Copd harrison
Reading File
Finding Sources
Searching PubMed
"COPD" AND "management"
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the key content from Harrison's COPD chapter. Let me compile the comprehensive response.
COPD - Harrison's Principles of Internal Medicine (22nd Ed., 2025)
Chapter 303 | Authors: Craig P. Hersh, Edwin K. Silverman, Dawn DeMeo
Definition
COPD is defined as a disease state characterized by persistent respiratory symptoms and airflow obstruction. It encompasses three overlapping entities:
- Emphysema - anatomically defined; destruction of alveoli with air space enlargement
- Chronic bronchitis - clinically defined; chronic cough + phlegm production
- Small airway disease - small bronchioles narrowed and reduced in number
The classic definition requires chronic airflow obstruction on spirometry (post-bronchodilator FEV1/FVC <0.7) usually in the setting of noxious exposures (cigarette smoke, biomass fuels). Increasing prevalence of vaping and inhaled cannabis are of growing concern, especially in adolescents.
COPD is the 4th leading cause of death in the United States, affecting >15 million Americans. Globally, ~480 million individuals are affected, projected to reach 592 million by 2050.
Pathogenesis & Pathology
Large Airway Disease
- Cigarette smoking → mucus gland enlargement + goblet cell hyperplasia → chronic cough/sputum (chronic bronchitis)
- Mucus plugs on CT are associated with increased mortality risk
- Squamous metaplasia - disrupts mucociliary clearance, increases carcinogenesis risk
- Neutrophil elastase is a potent secretagogue (independent of its proteolytic activity)
Small Airway Disease
- Primary site of increased airflow resistance in most COPD patients
- Early COPD is driven by small airway disease - narrowed by cellular hyperplasia, mucus, and fibrosis
- The transition zone (respiratory bronchioles) is critical in early disease
Emphysema
- Alveolar destruction results from an imbalance of proteases and antiproteases, and oxidants and antioxidants
- Cigarette smoke activates macrophages and neutrophils → release of elastase, matrix metalloproteinases
- Alpha-1 antitrypsin (AAT) deficiency is the best-defined genetic risk factor
- Affects ~1-2% of COPD patients; autosomal codominant
- PiZZ genotype: serum AAT levels ~15% of normal
- Should be tested in all COPD patients, especially those with early onset (<45 years), panlobular emphysema, or family history
- Panacinar emphysema - associated with AAT deficiency (lower lobes predominant)
- Centrilobular emphysema - associated with cigarette smoking (upper lobes predominant)
Systemic Effects
COPD has significant systemic manifestations including cachexia, skeletal muscle wasting, osteoporosis, depression, cardiovascular disease, anemia, and increased lung cancer risk.
Diagnosis & Assessment
Spirometry
- Post-bronchodilator FEV1/FVC <0.7 confirms airflow obstruction
- FEV1 % predicted determines GOLD grade severity
GOLD ABE Classification (2024 GOLD Report)
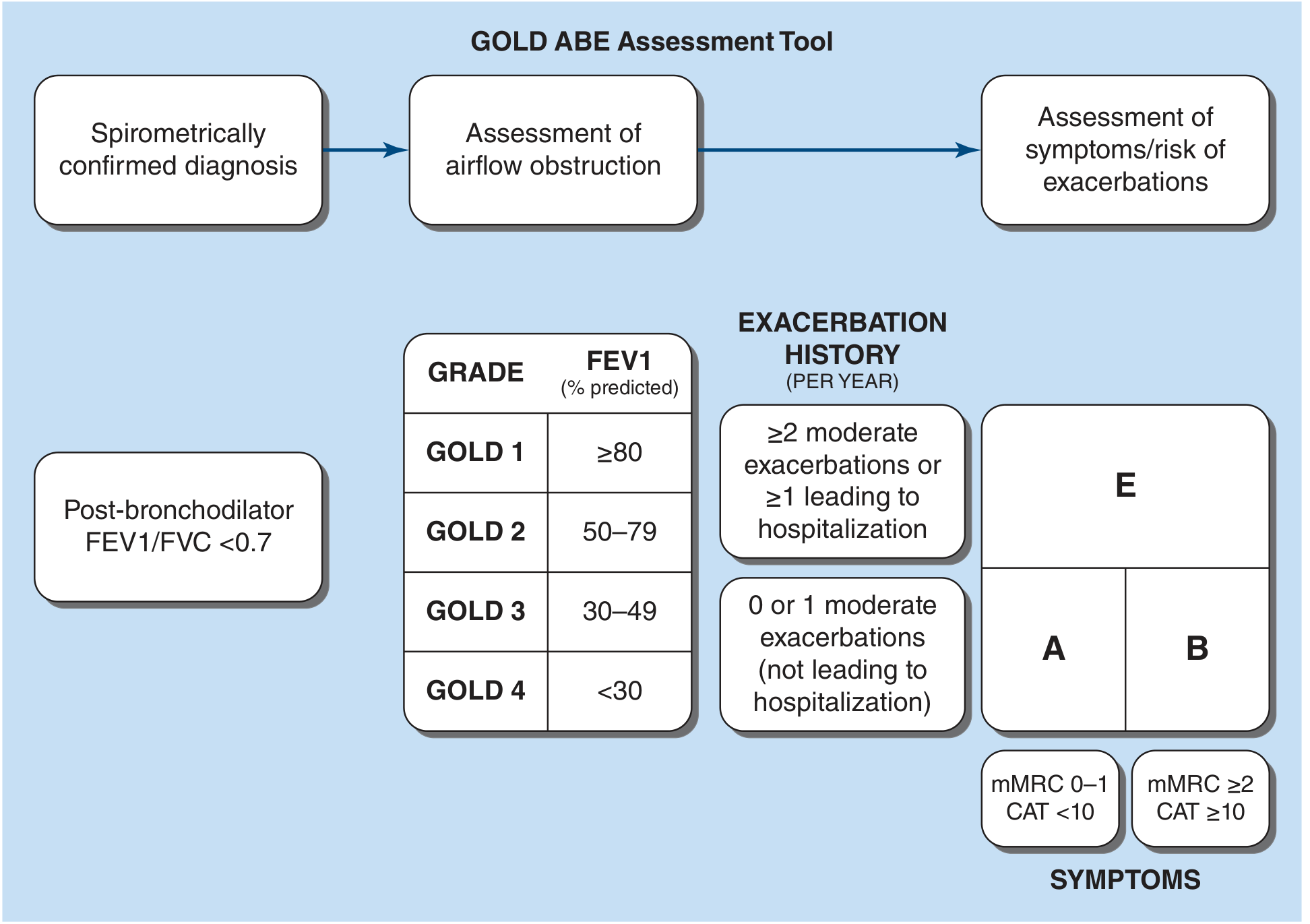
| GOLD Grade | FEV1 % Predicted |
|---|---|
| GOLD 1 (Mild) | ≥80% |
| GOLD 2 (Moderate) | 50-79% |
| GOLD 3 (Severe) | 30-49% |
| GOLD 4 (Very Severe) | <30% |
Symptom/Exacerbation Groups:
- Group A - Few symptoms (mMRC 0-1, CAT <10), low exacerbation risk (0-1 moderate exacerbations not leading to hospitalization)
- Group B - More symptoms (mMRC ≥2, CAT ≥10), low exacerbation risk
- Group E - High exacerbation risk (≥2 moderate exacerbations OR ≥1 hospitalization per year)
Symptom Scoring Tools
- mMRC (Modified Medical Research Council) Dyspnea Scale: 0 (only with strenuous activity) to 4 (too breathless to leave house)
- CAT (COPD Assessment Test): 0-40 scale; ≥10 = more symptoms
Imaging
- Chest X-ray: hyperinflation, flattened diaphragms, increased AP diameter, bullae
- CT chest: best for characterizing emphysema (centrilobular vs. paraseptal vs. panlobular), airway disease, mucus plugging
- CT is superior to spirometry for assessing emphysema distribution and predicting exacerbation risk
Laboratory
- ABG: assess for hypoxemia (PaO2 <55 mmHg) and hypercapnia - guides oxygen therapy
- CBC: polycythemia in chronic hypoxemia
- Alpha-1 antitrypsin level: test all COPD patients at least once
Management
Stable COPD
Non-Pharmacologic (proven mortality benefit)
- Smoking cessation - most impactful intervention; slows FEV1 decline
- Supplemental oxygen (for resting PaO2 ≤55 mmHg, or ≤59 with cor pulmonale/polycythemia) - only non-surgical therapy proven to improve survival
- Lung volume reduction surgery (LVRS) - in selected patients (upper-lobe emphysema + low exercise capacity after rehab)
- Pulmonary rehabilitation - improves dyspnea, exercise tolerance, quality of life; reduces hospitalization
- Vaccinations: influenza (annual), pneumococcal, COVID-19, RSV (recommended)
Pharmacotherapy
Smoking Cessation Pharmacotherapy:
- Nicotine replacement therapy (patch, gum, lozenge, inhaler, nasal spray)
- Bupropion
- Varenicline (nicotinic receptor partial agonist - most effective)
Bronchodilators (mainstay of pharmacologic treatment):
| Drug Class | Examples | Role |
|---|---|---|
| Short-acting muscarinic antagonist (SAMA) | Ipratropium | Acute symptom relief |
| Long-acting muscarinic antagonist (LAMA) | Tiotropium, umeclidinium, glycopyrrolate, aclidinium, revefenacin | Reduces exacerbations more than LABA; dry mouth is main side effect |
| Short-acting beta agonist (SABA) | Albuterol, levalbuterol | As-needed relief |
| Long-acting beta agonist (LABA) | Formoterol, salmeterol, indacaterol, olodaterol, vilanterol, arformoterol | Symptomatic benefit; tremor/tachycardia side effects |
| LABA + LAMA combo | Umeclidinium/vilanterol, tiotropium/olodaterol | Superior to monotherapy |
Inhaled Corticosteroids (ICS):
- NOT recommended as monotherapy in COPD
- Triple therapy (LABA + LAMA + ICS) - reduces mortality in selected patients, particularly those with:
- Blood eosinophil count ≥300 cells/μL
- History of asthma-COPD overlap
- Frequent exacerbations despite dual bronchodilator therapy
- Risk: increased pneumonia with ICS use
Phosphodiesterase-4 Inhibitor:
- Roflumilast - oral anti-inflammatory; reduces exacerbations in severe COPD with chronic bronchitis phenotype; GI side effects (nausea, weight loss)
Antibiotics (preventive):
- Azithromycin (250 mg/day or 500 mg 3x/week) - reduces exacerbation frequency in select patients (former smokers, high exacerbation risk); risk of hearing loss and cardiac arrhythmia
Mucolytics:
- N-acetylcysteine and carbocysteine - modest benefit in reducing exacerbations in non-ICS patients
Alpha-1 Antitrypsin Augmentation:
- IV AAT replacement for patients with AAT deficiency and established airflow obstruction; slows emphysema progression
Initial Treatment Algorithm (GOLD Groups):
- Group A: As-needed bronchodilator (SABA or SAMA)
- Group B: Long-acting bronchodilator (LAMA preferred, or LABA+LAMA)
- Group E: LAMA + LABA; add ICS if eos ≥300 or frequent exacerbations
COPD Exacerbations
Definition: Acute worsening of respiratory symptoms beyond normal day-to-day variation requiring additional therapy.
Common Triggers: viral infections (most common), bacterial infections (H. influenzae, S. pneumoniae, M. catarrhalis, Pseudomonas in severe COPD), air pollution
Severity Classification:
- Mild: managed with increased bronchodilators alone
- Moderate: requires antibiotics and/or systemic corticosteroids
- Severe: requires hospital admission
Treatment:
- Bronchodilators: increase frequency of SABA (± SAMA); nebulization in severe cases
- Systemic corticosteroids: prednisone 40 mg/day × 5 days (short course equivalent to longer course); reduces treatment failure and hospital length of stay
- Antibiotics: indicated for purulent sputum, severe exacerbations; aminopenicillin ± clavulanate, macrolides, or tetracyclines; fluoroquinolones for Pseudomonas risk
- Supplemental oxygen: target SpO2 88-92% to avoid hypercapnic respiratory failure
- NIV (Non-invasive ventilation): for acute hypercapnic respiratory failure (pH <7.35, PaCO2 >45); reduces intubation rate and mortality
- Mechanical ventilation: if NIV fails or contraindicated
Post-exacerbation care: pulmonary rehabilitation within 4 weeks improves outcomes.
Interventional & Surgical Options
Bronchoscopic Therapies (for severe emphysema):
- Endobronchial valves (EBV) - one-way valves causing lobar atelectasis; most effective with absent collateral ventilation (Chartis assessment); risk of pneumothorax
- Coils - mechanical compression of hyperinflated lung
- Vapor (thermal) ablation - targeted delivery of heated steam to destroy emphysematous lung
Lung Volume Reduction Surgery (LVRS):
- Best candidates: upper-lobe predominant emphysema + low baseline exercise capacity after pulmonary rehab
- NETT trial showed survival benefit in this subgroup; high-risk if FEV1 <20% + homogeneous emphysema or DLCO <20%
Lung Transplantation:
- Last resort for end-stage COPD; bilateral lung transplant preferred
- Improved quality of life; uncertain survival benefit
Prognosis
- BODE Index predicts mortality: BMI, Obstruction (FEV1), Dyspnea (mMRC), Exercise capacity (6MWT)
- Higher BODE score = worse prognosis
- Frequent exacerbations, low DLCO, hypoxemia, hypercapnia, pulmonary hypertension, low BMI are all adverse prognostic factors
Source: Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 303
This is a shared conversation. Sign in to Orris to start your own chat.