2nd year bds pathology multiple myeloma
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the content and images needed for a comprehensive 2nd year BDS pathology answer on multiple myeloma. Here is the complete response:
Multiple Myeloma - 2nd Year BDS Pathology
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
Definition
Multiple myeloma is a malignant neoplasm of plasma cells (terminally differentiated B lymphocytes), characterized by:
- Bone marrow infiltration by clonal plasma cells
- Production of a monoclonal immunoglobulin (M protein)
- Extensive skeletal destruction
- Systemic effects on kidneys, immune system, and blood
Epidemiology
| Feature | Detail |
|---|---|
| Incidence | ~30,000 new cases/year in the USA; 1% of all cancer deaths in Western countries |
| Age | Peak at 65-70 years; rare under 40 |
| Sex | More common in males |
| Race | Higher incidence in people of African descent |
Pathogenesis
Genetic basis:
- Frequent chromosomal translocations involving the IGH locus on chromosome 14q32 fused to proto-oncogenes (cyclin D1, cyclin D3)
- Deletions of chromosome 17p (TP53 locus) - associated with poor prognosis
- Late-stage translocations involving MYC - seen in aggressive disease / plasma cell leukemia
- Mutations in NF-κB pathway genes support B-cell survival
Key cytokine - Interleukin-6 (IL-6):
- Produced by bone marrow stromal cells AND tumor cells themselves
- Major growth and survival factor for myeloma cells
- High serum IL-6 = poor prognosis
Bone destruction mechanism:
- Myeloma cells release MIP1α (CCL3) - a chemokine that activates osteoclasts
- Myeloma-derived factors upregulate RANKL on stromal cells → osteoclast activation
- Other tumor factors inhibit osteoblasts (via Wnt pathway inhibition)
- Net result: uncoupled bone resorption → hypercalcemia + pathologic fractures
M Protein (Monoclonal Protein)
| Type | Frequency |
|---|---|
| IgG | 60% (most common) |
| IgA | 20-25% |
| Light chains only (κ or λ) | ~20% |
| IgM, IgD, IgE | Rare |
| Nonsecretory | ~1% |
- Excess free light chains are small enough to pass through the glomerulus and appear in urine as Bence Jones proteins
- Free and complete M proteins are present together in 60-70% of cases
Morphology
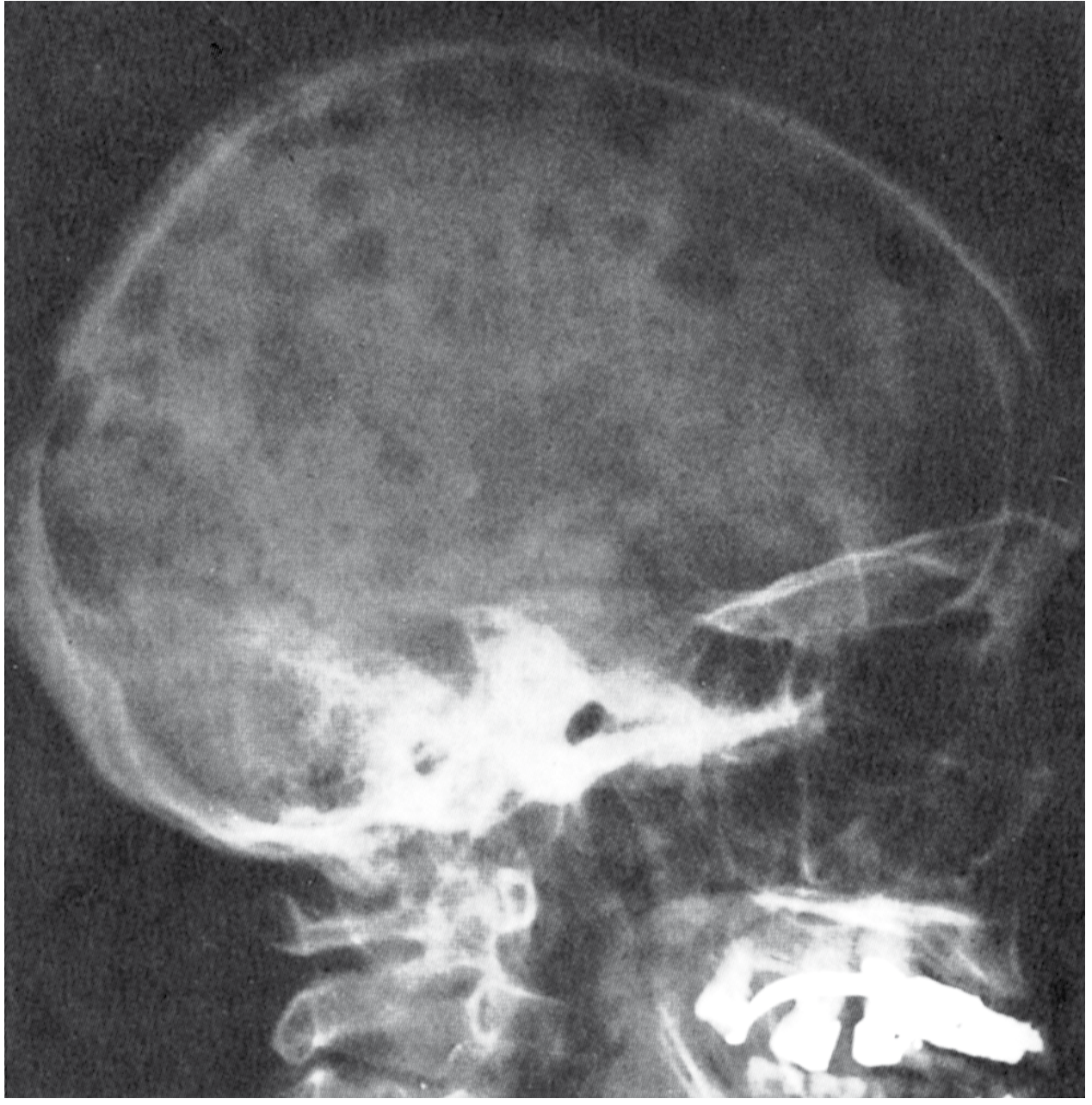
Gross / Radiologic
- Multiple "punched-out" lytic bone lesions, 1-4 cm in diameter
- Lesions begin in medullary cavity, erode cancellous bone, then destroy cortex
- Pathologic fractures - most common in vertebral column and femur
- Bones most commonly affected (in order): vertebral column, ribs, skull, pelvis, femur, clavicle, scapula
- Less commonly: diffuse demineralization (osteopenia) rather than focal defects
Skull X-ray - classic "pepper-pot" or punched-out appearance:
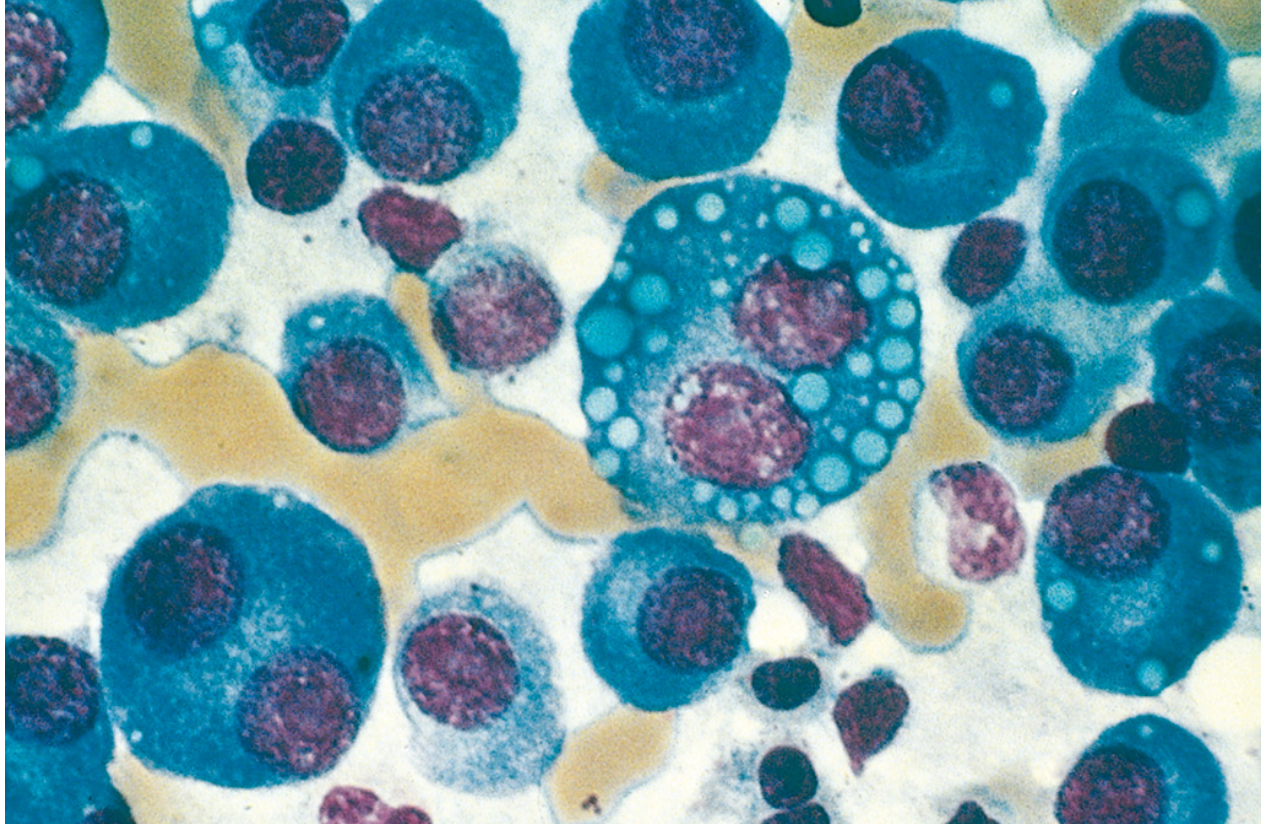
Bone Marrow Histology
- Plasma cells constitute > 30% of marrow cellularity (diagnostic threshold)
- Normal marrow elements are partially or completely replaced
Key cytologic features of myeloma cells:
| Variant | Feature |
|---|---|
| Plasmablasts | Vesicular chromatin, prominent single nucleolus |
| Russell bodies | Cytoplasmic globular immunoglobulin inclusions |
| Dutcher bodies | Nuclear immunoglobulin inclusions |
| Flame cells | Fiery red cytoplasm |
| Mott cells | Multiple grapelike cytoplasmic droplets |
| Multinucleated cells | Seen in advanced disease |
Bone marrow aspirate - myeloma cells with prominent nucleoli and cytoplasmic droplets:
Peripheral Blood - Rouleaux Formation
- High levels of M protein in blood cause red cells to stack in linear arrays (rouleaux)
- Characteristic but not specific (also seen in lupus, early HIV)
Myeloma Kidney (Renal Morphology)
- Proteinaceous casts in distal convoluted tubules and collecting ducts (mainly Bence Jones proteins + albumin)
- Multinucleate giant cells (macrophages) surround the casts
- Adjacent tubular epithelial cells become necrotic/atrophic (toxic effect of Bence Jones proteins)
- Additional renal lesions: metastatic calcification, AL amyloidosis in glomeruli and vessel walls, bacterial pyelonephritis
Immunophenotype
| Marker | Status |
|---|---|
| CD138 (Syndecan-1) | Positive - hallmark of plasma cells |
| CD56 | Often positive - useful for identifying small tumor populations |
| Cytoplasmic κ or λ | Present (light chain restriction = clonality) |
Related Entities (Plasma Cell Neoplasms)
| Entity | Key Feature |
|---|---|
| Smoldering myeloma | High M component, no symptoms - may not require treatment for years |
| Solitary plasmacytoma | Single bony or soft-tissue mass; can progress to myeloma |
| MGUS (Monoclonal Gammopathy of Undetermined Significance) | Common asymptomatic precursor; ~1%/year risk of progression to myeloma |
| Waldenström macroglobulinemia | IgM excess → hyperviscosity; associated with lymphoplasmacytic lymphoma |
| AL amyloidosis | λ light chains deposit as amyloid; 15% of myeloma patients |
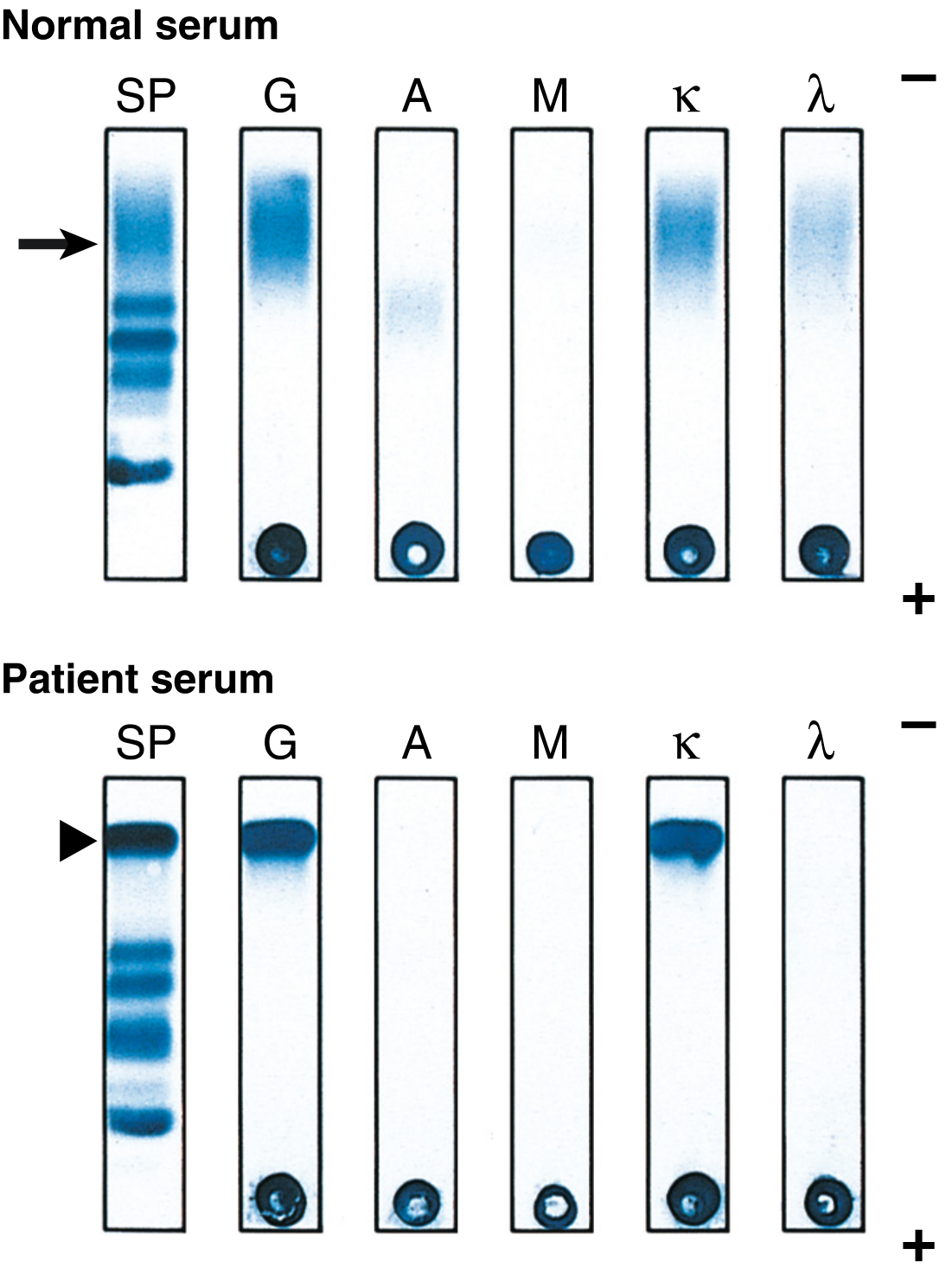
Laboratory Findings
Serum protein electrophoresis (SPEP):
- Normal serum: broad, diffuse band in γ-globulin region
- Myeloma: single, sharp, tall M-spike (narrow spike = monoclonal protein)
Immunofixation electrophoresis (IFE):
- Characterizes the M protein by heavy chain class (G, A, M) and light chain type (κ or λ)
Other lab findings:
- ↑ Serum immunoglobulins (M protein)
- Bence Jones proteinuria (urine light chains) - heat test: precipitates at 40-60°C, re-dissolves at 100°C
- Normocytic normochromic anemia (marrow replacement)
- ↑ ESR, ↑ serum calcium
- Renal failure (elevated creatinine)
- Moderate leukopenia and thrombocytopenia
Clinical Features (Mnemonic: CRAB)
| Letter | Feature | Mechanism |
|---|---|---|
| C - Hypercalcemia | Confusion, weakness, lethargy, constipation, polyuria | Bone resorption |
| R - Renal failure | Up to 50% of patients | Bence Jones toxicity, casts, amyloid, hypercalcemia |
| A - Anemia | Normocytic normochromic | Marrow replacement |
| B - Bone lesions | Pain, pathologic fractures | Osteoclast activation |
Additional features:
- Recurrent bacterial infections - most common cause of death. Myeloma cells suppress normal B-cell function → profound hypogammaglobulinemia despite high total Ig
- Cellular immunity is relatively preserved
- Hyperviscosity (less common than Waldenström)
- AL amyloidosis causing multi-organ deposits
Oral/Dental Relevance (BDS Focus)
- Jaw (mandible) can be involved with lytic bone lesions - may present as unexplained tooth mobility, jaw pain, or a "punched-out" appearance on dental X-rays
- Rare cases present as gingival swelling as the primary oral manifestation
- Solitary plasmacytoma of the jaw has been reported
- Bisphosphonate therapy used for myeloma bone disease carries risk of medication-related osteonecrosis of the jaw (MRONJ), especially with IV zoledronic acid/pamidronate
- Always include multiple myeloma in differential diagnosis of radiolucent jaw lesions in elderly patients
Diagnosis
- Imaging - skeletal survey (skull, spine, pelvis) showing punched-out lytic lesions
- Bone marrow biopsy - > 10% clonal plasma cells (symptomatic myeloma requires ≥ 10% plus organ damage, or ≥ 60%)
- Serum/urine protein electrophoresis - M protein detection
- Immunofixation - characterize M protein class
- Complete blood count - anemia, leukopenia, thrombocytopenia
- Serum calcium, creatinine, β2-microglobulin, LDH - for staging and prognosis
Prognosis
- Patients with multiple bony lesions, if untreated: survival < 6-12 months
- Smoldering myeloma: may not require treatment for years
- Median survival with treatment: ~5 years
- Cures remain rare, but modern agents (proteasome inhibitors, IMiDs, monoclonal antibodies) have significantly improved outcomes
Key exam points for 2nd year BDS:
- Multiple myeloma = plasma cell malignancy - NOT a B-cell lymphoma
- Classic lesion = punched-out lytic bone lesions (no osteoblastic reaction = no increase in serum alkaline phosphatase, unlike metastatic carcinoma)
- Bence Jones protein = free immunoglobulin light chains in urine - hallmark
- M protein/M spike on electrophoresis
- IL-6 = key growth factor
- Russell bodies = cytoplasmic Ig inclusions
- CRAB criteria for diagnosis
- Most common M protein = IgG
This is a shared conversation. Sign in to Orris to start your own chat.