance
| Compartment | Contents | Roof | Floor/Boundary |
|---|---|---|---|
| Superficial perineal pouch | Crura, bulb/vestibular bulbs, ischiocavernosus, bulbospongiosus, superficial transverse perineal, Bartholin's glands | Perineal membrane | Colles fascia |
| Deep perineal pouch | External urethral sphincter, compressor urethrae, deep transverse perineal, terminal pudendal vessels/nerve | Superior fascia of perineal membrane | Perineal membrane itself |
| Ischio-anal fossa | Fat, inferior rectal vessels/nerves, pudendal canal (Alcock's canal) | Levator ani | Perineal skin |
Key sources:
- Gray's Anatomy for Students (9780323934237), pp. 579-603
- Campbell Walsh Wein Urology (9780323546423), pp. 3218-3241
This is a shared conversation. Sign in to Orris to start your own chat.