Paper smar
It looks like your message got cut off! Could you finish your thought? Did you mean:
- "Paper smart" - tips for reading/writing papers efficiently?
- "Paper summary" - summarize a specific paper?
- "Paper search" - find papers on a topic?
What were you trying to say?
Paper smear
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Papanicolaou test" AND "cervical cancer screening"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a thorough overview of the Pap smear based on authoritative medical textbooks.
Pap Smear (Papanicolaou Smear)
What Is It?
The Pap smear is a cervical cancer screening test developed by George Papanicolaou in the 1920s. Cells are lightly scraped from the transformation zone of the cervix and examined microscopically for dysplastic or precancerous changes. It remains the most successful cancer-screening test ever developed - cervical cancer was the leading cause of cancer death in women in the US 50 years ago, but the death rate has since declined by approximately 75%. - Robbins Basic Pathology
Purpose and Rationale
The test detects squamous intraepithelial lesions (SIL) - abnormal cell changes driven mainly by persistent high-risk Human Papillomavirus (HPV) infection. Cervical precancerous lesions are detectable by cytology long before any gross abnormality is visible, making the Pap smear extremely valuable for early intervention. - Robbins Basic Pathology
Technique and Sample Collection
- Cells are scraped from the cervix, particularly the transformation zone (squamocolumnar junction), where most precancerous changes arise.
- Conventional slide smear - the traditional method.
- Liquid-based cytology (ThinPrep, SurePath) - FDA-approved alternatives that suspend cells in liquid, reduce obscuring material, and allow reflex HPV DNA testing from the same sample. This is now the dominant method in most settings. - Pfenninger & Fowler's Procedures for Primary Care
The Bethesda Classification System (2001)
Results are reported using standardized Bethesda terminology:
| Cytology Term | Old Term | Histology (CIN) |
|---|---|---|
| ASC-US | Atypical squamous cells of undetermined significance | - |
| ASC-H | Atypical squamous cells, cannot exclude HSIL | - |
| LSIL | Low-grade SIL | CIN 1 |
| HSIL | High-grade SIL | CIN 2 / CIN 3 / Carcinoma in situ |
| AGC | Atypical glandular cells | - |
- Swanson's Family Medicine Review
Histological Spectrum of Cervical Intraepithelial Neoplasia (CIN)
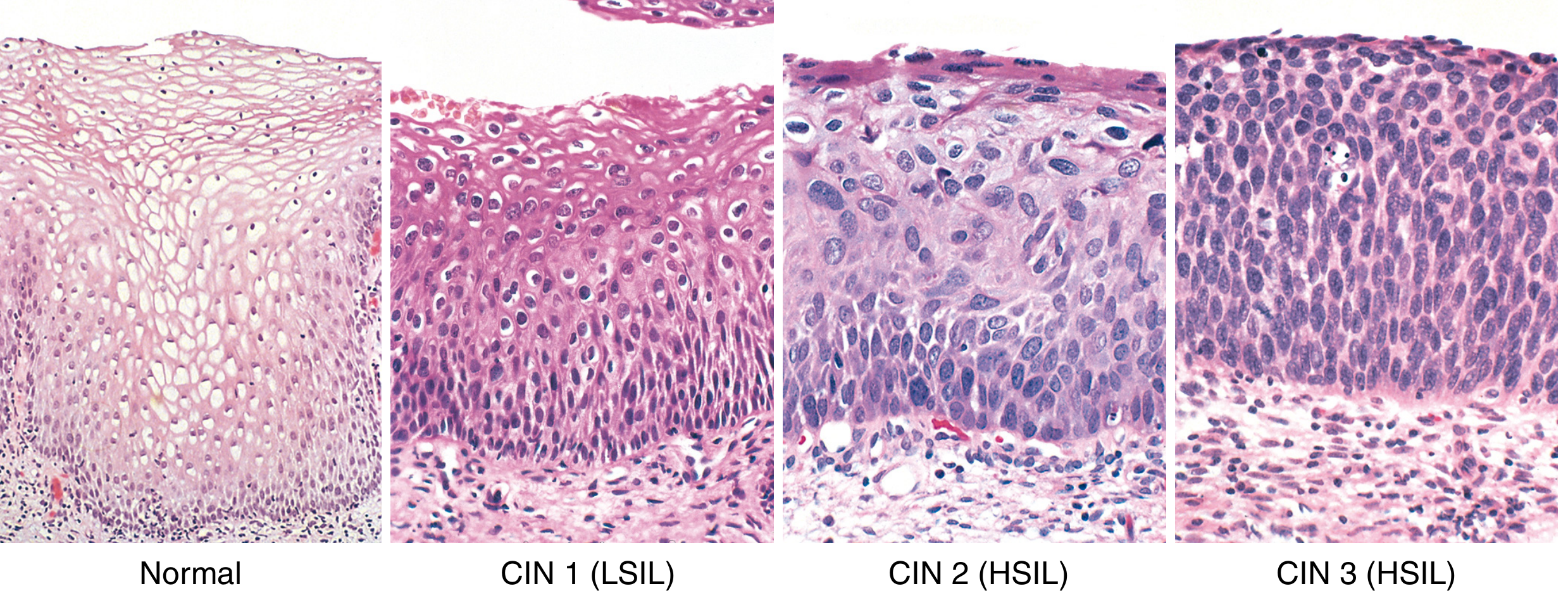
Normal cervical epithelium (left) through CIN 1 (LSIL, koilocytic atypia), CIN 2 (HSIL, progressive atypia), and CIN 3 (HSIL, full-thickness atypia and loss of maturation) - Robbins, Cotran & Kumar Pathologic Basis of Disease
Key microscopic features:
- Nuclear enlargement, hyperchromasia, coarse chromatin
- Koilocytic atypia - perinuclear halos from HPV protein E5 effect on ER membranes
- Grading is based on how far the immature basal cell layer expands upward through the epithelium
| Lesion | Regression | Persist | Progress |
|---|---|---|---|
| LSIL (CIN 1) | 60% | 30% | 10% (to HSIL) |
| HSIL (CIN 2/3) | 30% | 60% | 10% (to carcinoma) |
- Robbins Basic Pathology, Table 17.1
Screening Guidelines (USPSTF)
-
Age < 21: No screening recommended
-
Age 21-29: Pap smear every 3 years
-
Age 30-65: Pap smear every 3 years, OR co-testing (Pap + high-risk HPV DNA) every 5 years
-
Age > 65 or post-hysterectomy (benign): Screening can be discontinued
-
Swanson's Family Medicine Review
HPV Co-testing and Reflex Testing
- High-risk HPV types (especially HPV 16) are the necessary precursor to cervical carcinoma.
- Reflex HPV testing: If a Pap returns ASC-US, HPV DNA testing is automatically performed from the same liquid-based sample.
- HPV testing has 90-96% sensitivity for high-grade lesions vs. 75-85% for repeat Pap alone.
- A negative high-risk HPV test carries a negative predictive value of at least 98%. - Swanson's Family Medicine Review
Management by Result
| Result | Management |
|---|---|
| ASC-US | Reflex HPV testing; if HPV+, colposcopy; if HPV-, routine follow-up |
| ASC-H | Colposcopy |
| LSIL | Usually colposcopy (may observe in some populations) |
| HSIL | Colposcopy + directed biopsy; treat |
| AGC | Colposcopy + endocervical sampling ± endometrial sampling |
Limitations
- A single Pap smear has a false-negative rate of 20-50% for detecting cervical dysplasia, even with the ThinPrep liquid-based method. Serial testing significantly improves sensitivity.
- Errors can occur at multiple points: sampling technique, laboratory preparation, report interpretation, and clinician follow-up. - Pfenninger & Fowler's Procedures for Primary Care
Risk Factors for Cervical Dysplasia
- Persistent high-risk HPV infection (essential prerequisite)
- Smoking
- Immunocompromised state (e.g., HIV)
- Early age of first intercourse
- Multiple sexual partners
Recent Evidence
A 2026 systematic review (PMID 41988240) comparing HPV-based vs. cytology (Pap) screening found that HPV testing has superior sensitivity for detecting cervical precancer. Current guidelines in many countries are shifting toward primary HPV testing, with cytology as a reflex or co-test rather than the standalone first-line method. This does not make the Pap smear obsolete, but does indicate that its role is evolving in systems with access to molecular testing.
In summary: The Pap smear collects cervical cells from the transformation zone, classifies any abnormalities using the Bethesda system (ASC-US through HSIL), and guides management from surveillance to colposcopy and treatment. It is performed every 3 years from age 21, or every 5 years in combination with HPV co-testing from age 30 to 65.
This is a shared conversation. Sign in to Orris to start your own chat.