Anti hypertensives prescription step by step according to health conditions and Blood pressure of the individual
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertension" AND "antihypertensive" AND "treatment guidelines"
Finding Sources
Searching PubMed
"hypertension" AND "antihypertensive agents"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative sources. Let me compile the full, structured response.
Antihypertensive Prescribing: Step-by-Step Guide
This guide integrates the 2024 ESC Guidelines (PMID: 39210715), the 2025 AHA/ACC Guidelines (PMID: 40811516), and major textbooks including Goodman & Gilman, Goldman-Cecil Medicine, and Comprehensive Clinical Nephrology.
Step 1 - Confirm the Diagnosis and Classify Blood Pressure
Blood pressure should be measured on at least 2 separate occasions before initiating therapy. Use the following classification:
| Category | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Normal | < 120 | and | < 80 |
| Elevated | 120-129 | and | < 80 |
| Stage 1 Hypertension | 130-139 | or | 80-89 |
| Stage 2 Hypertension | ≥ 140 | or | ≥ 90 |
| Hypertensive Crisis | > 180 | and/or | > 120 |
Note: The 2025 AHA/ACC guideline retains the 130/80 mmHg threshold for stage 1 HTN introduced in 2017.
Step 2 - Assess Cardiovascular Risk and Comorbidities
Before prescribing, evaluate for:
- Target organ damage: LVH, CKD, proteinuria, retinopathy
- Compelling comorbidities: diabetes, heart failure, CAD, prior stroke, atrial fibrillation, CKD
- Contraindications to specific drug classes
- Special populations: elderly (≥80 yrs), pregnancy, Black ethnicity
Step 3 - Lifestyle Modifications (All Stages, All Patients)
Lifestyle changes lower systolic BP by 7-15 mmHg and should always accompany drug therapy:
| Intervention | Expected SBP Reduction |
|---|---|
| DASH diet / Mediterranean diet | ~6 mmHg |
| Reduce sodium to < 1500 mg/day | ~5-6 mmHg |
| Aerobic exercise 90-150 min/week | ~4-8 mmHg |
| Weight loss (per 5 kg) | ~4-5 mmHg |
| Alcohol: ≤2 drinks/day (men), ≤1 drink/day (women) | ~3-4 mmHg |
| Quit smoking | Additional CV risk reduction |
"Lifestyle modifications can lower systolic blood pressure by 7 to up to 15 mm Hg and can be tried before embarking on drug therapy." - Goldman-Cecil Medicine
Step 4 - When to Start Drug Therapy
| BP Level | Action |
|---|---|
| Elevated (120-129/< 80) | Lifestyle only; reassess in 3-6 months |
| Stage 1 (130-139/80-89), low CV risk | Lifestyle for 3-6 months; add drug if target not met |
| Stage 1 (130-139/80-89), high CV risk or diabetes | Lifestyle + drug therapy simultaneously |
| Stage 2 (≥ 140/90) | Lifestyle + two-drug therapy simultaneously |
| Stage 2 (≥ 160/100 or ≥ 20/10 above target) | Start with two-drug therapy; consider single-pill combination |
Step 5 - The Four First-Line Drug Classes
Both US (2025 AHA/ACC) and European (2024 ESC) guidelines agree on the same four preferred classes:
| Class | Examples | Key Mechanism |
|---|---|---|
| ACE Inhibitors (ACEi) | Ramipril, Lisinopril, Enalapril | Block angiotensin II production |
| Angiotensin Receptor Blockers (ARBs) | Losartan, Valsartan, Candesartan | Block angiotensin II receptors |
| Calcium Channel Blockers (CCBs) | Amlodipine (DHP); Diltiazem, Verapamil (non-DHP) | Vasodilation / HR reduction |
| Thiazide/Thiazide-like Diuretics | Chlorthalidone (preferred in US), HCTZ, Indapamide | Sodium excretion, volume reduction |
ACEi and ARBs should not be combined with each other (increased risk of renal impairment and hyperkalemia without added BP benefit).
Step 6 - Core Treatment Algorithm (Uncomplicated Hypertension)
This follows the European Core Algorithm (also consistent with 2025 AHA/ACC guidance):
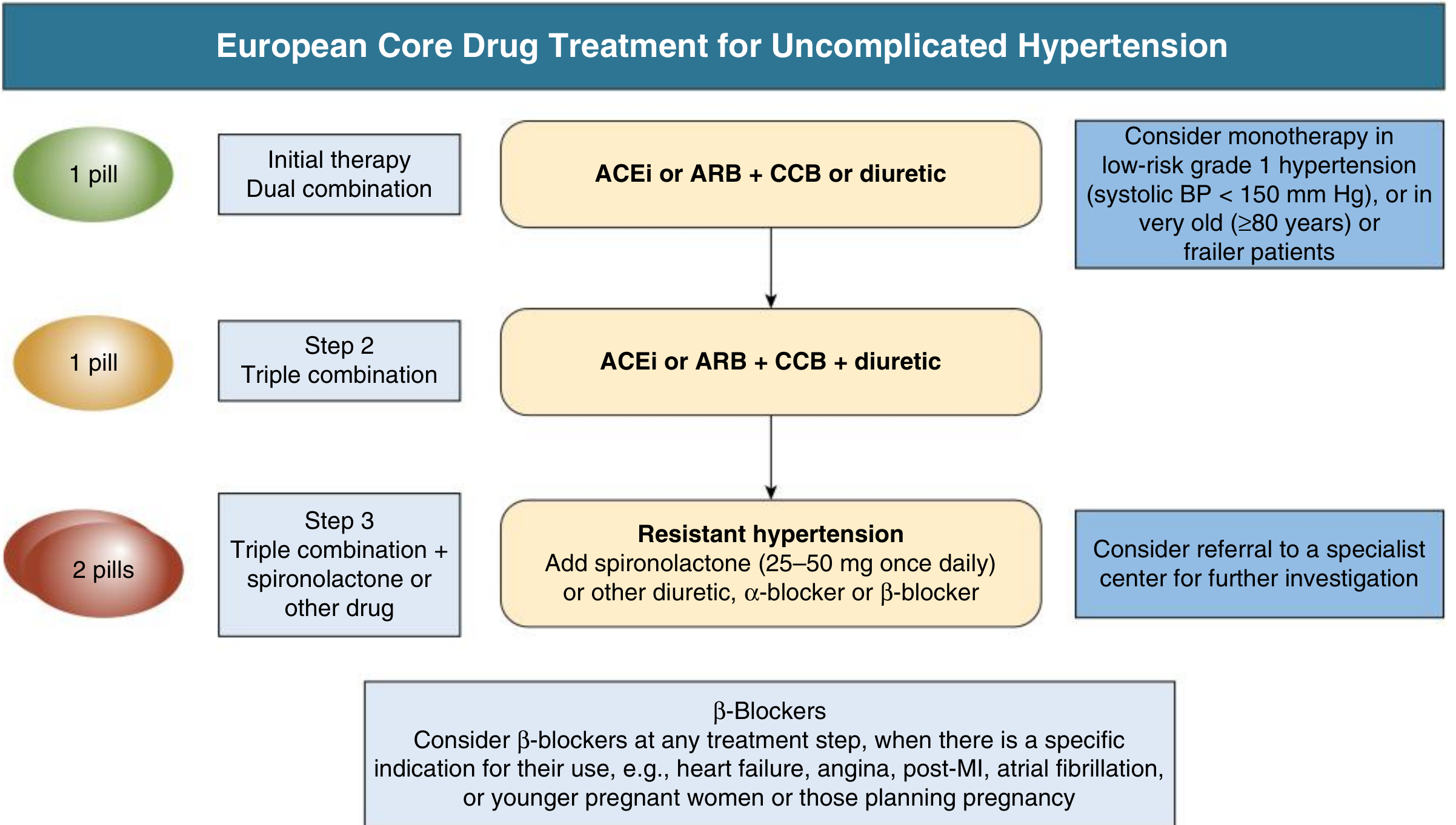
Comprehensive Clinical Nephrology, 7th Ed., Fig. 37.3
Step 6a - Initial Therapy (Step 1 of the algorithm)
- Start with a dual combination: ACEi or ARB + CCB OR ACEi or ARB + thiazide diuretic
- Prefer single-pill combinations for adherence
- Exception: Monotherapy acceptable for - frail elderly (≥80 yrs) or stage 1 HTN with SBP < 150 mmHg
Step 6b - Step 2: Triple Combination
- If BP uncontrolled on dual therapy: ACEi or ARB + CCB + thiazide diuretic
- Again, single-pill triple combination preferred
Step 6c - Step 3: Resistant Hypertension
- BP uncontrolled on maximized triple therapy = Resistant Hypertension
- Add spironolactone 25-50 mg once daily (best evidence - PATHWAY-2 trial)
- Alternatives: doxazosin (alpha-blocker), bisoprolol (beta-blocker), or additional diuretic
- Consider specialist referral and exclude secondary causes
Beta-Blockers
Use beta-blockers at any step when there is a specific indication: heart failure with reduced EF, angina, post-MI, atrial fibrillation, or pregnancy. They are not preferred as routine first-line in uncomplicated HTN.
Step 7 - Drug Selection Based on Comorbidities (Compelling Indications)
This is the most important step for individualized prescribing.
| Comorbidity | Preferred Agent(s) | Avoid |
|---|---|---|
| Diabetes mellitus | ACEi or ARB (especially with proteinuria); CCB, thiazide also acceptable | High-dose thiazides (worsen glucose) |
| Diabetes + proteinuria / microalbuminuria | ACEi or ARB (renoprotective - mandatory) | - |
| CKD with proteinuria (≥1 g/day) | ACEi or ARB first-line | - |
| Heart Failure (HFrEF) | ACEi or ARB, beta-blocker, diuretic, MRA (spironolactone/eplerenone) | Non-DHP CCBs (verapamil, diltiazem) |
| Post-MI / CAD / Angina | ACEi or ARB + beta-blocker; CCB for angina | - |
| Atrial Fibrillation (rate control) | Beta-blocker, non-DHP CCBs (diltiazem, verapamil) | - |
| Atrial Fibrillation (prevention) | ACEi, ARB, beta-blocker | - |
| Prior Stroke | ACEi or ARB + thiazide diuretic | - |
| Left Ventricular Hypertrophy | ACEi, ARB, CCB | - |
| Peripheral Artery Disease | ACEi or ARB, CCB | Beta-blockers (use with caution) |
| Aortic Aneurysm | Beta-blocker | - |
| Isolated Systolic HTN (elderly) | ACEi/ARB, CCB, thiazide | - |
| Metabolic Syndrome | ACEi, ARB, CCB | Thiazides + beta-blockers (worsen insulin resistance) |
| Hyperaldosteronism (Conn's) | Spironolactone (MRA) | - |
| Asymptomatic Atherosclerosis | CCB | - |
| Gout | ACEi, ARB, CCB | Thiazide diuretics (raise uric acid) |
| Asthma / COPD | ACEi, ARB, CCB, thiazide | Beta-blockers (contraindicated in asthma) |
| Black patients | CCB + thiazide diuretic (ACEi/ARBs less effective as monotherapy) | - |
| Bilateral Renal Artery Stenosis | CCB, thiazide | ACEi or ARB (contraindicated) |
Source: Goodman & Gilman's The Pharmacological Basis of Therapeutics, Table 32-4
Step 8 - Pregnancy
All standard first-line agents (ACEi, ARBs) are contraindicated due to teratogenicity.
| Preferred in Pregnancy | Notes |
|---|---|
| Labetalol (alpha + beta-blocker) | First-line for chronic HTN in pregnancy |
| Methyldopa | Long safety record; centrally acting |
| Nifedipine (CCB, long-acting) | Effective for acute and chronic |
| Hydralazine | Used IV for hypertensive emergencies in pregnancy |
"ACE inhibitors and ARBs have been proven to be teratogenic and increase fetal/neonatal adverse outcomes." - Washington Manual of Medical Therapeutics
Step 9 - BP Targets
| Patient Group | Target BP |
|---|---|
| General adults | < 130/80 mmHg (2025 AHA/ACC) |
| General adults (ESC 2024) | < 130/80 mmHg (if tolerated) |
| Elderly ≥ 65 yrs | < 130/80 (if tolerated); SBP 120-130 preferred |
| Very elderly ≥ 80 yrs / frail | SBP 130-149 mmHg; avoid over-treatment |
| Diabetes | < 130/80 mmHg |
| CKD with proteinuria | < 130/80 mmHg |
| Pregnancy | SBP 110-140; DBP 70-90 mmHg |
Step 10 - Key Contraindications Summary
| Drug Class | Absolute Contraindication |
|---|---|
| ACEi | Pregnancy, angioedema, bilateral RAS, hyperkalemia |
| ARB | Pregnancy, bilateral RAS, hyperkalemia |
| Non-DHP CCB (verapamil/diltiazem) | AV block grade 2-3, severe LV dysfunction, HFrEF |
| Thiazide diuretics | Gout |
| Beta-blockers | Asthma, AV block grade 2-3 |
| MRA (spironolactone) | Hyperkalemia, creatinine >2.5 mg/dL (men) or >2.0 mg/dL (women) |
Source: Goodman & Gilman, Table 32-5
Quick Reference Summary
Lifestyle always first →
↓
Stage 2 or high risk + Stage 1? → Start drugs
↓
Step 1: ACEi/ARB + CCB or thiazide (dual combo, single pill if possible)
↓ (if BP not at target)
Step 2: ACEi/ARB + CCB + thiazide (triple combo)
↓ (if still uncontrolled = Resistant HTN)
Step 3: Add spironolactone 25-50 mg/day ± alpha/beta-blocker → Specialist referral
Always adjust for comorbidities (diabetes → ACEi/ARB mandatory;
heart failure → ACEi+BB+MRA; pregnancy → labetalol/methyldopa/nifedipine)
Key 2025 Updates to Note:
- The 2025 AHA/ACC Guideline (PMID: 40811516) was just published (Sep-Oct 2025) and reinforces BP target of < 130/80 mmHg for most adults, and strongly advocates single-pill combination therapy to improve adherence
- The 2024 ESC Guideline (PMID: 39210715) introduced a single-pill strategy and aligns closely with US guidance on preferred drug classes
- Beta-blockers are no longer routine first-line for uncomplicated HTN in either guideline but remain important for specific indications
Sources: Comprehensive Clinical Nephrology 7th Ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics | Goldman-Cecil Medicine | Washington Manual of Medical Therapeutics | Harrison's 22E | 2024 ESC Guidelines (PMID: 39210715) | 2025 AHA/ACC Guidelines (PMID: 40811516)
This is a shared conversation. Sign in to Orris to start your own chat.