IMRT in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
IMRT intensity modulated radiation therapy head neck cancer
Searching the Web
IMRT intensity modulated radiotherapy ENT head neck otolaryngology detailed review 2024 2025
Finding Sources
Finding Sources
Searching PubMed
IMRT nasopharyngeal carcinoma laryngeal cancer outcomes toxicity
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
INTENSITY-MODULATED RADIATION THERAPY (IMRT)
A Comprehensive 20-Mark Answer for RGUHS Examinations
Sources: Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, K.J. Lee's Essential Otolaryngology, Dhingra's Diseases of ENT, Hazarika's Textbook of ENT, and recent PubMed literature
1. DEFINITION AND HISTORICAL BACKGROUND
Intensity-Modulated Radiation Therapy (IMRT) is an advanced form of three-dimensional conformal radiotherapy in which the intensity of the radiation beam varies across each treatment field, allowing simultaneous delivery of high dose to the tumor target while sparing adjacent critical normal structures. It was approved for clinical use in head and neck cancers in 1999.
- Cummings Otolaryngology, Ch. 75: "IMRT implies the use of radiation fields whose intensity varies across the field, depending on the thickness of the target and the existence of critical organs or critical non-involved tissue in their path."
- Scott-Brown's Vol 2: "IMRT is now the accepted standard of care for RT treatment planning and delivery."
- K.J. Lee's Essential Otolaryngology, p. 873: "IMRT is a significant advance over 3D-CRT and is now used standardly for treatment of most head and neck tumors."
2. EVOLUTION: FROM CONVENTIONAL RT TO IMRT
┌──────────────────────────────────────────────────────────────────────────────┐
│ EVOLUTION OF RADIOTHERAPY TECHNIQUES │
│ │
│ Orthovoltage RT → Cobalt-60 RT → 2D Conventional RT → 3D-CRT → IMRT│
│ (1940s-50s) (1950s) (1960s-80s) (1990s) (1999→)│
│ │
│ ↓ │
│ IGRT + Adaptive RT │
│ (2005 →) │
│ ↓ │
│ VMAT / Tomotherapy / Proton RT │
└──────────────────────────────────────────────────────────────────────────────┘
3. BASIC PHYSICS AND PRINCIPLE
The Fundamental Concept:
┌─────────────────────────────────────────────────────────────────────┐
│ HOW IMRT DIFFERS FROM CONVENTIONAL RT │
│ │
│ CONVENTIONAL RT: IMRT: │
│ ┌────────────┐ ┌────────────┐ │
│ │ BEAM │ │ BEAMLETS │ │
│ │ (uniform │ │ (varying │ │
│ │ intensity) │ │ intensity) │ │
│ └────┬───────┘ └─────┬──────┘ │
│ │ │ │
│ Uniform dose → Sculpted dose distribution │
│ Rectangular field → Concave/irregular field │
│ Dose = same across beam → Dose varies pixel by pixel │
└─────────────────────────────────────────────────────────────────────┘
Each broad radiation beam is divided into many smaller beams called beamlets. This is achieved using a Multileaf Collimator (MLC) that shapes the beam and modulates the intensity of each beamlet. (Cummings, block26)
4. KEY TECHNICAL COMPONENTS
A. Linear Accelerator (LINAC)
The radiation is delivered by a LINAC producing 6-15 MV photon beams. The gantry rotates around the patient to deliver beams from multiple angles (typically 7-9 fixed fields, or 360° arc).
B. Multileaf Collimator (MLC)
┌─────────────────────────────────────────────┐
│ MULTILEAF COLLIMATOR (MLC) │
│ │
│ [Leaf 1 ───────┐ ┌───────── Leaf 1 ] │
│ [Leaf 2 ─────────┐ ┌─────── Leaf 2 ] │
│ [Leaf 3 ──────────┐┌────────── Leaf 3 ] │ ← Beam aperture
│ [Leaf 4 ─────────┐ ┌─────── Leaf 4 ] │ shaped by leaf
│ [Leaf 5 ───────┐ ┌───────── Leaf 5 ] │ positions
│ [Leaf 6 ─────────────────────── Leaf 6 ] │
│ │
│ Each leaf: 3-10 mm wide (sub-cm resolution) │
└─────────────────────────────────────────────┘
- Leaves move dynamically in and out of each radiation field
- This allows the beam intensity to be modulated at each position
C. Treatment Planning System (TPS) - Inverse Planning
┌──────────────────────────────────────────────────────────────────────────┐
│ INVERSE PLANNING ALGORITHM │
│ │
│ Physician inputs: │
│ • Target dose (e.g., GTV 70 Gy, CTV1 63 Gy, CTV2 54 Gy) │
│ • OAR constraints (e.g., parotid mean dose < 26 Gy) │
│ • Importance (penalty) weights for each structure │
│ ↓ │
│ Computer iterates through thousands of beam intensity combinations │
│ ↓ │
│ Minimizes objective/cost function: │
│ f = Σ [wᵢ × (Dᵢ_delivered - Dᵢ_prescribed)²] │
│ ↓ │
│ Outputs: Optimal fluence map for each beam angle │
│ MLC leaf sequence for delivery │
└──────────────────────────────────────────────────────────────────────────┘
Cummings, Ch. 75: "Inverse planning demands that the planner state the treatment goals in terms of dose and/or dose/volume goals for the targets, and the constraints for the critical normal tissue. The desired solution is the dose distribution that minimizes the variance of the delivered dose relative to the objective function."
5. IMRT DELIVERY TECHNIQUES
┌───────────────────────────────────────────────────────────────────────────┐
│ IMRT DELIVERY TECHNIQUES │
│ │
│ 1. STEP-AND-SHOOT (SEGMENTAL MLC) │
│ • Gantry stops at each angle │
│ • MLC shapes change in discrete segments │
│ • Beam on only when MLC is static │
│ │
│ 2. SLIDING WINDOW (DYNAMIC MLC) │
│ • Gantry stops at each angle │
│ • MLC leaves move continuously while beam is on │
│ • More efficient than step-and-shoot │
│ │
│ 3. VOLUMETRIC MODULATED ARC THERAPY (VMAT) │
│ • Gantry rotates CONTINUOUSLY while beam is on │
│ • MLC shapes change continuously during rotation │
│ • Faster delivery (< 2 min vs 15-20 min for IMRT) │
│ • Better dose homogeneity │
│ │
│ 4. TOMOTHERAPY (HELICAL IMRT) │
│ • Patient moves through bore like CT scanner │
│ • Helical delivery of modulated beam │
│ • Built-in CT for daily IGRT │
└───────────────────────────────────────────────────────────────────────────┘
Scott-Brown's: "Intensity modulation is delivered using a step and shoot technique or more recently, with dynamic arc therapy, either volumetric modulated arc therapy (VMAT) or tomotherapy."
6. IMRT PLANNING: FLOWCHART
┌─────────────────────────────────────────────────────────────────────────┐
│ COMPLETE IMRT PLANNING FLOWCHART │
│ │
│ STEP 1: PATIENT WORKUP │
│ ↓ │
│ • Clinical examination, endoscopy, biopsy │
│ • MRI/CT/PET-CT staging │
│ • MDT discussion (Surgeon + Radiation Oncologist + Radiologist) │
│ ↓ │
│ STEP 2: SIMULATION / IMMOBILIZATION │
│ ↓ │
│ • Custom thermoplastic head-neck-shoulder shell (5-point fixation) │
│ • Dental assessment / fluoride tray │
│ • CT simulation scan (3 mm slices, +/- IV contrast) │
│ • MRI fusion (for skull base, nasopharynx tumors) │
│ ↓ │
│ STEP 3: TARGET VOLUME DELINEATION │
│ ↓ │
│ GTV (Gross Tumor Volume) - visible tumor on imaging │
│ CTV1 (High Risk CTV) = GTV + margin for microscopic spread (5-10 mm) │
│ CTV2 (Elective CTV) = Regional lymphatics at risk │
│ PTV = CTV + setup margin (3-5 mm) │
│ ↓ │
│ STEP 4: ORGANS AT RISK (OAR) DELINEATION │
│ ↓ │
│ • Spinal cord (max < 45 Gy) │
│ • Brainstem (max < 54 Gy) │
│ • Parotid glands (mean < 26 Gy, contralateral < 24 Gy) │
│ • Mandible, cochlea, optic nerves/chiasm, retina │
│ • Larynx/pharyngeal constrictors (swallowing) │
│ ↓ │
│ STEP 5: INVERSE PLANNING (TPS) │
│ ↓ │
│ • Dose prescription entered │
│ • Beam angles selected (7-9 beams or arcs) │
│ • Optimization algorithm runs iteratively │
│ • Dose-Volume Histogram (DVH) reviewed │
│ ↓ │
│ STEP 6: PLAN EVALUATION & QA │
│ ↓ │
│ • DVH analysis - meets planning goals? │
│ • IMRT QA phantom measurement │
│ • Medical physicist sign-off │
│ ↓ │
│ STEP 7: TREATMENT DELIVERY │
│ ↓ │
│ • IGRT verification (cone-beam CT daily) │
│ • Treatment 5 days/week × 6-7 weeks │
│ • Weekly on-treatment review │
│ ↓ │
│ STEP 8: FOLLOW-UP │
│ • 6-8 weeks post-RT: clinical review, PET-CT if indicated │
└─────────────────────────────────────────────────────────────────────────┘
7. TARGET VOLUME DEFINITIONS
| Volume | Definition | Dose (Typical) |
|---|---|---|
| GTV (Gross Tumor Volume) | Macroscopic tumor visible on imaging/examination | - |
| CTV1 (High Risk) | GTV + 5-10 mm for microscopic disease, involved nodes | 66-70 Gy |
| CTV2 (Intermediate Risk) | Adjacent at-risk tissue, close nodes | 60-63 Gy |
| CTV3 (Elective/Low Risk) | Regional lymph node levels at risk | 54-56 Gy |
| PTV | CTV + 3-5 mm setup margin | - |
| OAR | Organs at risk to be protected | Max dose specified |
8. IMRT DOSE DISTRIBUTION DIAGRAM (from Scott-Brown's)
The following image shows an actual IMRT plan on axial CT - note how the isodose lines conform tightly to the target (tonsillar carcinoma) while sparing the contralateral parotid:
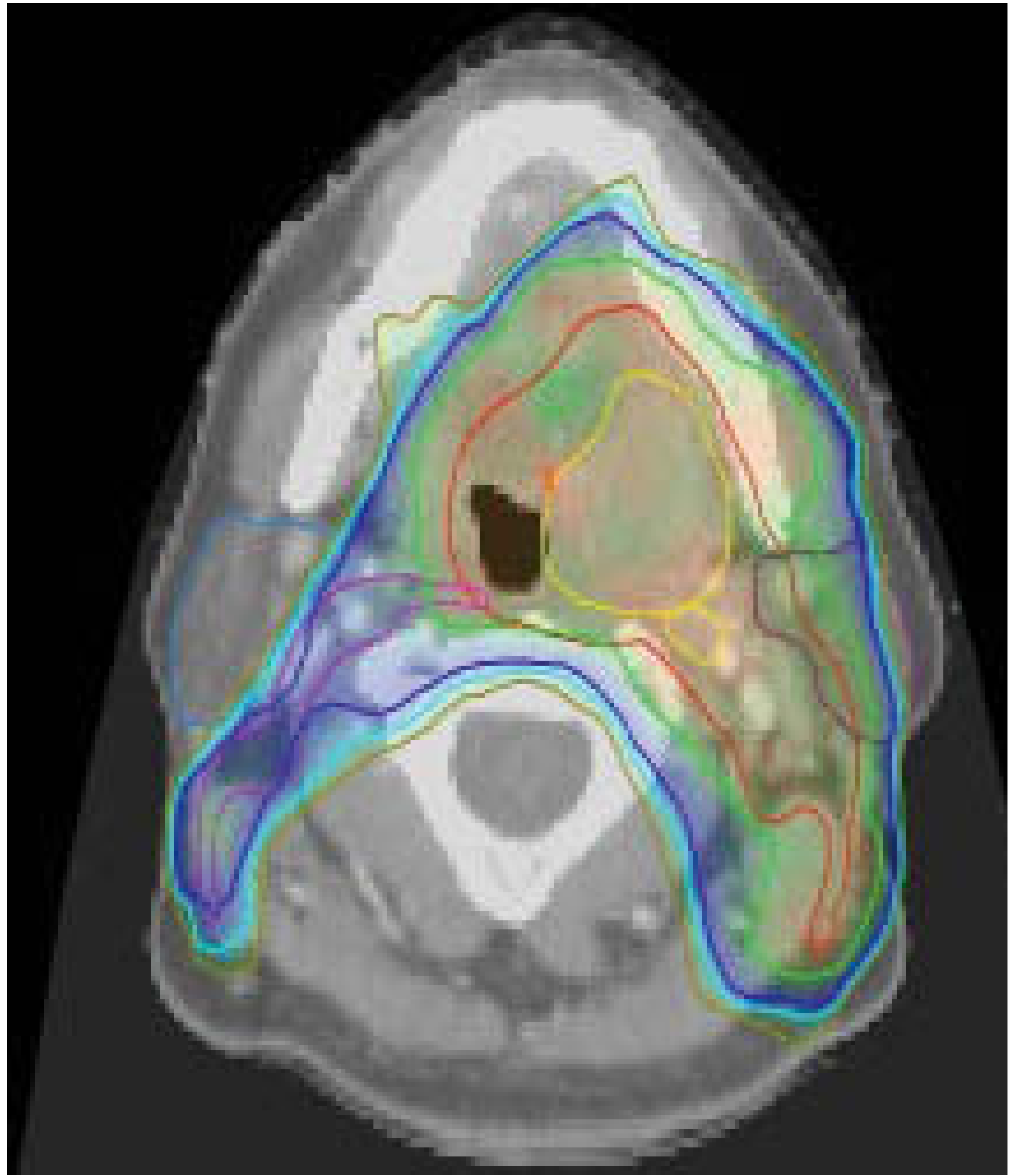
Figure: IMRT plan for left tonsillar carcinoma. GTV (yellow), CTV1 radical dose (red), CTV2 prophylactic (purple). Isodose lines at 62.7 Gy (green), 51.3 Gy (blue) and 48 Gy (mustard). - Scott-Brown's Otorhinolaryngology
9. MULTI-BEAM IMRT ARRANGEMENT (from Cummings)
The following image shows 3D IMRT beam arrangement - multiple green MLC-shaped fields converge on the red target (oropharyngeal primary) while avoiding critical structures including the eyes:
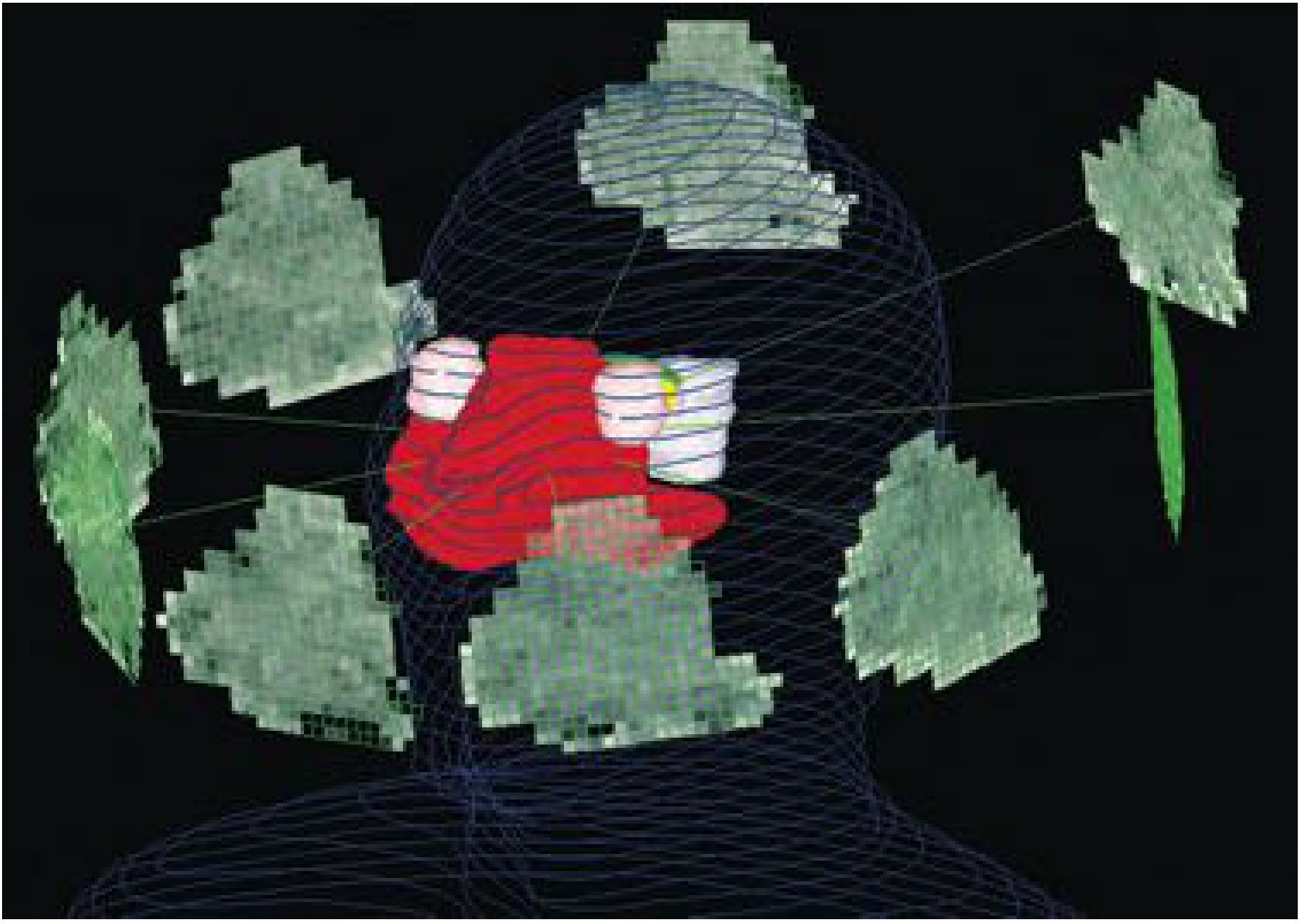
Figure: IMRT of head and neck cancer. Each green field represents a radiation field shaped by the MLC. The red structure is the target. Eyes are avoided. - Cummings Otolaryngology, Fig. 75.11
10. DOSE FRACTIONATION SCHEDULES IN IMRT
Standard Fractionation:
- 2 Gy/fraction, 5 days/week, 35 fractions = 70 Gy total (7 weeks)
Simultaneous Integrated Boost (SIB) - MOST USED IN IMRT:
┌──────────────────────────────────────────────────────────────────┐
│ SIMULTANEOUS INTEGRATED BOOST (SIB) TECHNIQUE │
│ │
│ SINGLE TREATMENT SESSION delivers: │
│ • High-dose boost: GTV → 66-70 Gy in 30-33 fx (2.12-2.2 Gy/fx)│
│ • Intermediate dose: CTV1 → 60 Gy in 30 fx (2.0 Gy/fx) │
│ • Elective dose: CTV2 → 54 Gy in 30 fx (1.8 Gy/fx) │
│ │
│ ADVANTAGE: All doses in SAME number of fractions │
│ No sequential boost needed │
│ Radiobiologically advantageous │
└──────────────────────────────────────────────────────────────────┘
Common IMRT Regimens in HNC:
| Regimen | Dose | Fractions | Indication |
|---|---|---|---|
| Conventional SIB | 66-70/54-56 Gy | 30-33 fx | Most HNC |
| PARSPORT | 65/54 Gy | 30 fx | Parotid-sparing |
| Hypofractionated | 55 Gy | 20 fx | Palliative |
| Hyperfractionated | 1.2 Gy BD | 68.4 Gy total | Selected T3-T4 |
11. INDICATIONS FOR IMRT IN ENT (Head and Neck)
┌──────────────────────────────────────────────────────────────────┐
│ INDICATIONS FOR IMRT IN ENT TUMORS │
│ │
│ DEFINITIVE (PRIMARY) IMRT: │
│ 1. Nasopharyngeal carcinoma (ALL stages) - PRIMARY INDICATION │
│ 2. Oropharyngeal carcinoma (tonsillar, BOT, soft palate) │
│ 3. Hypopharyngeal carcinoma (larynx-preservation protocol) │
│ 4. Laryngeal cancer (T3-T4, organ preservation) │
│ 5. Paranasal sinus malignancies (near optic pathways) │
│ 6. Salivary gland tumors (near brainstem/cochlea) │
│ 7. Unknown primary with neck nodes (bilateral neck RT) │
│ │
│ POSTOPERATIVE (ADJUVANT) IMRT: │
│ 8. Post-op HNC with close/positive margins │
│ 9. ECE (extracapsular extension) in neck nodes │
│ 10. Recurrent tumors (re-irradiation) │
│ │
│ LEAST BENEFIT (conventional RT may suffice): │
│ • T1-T2 N0 larynx (small field, away from OAR) │
│ • Ipsilateral neck only │
└──────────────────────────────────────────────────────────────────┘
Cummings, Ch. 75: "Those who would benefit most are patients with paranasal sinus cancer near the optic pathways, oropharyngeal or nasopharyngeal cancer in whom standard fields would encompass most salivary glands, and patients where the tumor dose would be compromised because of proximity to the spinal cord or brainstem."
12. ORGANS AT RISK (OAR) DOSE CONSTRAINTS
| Organ at Risk | Constraint | Clinical Effect if Exceeded |
|---|---|---|
| Spinal cord | Max < 45 Gy | Radiation myelopathy |
| Brainstem | Max < 54 Gy | Brainstem necrosis |
| Parotid gland | Mean < 26 Gy | Xerostomia |
| Contralateral parotid | Mean < 24 Gy | Severe xerostomia |
| Mandible | Max < 70 Gy | Osteoradionecrosis |
| Cochlea | Mean < 35 Gy | Sensorineural hearing loss |
| Optic chiasm | Max < 54 Gy | Visual loss |
| Retina | Max < 45 Gy | Radiation retinopathy |
| Larynx | Mean < 45 Gy | Dysphagia, aspiration |
| Pharyngeal constrictors | Mean < 50 Gy | Dysphagia |
13. ADVANTAGES OF IMRT OVER CONVENTIONAL RT
┌───────────────────────────────────────────────────────────────────────┐
│ IMRT vs CONVENTIONAL RT - COMPARISON │
│ │
│ PARAMETER CONVENTIONAL RT IMRT │
│ ─────────────────────────────────────────────────────────────────── │
│ Dose distribution Rectangular fields Conformal, sculpted │
│ Tumor dose Limited by OAR Higher doses possible │
│ Salivary glands Both parotids irradiated One/both can be spared │
│ Xerostomia Severe (83%) Reduced (29%) │
│ Posterior neck Electron supplement Integrated in plan │
│ Dose homogeneity Less uniform Superior │
│ Dosimetry Forward planning Inverse (computer) │
│ Beams 2-4 fields 7-9 fields / arcs │
│ Treatment time 10-15 min 15-30 min (IMRT) │
│ <5 min (VMAT) │
│ QA requirement Standard Extensive │
│ Cost Lower Higher │
└───────────────────────────────────────────────────────────────────────┘
The PARSPORT Trial (Phase III UK RCT): Parotid-sparing IMRT reduced grade 3-4 xerostomia from 83% to 29% at 24 months (p=0.0001). (Scott-Brown's, block3)
14. IMRT IN SPECIFIC ENT SITES
A. NASOPHARYNGEAL CARCINOMA (NPC)
- IMRT is the gold standard for NPC - most ideal indication
- Tumors adjacent to brainstem, temporal lobes, cochlea, optic pathways
- Standard dose: 70 Gy to GTV, 60 Gy to CTV, 54 Gy elective nodes
- Concurrent cisplatin-based chemoradiation for Stage II-IVB
- IMRT reduced xerostomia and improved QoL vs 2D-RT in randomized trial (Kam et al.)
B. OROPHARYNGEAL CARCINOMA
- SIB-IMRT is standard of care (Scott-Brown's block3)
- Lateralized tumors: ipsilateral parotid-sparing possible
- HPV+ tumors: de-escalation trials ongoing (PATHOS, ADEPT)
- Concurrent cisplatin (100 mg/m² 3-weekly or 40 mg/m² weekly)
C. LARYNGEAL/HYPOPHARYNGEAL CANCERS
- Organ preservation protocols
- T3 larynx: IMRT + concurrent chemo avoids laryngectomy
- Key OARs: larynx, pharyngeal constrictors (swallowing preservation)
D. PARANASAL SINUS TUMORS
- Targets close to optic nerves, chiasm, brain
- IMRT allows dose escalation while sparing vision
- Post-op IMRT for close/positive margins
E. SALIVARY GLAND TUMORS
- Cummings, block17: IMRT use increased from 16.9% (2004) to 56.3% (2012)
- Allows curative dose near brainstem/cochlea
- Grade 3 mucositis in 14%, no Grade 4-5 toxicities (Schoenfeld series)
15. TOXICITIES OF IMRT
Acute (During/Within 3 months):
- Mucositis (Grade 3: 14-30%)
- Dysphagia, odynophagia
- Xerostomia (less severe than conventional RT)
- Skin erythema / moist desquamation
- Fatigue, weight loss
- Hoarseness (laryngeal edema)
Late (>3 months post-RT):
- Xerostomia - significantly reduced with parotid-sparing IMRT
- Dysphagia / aspiration (pharyngeal constrictor fibrosis)
- Hypothyroidism (30-50%)
- Trismus (TMJ fibrosis)
- Osteoradionecrosis of mandible
- Sensorineural hearing loss (cochlear dose)
- Lymphedema
- Secondary malignancy (increased integral dose)
16. IMAGE-GUIDED RADIOTHERAPY (IGRT) - COMPLEMENT TO IMRT
┌──────────────────────────────────────────────────────────────────────┐
│ IGRT INTEGRATED WITH IMRT │
│ │
│ Pre-treatment daily imaging: │
│ • Cone-beam CT (CBCT) on LINAC │
│ • kV/MV orthogonal X-rays │
│ ↓ │
│ Compare to planning CT → calculate shift required │
│ ↓ │
│ Correct patient position before each fraction │
│ │
│ BENEFITS: │
│ • Reduces setup error (accounts for tumor shrinkage, weight loss) │
│ • Reduces PTV margins → less normal tissue irradiated │
│ • Detects anatomic changes requiring plan adaptation │
│ │
│ ADAPTIVE IMRT (ART): │
│ • CT rescan mid-treatment (week 3-4) │
│ • Replanning if significant anatomic change │
└──────────────────────────────────────────────────────────────────────┘
K.J. Lee's: "IGRT improves the likelihood that treatment is delivered accurately and thus reduces the risk of 'marginal miss.' IGRT can reduce the margin of normal tissue used to account for potential setup error."
17. QUALITY ASSURANCE (QA) IN IMRT
- Pre-treatment IMRT QA is mandatory - more complex than conventional RT
- Phantom measurements using ionization chambers and film dosimetry
- Gamma analysis (3%/3mm criteria - >95% pass rate required)
- MLC leaf calibration and position verification
- Dosimetric verification before each new plan
18. ADVANTAGES AND DISADVANTAGES SUMMARY
Advantages:
- Superior dose conformality - tumors of complex irregular shape
- Simultaneous treatment of multiple dose levels (SIB)
- Reduced xerostomia (parotid sparing)
- Spares spinal cord, brainstem, optic pathways
- Eliminates posterior electron neck boost
- Better quality of life outcomes
- Improved locoregional control (dose escalation possible)
Disadvantages / Limitations:
- Risk of marginal miss - if target not accurately delineated
- Higher integral dose to normal tissue (low-dose bath) - risk of secondary cancers
- Longer planning time - requires experienced MDT
- Extensive QA required
- Higher cost
- Not beneficial for all patients (small field larynx cases)
- Anatomic changes during treatment (weight loss, tumor shrinkage) - need adaptive RT
19. RECENT ADVANCES (2023-2026)
Based on PubMed literature (PMID 37803477, 38116957, 38843843, 39614391):
┌──────────────────────────────────────────────────────────────────────────┐
│ RECENT ADVANCES IN IMRT (2023-2026) │
│ │
│ 1. VMAT (Volumetric Modulated Arc Therapy) │
│ • Now preferred over static-field IMRT at most centers │
│ • Faster delivery, comparable or better dosimetry │
│ │
│ 2. MRI-LINAC (MR-guided RT) │
│ • Real-time soft tissue imaging during treatment │
│ • Adapt plan DURING fraction (online adaptive RT) │
│ │
│ 3. ADAPTIVE RADIOTHERAPY (ART) │
│ • Replanning when anatomy changes significantly │
│ • Maintains dose to shrinking tumor, better OAR sparing │
│ │
│ 4. PROTON THERAPY / IMPT │
│ • Intensity-Modulated Proton Therapy │
│ • No exit dose (Bragg peak) - further reduces integral dose │
│ • Trials comparing IMPT vs IMRT for HNC in progress │
│ • Scott-Brown's: "IMPT may be considered in the future for │
│ certain head and neck tumors" │
│ │
│ 5. AI / DEEP LEARNING IN IMRT PLANNING │
│ • Automated contouring (OAR delineation by AI) │
│ • Automated treatment planning (knowledge-based planning) │
│ • Reduces planning time from hours to minutes │
│ │
│ 6. DE-ESCALATION IN HPV+ OROPHARYNGEAL CA │
│ • IMRT dose reduction trials (54 Gy vs 70 Gy) │
│ • Replacing cisplatin with cetuximab (RTOG 1016, De-Escalate) │
│ • Transoral surgery + de-intensified IMRT (PATHOS, ADEPT trials) │
│ │
│ 7. IMRT FOR NPC: GP vs TPF induction + IMRT │
│ • GP regimen (gemcitabine + cisplatin) superior to TPF │
│ • Comparable efficacy with less toxicity (PMID 39271993) │
│ │
│ 8. SPARING SWALLOWING STRUCTURES │
│ • SWOAR Trial: organ-at-risk sparing IMRT for submandibular │
│ glands and swallowing structures │
│ • Reduces dysphagia and aspiration post-RT │
│ │
│ 9. CARBON ION BOOST + IMRT │
│ • Combined IMRT + carbon ion for salivary gland tumors │
│ • Better local control for adenoid cystic carcinoma │
└──────────────────────────────────────────────────────────────────────────┘
20. ROLE OF ENT SURGEON IN IMRT (Multidisciplinary Approach)
Cummings, block26: "Precise target volume delineation is dependent on a thorough physical examination, comprehensive imaging studies such as MRI, and detailed knowledge of routes of tumor spread. Given these factors, target volume delineation should be performed using a multidisciplinary approach involving a radiation oncologist, neuroradiologist, and - in the postoperative setting - head and neck surgeon."
┌──────────────────────────────────────────────────────────────────────┐
│ ROLE OF ENT SURGEON IN IMRT MDT │
│ │
│ PRE-TREATMENT: │
│ • Accurate staging (examination under anesthesia, endoscopy) │
│ • Biopsy and histological diagnosis │
│ • Dental clearance, feeding tube assessment │
│ • Discuss organ-preservation vs surgery with patient │
│ │
│ DURING PLANNING: │
│ • Input to GTV delineation (knowledge of tumor spread patterns) │
│ • Identify at-risk subsites not visible on imaging alone │
│ • Identify post-surgical changes (anatomy distortion) │
│ │
│ DURING TREATMENT: │
│ • Weekly on-treatment reviews │
│ • Manage acute toxicities (mucositis, dysphagia, tracheostomy) │
│ │
│ POST-TREATMENT: │
│ • Clinical assessment for response │
│ • PET-CT interpretation (no earlier than 10-12 weeks post-RT) │
│ • Salvage surgery if residual/recurrent disease │
└──────────────────────────────────────────────────────────────────────┘
QUICK REVISION - KEY POINTS FOR RGUHS EXAM
| Key Fact | Value |
|---|---|
| IMRT approved for H&N cancer | 1999 |
| Key physical principle | Inverse planning + MLC beamlets |
| Key trial for parotid sparing | PARSPORT (UK Phase III RCT) |
| Xerostomia reduction | 83% → 29% (PARSPORT) |
| Parotid mean dose constraint | < 26 Gy (mean) |
| Spinal cord max | < 45 Gy |
| SIB - simultaneous dose levels | 70/63/56 Gy in same # fractions |
| IMRT delivery modes | Step-shoot, Dynamic, VMAT, Tomotherapy |
| Best indication | NPC, oropharyngeal ca, paranasal sinus |
| Main risk | Marginal miss if poor delineation |
| Modern upgrade | VMAT, MRI-LINAC, IMPT (protons) |
REFERENCES
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th Ed. - Ch. 13 (Oropharynx), Ch. 45 (Salivary glands/RT), Ch. Hypopharynx
- Cummings Otolaryngology Head and Neck Surgery, 7th Ed. - Ch. 75 (RT principles), Ch. 88 (Salivary glands), Ch. 121 (Skull base)
- K.J. Lee's Essential Otolaryngology, 11th Ed. - p. 873 (IMRT), p. 873 (IGRT)
- Dhingra's Diseases of Ear, Nose and Throat - RT in H&N tumors
- Hazarika's Textbook of Ear, Nose and Throat - Radiotherapy principles
- Zhang S et al. (2023). Advancements of radiotherapy for recurrent head and neck cancer. Radiat Oncol. [PMID: 37803477]
- Levyn H et al. (2024). Radiation oncology for the rhinologist. Curr Opin Otolaryngol Head Neck Surg. [PMID: 38116957]
- Jiang W et al. (2024). Therapeutic optimization in locoregionally advanced NPC. Cell Rep Med. [PMID: 38843843]
- Hosseini MS et al. (2024). Cancer treatment-related xerostomia. Eur J Med Res. [PMID: 39614391]
- PARSPORT Trial - Nutting CM et al. Lancet Oncol 2011;12:127-136
- Beddok A et al. (2025). Reirradiation: Standards and patient-focused strategies. CA Cancer J Clin. [PMID: 40438993]
RGUHS Exam Tip: IMRT questions commonly appear as 20-mark long essays asking for definition, principle, planning steps, indications, advantages over conventional RT, dose constraints, and recent advances. Diagrams of the MLC, inverse planning flowchart, dose distribution, and SIB fractionation are high-yield. The PARSPORT trial data (xerostomia reduction from 83% to 29%) is a classic exam statistic. Always mention NPC as the primary/best indication.
This is a shared conversation. Sign in to Orris to start your own chat.