Acute pancreatitis
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Searching PubMed
"acute pancreatitis"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced information to deliver a thorough answer. Here is the full clinical overview of acute pancreatitis:
Acute Pancreatitis
Definition & Epidemiology
Acute pancreatitis (AP) is a sudden inflammatory disease of the pancreas caused by enzymatic autodigestion of pancreatic tissue. It is the most common pancreatic disease worldwide and one of the leading reasons for GI-related hospitalization in the United States. While overall mortality has decreased despite rising hospital admissions, mortality in severe cases can reach 30%, and exceeds 36-50% when infected necrosis develops. - Rosen's Emergency Medicine, p. 1265
Etiology
The two dominant causes account for the vast majority of cases:
- Gallstones: 40-70%
- Chronic alcohol use: 25-35%
Other recognized causes include:
| Category | Examples |
|---|---|
| Toxic-Metabolic | Alcohol, hypertriglyceridemia (TG >1000 mg/dL), hypercalcemia, uremia, drugs, scorpion venom |
| Mechanical-Obstructive | Biliary stones, post-ERCP, pancreas divisum, annular pancreas, ampullary tumors, trauma, duodenal diverticulum |
| Infectious | Viral: mumps, coxsackievirus, HIV, CMV, EBV, varicella; Bacterial: TB, Salmonella, Mycoplasma; Parasitic: Ascaris |
| Autoimmune | IgG4-related (Type 1), Type 2 |
| Vascular | Ischemia, vasculitis |
| Idiopathic | Many may be occult microlithiasis |
Smoking and diabetes are independent risk factors. - Rosen's Emergency Medicine, p. 1265-1266
Pathophysiology
The central mechanism is premature activation of digestive enzymes within the pancreatic acinar cells, particularly trypsinogen being activated to trypsin. This triggers a cascade:
- Autodigestion of acinar cells and surrounding tissue
- Release of inflammatory mediators (cytokines, phospholipase A2, elastase)
- Local inflammation → increased microvascular permeability → third-spacing of fluid
- Systemic inflammatory response (SIRS) → potential multiorgan failure
Pulmonary complications arise from increased microvascular permeability and enzymatic degradation of surfactant, leading to ARDS. Cardiovascular collapse results from fluid shifts and third-spacing. Renal failure results from hypoperfusion combined with inflammatory mediator injury. Coagulopathy can progress to DIC. - Rosen's Emergency Medicine, p. 1266
Classification (2012 Revised Atlanta Classification)
| Grade | Organ Failure | Local/Systemic Complications | Mortality Risk |
|---|---|---|---|
| Mild | Absent | Absent | Very rare (<5%) |
| Moderately Severe | Transient (<48 hours) | Present, without persistent organ failure | Low |
| Severe | Persistent (>48 hours) | Present | High (36-50%); extremely high with infected necrosis |
Moderately severe AP accounts for ~15% of cases. Severe AP accounts for ~5%. Severity grade continues to evolve and should be reassessed at 24 hours, 48 hours, 7 days, and weekly thereafter. - Sleisenger & Fordtran's (Management of Pancreatic Necrosis chapter), p. 604
Morphological types:
- Interstitial edematous pancreatitis: Diffuse enlargement with edema, no necrosis - the majority (~90-95%)
- Necrotizing pancreatitis: ~5-10% of patients; involves parenchymal and/or peripancreatic necrosis; increased morbidity when infected
Clinical Features
Symptoms:
- Persistent epigastric or LUQ pain radiating to the back, chest, or flanks
- Pain severity does not correlate with clinical severity
- Nausea, vomiting, anorexia; oral intake worsens pain
- Pain may be relieved by sitting forward or leaning forward
Signs:
-
Vital signs may be normal in mild/early disease
-
Tachycardia, fever, tachypnea with progressive disease
-
Jaundice suggests biliary obstruction
-
Epigastric tenderness ± guarding
-
Cullen sign (periumbilical bluish discoloration) and Grey Turner sign (flank reddish-brown discoloration) indicate retroperitoneal hemorrhage - rare, neither sensitive nor specific, but suggest poor prognosis
-
Diminished bowel sounds if ileus is present
-
Pleural effusions in up to 50% of patients - more commonly left-sided
-
Rosen's Emergency Medicine, p. 1265-1266
Diagnosis
Requires at least 2 of 3 criteria:
- Abdominal pain characteristic of AP
- Serum lipase or amylase >3× upper limit of normal
- Characteristic findings on abdominal imaging
Biochemical Tests
| Test | Notes |
|---|---|
| Lipase | More sensitive AND specific than amylase; peaks rapidly, remains elevated ~1-2 weeks; preferred |
| Amylase | Less specific; elevated in many non-pancreatic conditions; may be falsely negative in alcohol- or hypertriglyceridemia-induced AP; remains elevated ~3-5 days |
| ALT | PPV ~95% for biliary pancreatitis if elevated |
| Bilirubin, AST | Evaluate for biliary obstruction |
| Calcium, TG | Rule out metabolic causes |
| CBC, BMP | Assess for SIRS, organ failure |
| Hematocrit | Elevated = hemoconcentration = risk of necrosis |
| BUN | Elevated BUN = poorer outcomes |
| CRP, Procalcitonin | Useful severity markers; CRP more useful at 24-48 hours |
- Testing both lipase AND amylase does not improve diagnostic sensitivity or specificity
- Degree of enzyme elevation does NOT correlate with severity
Imaging
Abdominal ultrasound - First-line; NOT for direct pancreas diagnosis (often obscured by bowel gas), but used to identify gallstones and biliary dilation as etiology.
CT with IV contrast - NOT routinely needed for diagnosis. Indicated when:
- Diagnostic uncertainty or normal enzyme levels with high clinical suspicion
- Need to exclude other serious pathology (e.g., aortic aneurysm, bowel obstruction)
- Failure to improve after 48-72 hours of appropriate therapy
CT sensitivity/specificity >90% for AP. Pancreatic necrosis appears as areas of non-enhancement. CT is most useful for complications when done 3-7 days after presentation (necrosis not always apparent early).
MRI/MRCP - Superior for gallbladder and biliary tract assessment; useful when CT contrast is contraindicated.
- Rosen's Emergency Medicine, p. 1267
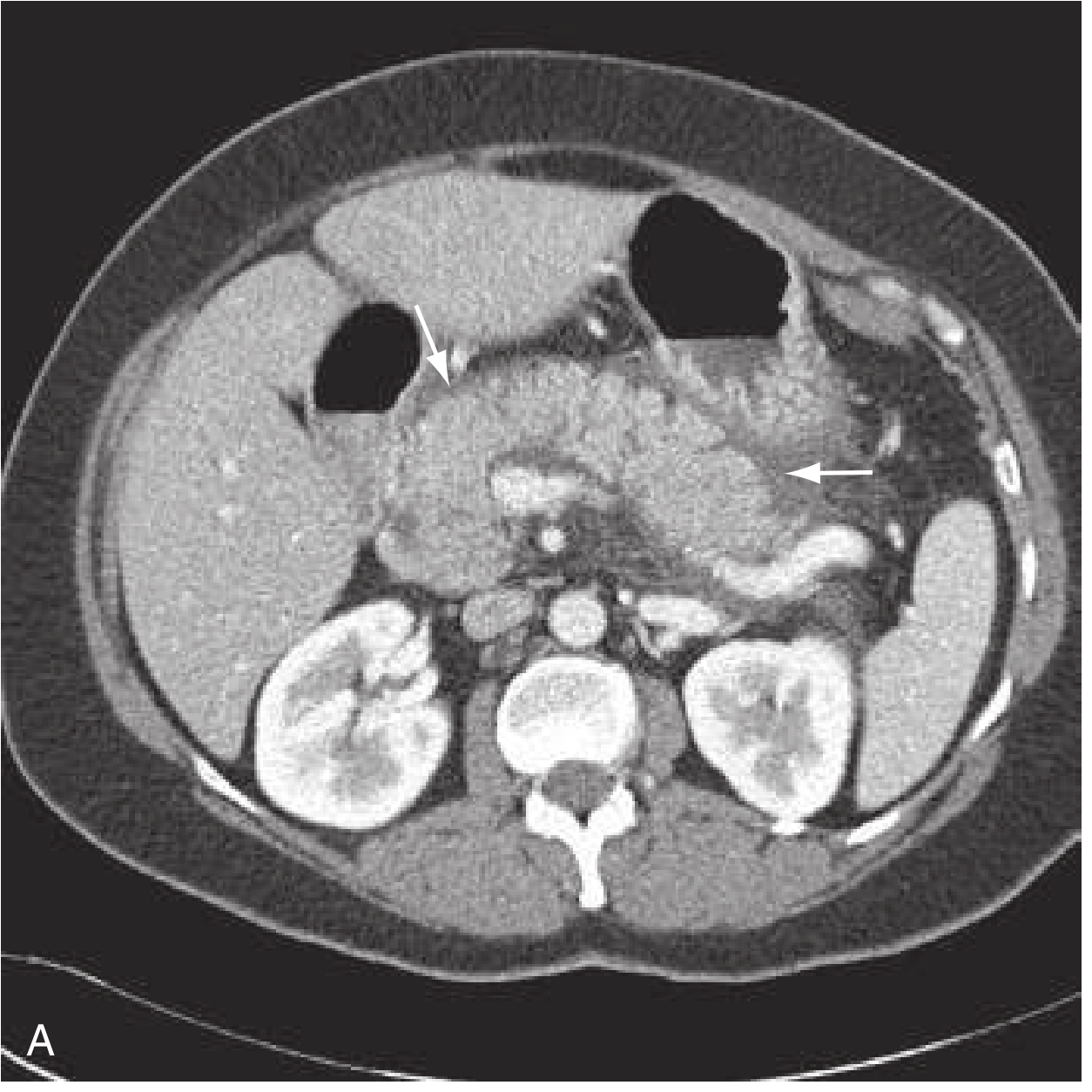
CT Imaging: Interstitial Edematous Pancreatitis
The arrows in this axial CT scan demonstrate peripancreatic fat stranding and mild fluid collection in interstitial edematous pancreatitis:
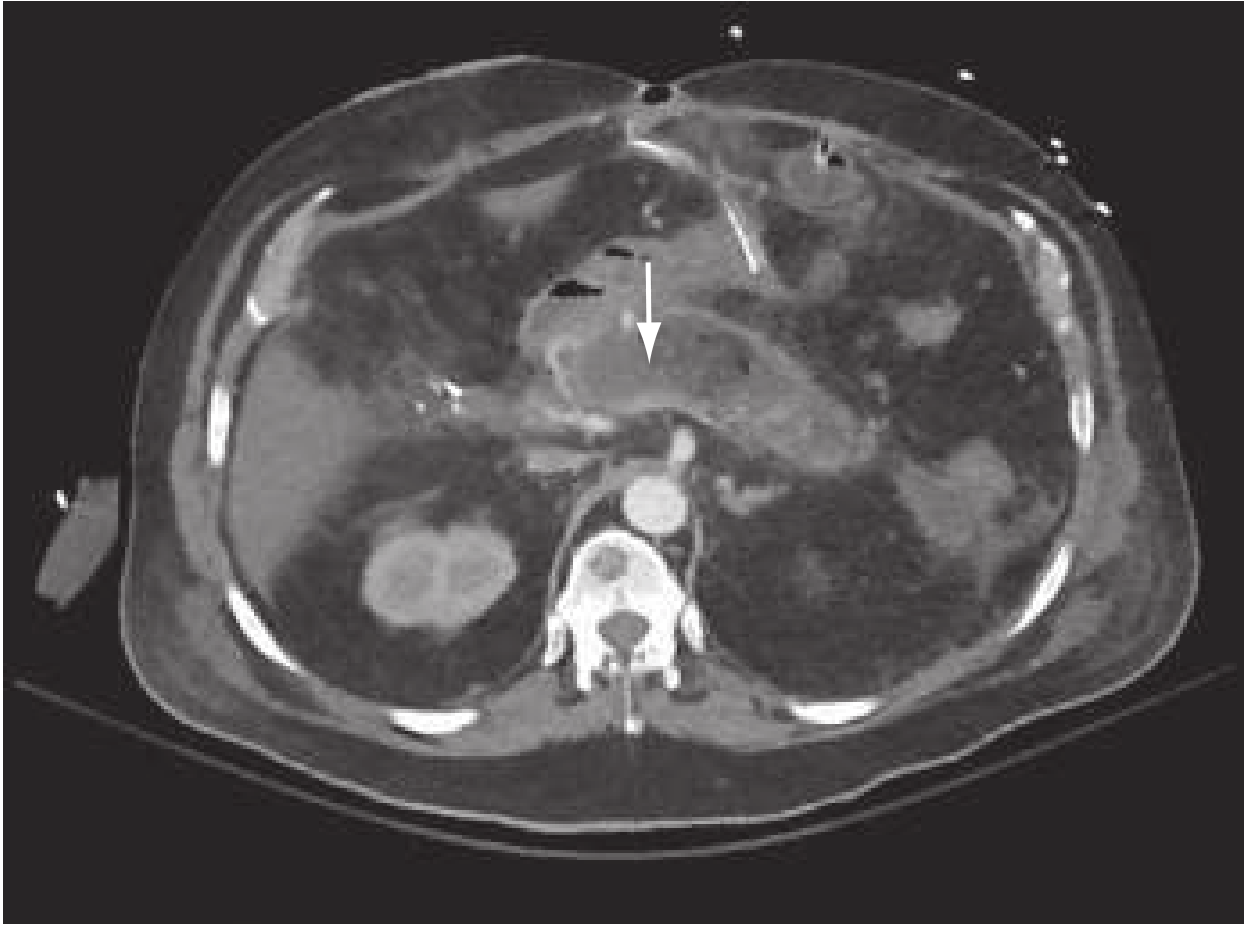
CT Imaging: Necrotizing Pancreatitis
The arrow in this CT points to an area of non-enhancement (decreased or absent contrast uptake) in the pancreatic parenchyma, indicating necrosis:
Severity Scoring Systems
| Score | Factors | Notes |
|---|---|---|
| BISAP | BUN, Impaired mental status, SIRS, Age >60, Pleural effusion | Most useful in ED - can be calculated on admission |
| Ranson's Criteria | 11 factors at admission and 48 hours | Complex; relies on 48h post-admission data |
| APACHE II | Multiple physiologic parameters | Requires ICU-type data; complex |
| HAPS | Peritonitis, creatinine, hematocrit | 97% specific for mild disease; identifies low-risk patients for early discharge |
| CT Severity Index (CTSI) | Degree of necrosis, inflammation, fluid collections on CT | Radiologic severity assessment |
| PASS | Continuous additive scoring including organ failure, SIRS, pain, diet tolerance | Dynamic, monitors severity throughout course |
These scoring systems have similar predictive accuracy - each has different strengths and weaknesses. - Rosen's Emergency Medicine, p. 1268
Local Complications
In Interstitial Edematous Pancreatitis:
- Acute peripancreatic fluid collection (APFC): Homogeneous fluid adjacent to pancreas, <4 weeks from onset; most resolve spontaneously
- Pancreatic pseudocyst: Encapsulated fluid collection with well-defined wall, >4 weeks from onset; contains no significant solid debris; forms from ductal leak
In Necrotizing Pancreatitis:
- Acute necrotic collection (ANC): Heterogeneous fluid + necrosis, <4 weeks
- Walled-off necrosis (WON): Heterogeneous fluid + necrosis with well-defined wall, >4 weeks; sterile or infected
(Atlanta Classification 2012, adapted from Banks PA et al., Gut 2013)
Vascular Complications:
- Splenic or portal vein thrombosis
- Pseudoaneurysm (splenic, hepatic, gastroduodenal arteries)
- GI bleeding, gastric outlet obstruction
Management
1. Fluid Resuscitation (Most Important Early Intervention)
Patients are volume-depleted from decreased oral intake, emesis, and third-spacing. Both inadequate AND excessive resuscitation are harmful.
- IAP/APA goal-directed approach: 5-10 mL/kg/h, targeting:
- HR <120/min
- MAP 65-85 mmHg
- Urine output >0.5-1 mL/kg/h
- ACG recommendation: 250-500 mL/h initially
- Preferred fluid: Lactated Ringer's (LR) over normal saline - LR is thought to provide anti-inflammatory benefits and avoids the hyperchloremic metabolic acidosis of large-volume NS (acidosis activates trypsinogen, worsening disease)
- Colloids are NOT generally recommended; may be considered if hematocrit <24% or albumin <2 g/dL
- Monitor with hematocrit, BUN, creatinine as surrogates
2. Pain Management
- IV opioids for moderate-to-severe pain; hydromorphone and morphine are commonly used
- NSAIDs as adjuncts
3. Nutrition
- Mild AP: Early oral feeding tolerated (even with elevated enzymes) - begin when nausea/vomiting controlled
- Severe AP: Early enteral nutrition is preferred over TPN - associated with fewer infectious complications and lower cost
- NG feeding is as effective as nasojejunal feeding; nasojejunal tubes preferred if gastric retention occurs
- NPO is no longer standard for all cases; prolonged fasting provides no benefit
4. Antibiotics
- Prophylactic antibiotics are NOT indicated in AP
- Antibiotics ARE indicated in:
- Confirmed or suspected infected pancreatic necrosis
- Other clear evidence of sepsis/infection
- Concomitant cholangitis
5. ERCP
Indicated ONLY in:
- Concomitant cholangitis
- Confirmed biliary obstruction (elevated bilirubin + clinical evidence)
- NOT indicated routinely in biliary pancreatitis without obstruction
- MRCP and EUS can identify bile duct stones and select patients for ERCP before proceeding
6. Surgery/Intervention for Complications
-
Cholecystectomy: Standard of care for gallstone pancreatitis - laparoscopic cholecystectomy within 3 days in mild biliary pancreatitis improves outcomes and reduces need for ERCP
-
Infected necrosis: Requires drainage/debridement - endoscopic transmural drainage (for WON abutting stomach/duodenum), minimally invasive surgical necrosectomy, or percutaneous drainage
-
Drainage of pseudocysts: When symptomatic, infected, or enlarging; endoscopic ultrasound-guided transmural drainage preferred for those abutting GI wall
-
Rosen's Emergency Medicine, p. 1268-1270; Sleisenger & Fordtran's (Endoscopy section), p. 2783-2787
Differential Diagnosis
- Peptic ulcer disease / perforation
- Acute cholecystitis / cholangitis / choledocholithiasis
- Gastritis / gastroenteritis
- Mesenteric ischemia / bowel obstruction
- Myocardial infarction (inferior MI can mimic epigastric pain with radiation to back)
- Pneumonia
- Aortic dissection/aneurysm
- Ectopic pregnancy
- Diabetic ketoacidosis
- Sickle cell crisis
Summary Table: Key Points
| Feature | Detail |
|---|---|
| Diagnosis | 2 of 3: characteristic pain, enzymes >3× ULN, imaging |
| Preferred enzyme | Lipase (more specific and sensitive than amylase) |
| Enzyme level vs. severity | No correlation |
| ALT >150 in AP | Strong predictor of biliary etiology (PPV 95%) |
| First-line imaging | Abdominal ultrasound (for biliary etiology) |
| CT indication | Diagnostic uncertainty, other pathology, or complications at 48-72h |
| Fluid of choice | Lactated Ringer's |
| Prophylactic antibiotics | Not indicated |
| Enteral vs. parenteral nutrition | Enteral preferred in severe AP |
| ERCP indication | Cholangitis or confirmed biliary obstruction only |
| Cholecystectomy timing (mild biliary AP) | Within 3 days |
Sources: Rosen's Emergency Medicine: Concepts and Clinical Practice, 9e | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Clinical Gastrointestinal Endoscopy, 3e
This is a shared conversation. Sign in to Orris to start your own chat.