
The images is showing the answer of how body fluids maintain homeostasis so according to the image answer can you provide me answer as similar as in it or make a complete notes on it
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here are complete notes on How Body Fluids Maintain Homeostasis — Renal Mechanism (Long-Term Regulation of Blood Pressure), based directly on the content in your image and enriched with authoritative textbook detail.
How Body Fluids Maintain Homeostasis
Renal Mechanism / Long-Term Regulation of Blood Pressure
The kidneys play a central role in the long-term regulation of blood pressure (BP). Unlike the neural mechanism (which acts quickly but transiently), the renal mechanism continues to regulate BP even when neural regulation fails — hence it is called long-term regulation.
The kidneys regulate BP via two main mechanisms:
- Renin–Angiotensin–Aldosterone System (RAAS)
- Action of Antidiuretic Hormone (ADH)
1. Renin–Angiotensin–Aldosterone System (RAAS)
Trigger
When blood pressure decreases → blood flow to the kidney decreases.
Step-by-Step Cascade
Blood pressure decreases
↓
Blood flow to kidney is decreased
↓
Juxtaglomerular (JG) cells in the kidney are stimulated
↓
JG cells release RENIN into the bloodstream
↓
Renin acts on Angiotensinogen (produced by liver)
↓
Angiotensinogen → Angiotensin I (Ang I)
↓ [Angiotensin-Converting Enzyme (ACE) — in lung capillaries]
Angiotensin I → Angiotensin II (Ang II)
↓ ↓
Causes vasoconstriction Stimulates ALDOSTERONE secretion
(↑ Total Peripheral (from zona glomerulosa of adrenal gland)
Resistance) ↓
Increases Na⁺ and water reabsorption
by the kidneys (↑ ECF volume)
↓_________________________________↓
LEADS TO INCREASE IN BP
Key Points
| Component | Source | Action |
|---|---|---|
| Renin | Juxtaglomerular cells of kidney | Cleaves angiotensinogen → Ang I |
| Angiotensinogen | Liver | Precursor protein |
| ACE | Lung capillary endothelium | Converts Ang I → Ang II |
| Angiotensin II | Formed in lungs | Vasoconstriction + stimulates aldosterone |
| Aldosterone | Adrenal cortex (zona glomerulosa) | ↑ Na⁺ & water reabsorption, ↑ K⁺ excretion |
Net result: ↑ vascular resistance + ↑ blood volume → ↑ Blood Pressure
2. Antidiuretic Hormone (ADH) Action
Trigger
When blood pressure decreases (or blood volume decreases / osmolarity increases).
Step-by-Step Cascade
Blood pressure (BP) decreases
↓
ADH is released from the POSTERIOR PITUITARY gland
↓
ADH acts on two receptor types:
• V1 receptors (vascular smooth muscle) → Vasoconstriction → ↑ TPR
• V2 receptors (renal collecting ducts) → ↑ water reabsorption → ↑ ECF volume
↓
Increases ECF volume AND causes vasoconstriction
↓
LEADING TO INCREASE IN BP
Key Points
- ADH is also called vasopressin because of its powerful vasoconstrictive effect
- V1 receptors → vasoconstriction of arterioles
- V2 receptors → water reabsorption in collecting ducts (↑ ECF volume)
- Increased ECF volume → increased blood volume → increased BP
RAAS Diagram (from Histology: A Text and Atlas)
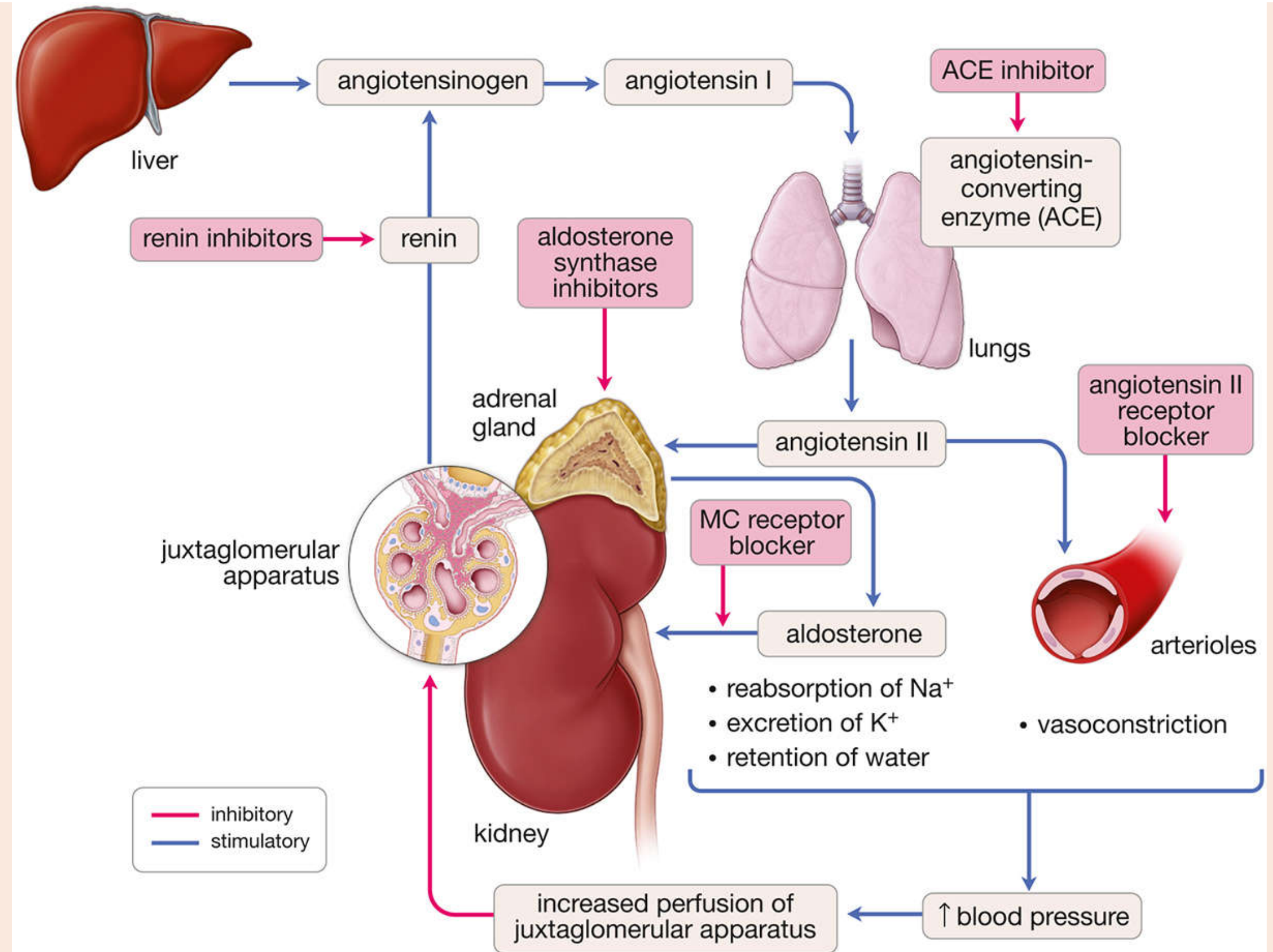
The RAAS is a multi-organ endocrine cascade. Decreased renal perfusion triggers renin release → angiotensin II production → vasoconstriction + aldosterone secretion → ↑ BP.
Comparison: RAAS vs. ADH
| Feature | RAAS | ADH |
|---|---|---|
| Trigger | ↓ renal blood flow / ↓ BP | ↓ BP, ↓ blood volume, ↑ osmolarity |
| Origin | Kidney (renin) | Posterior pituitary |
| Main hormone | Angiotensin II + Aldosterone | ADH (vasopressin) |
| Mechanism | Vasoconstriction + Na⁺/H₂O retention | Vasoconstriction + H₂O retention |
| Effect on BP | ↑ BP | ↑ BP |
Also Noted in Your Textbook (Hypothalamus — Neural Mechanism)
Though not the main focus of the image, the text at the top of the page mentions:
- Anterior hypothalamus stimulation → vasoconstriction → ↑ BP
- Posterior hypothalamus stimulation → vasodilation → ↓ BP
Clinical Relevance
- ACE inhibitors (e.g., captopril, enalapril) block the conversion of Ang I → Ang II, reducing vasoconstriction and aldosterone secretion → used in hypertension and heart failure
- Angiotensin II receptor blockers (ARBs) (e.g., valsartan, losartan) block the action of Ang II at its receptor
- Aldosterone antagonists (e.g., spironolactone) block aldosterone's effect on Na⁺ reabsorption
Sources: Anatomy, Physiology and Health Education (your textbook image); Costanzo Physiology 7th Edition, p. 174–175; Histology: A Text and Atlas, p. 1888–1889
In which any role of decrease in osmolality
Checking Date & Time
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Great question! Here is a complete explanation of the role of decreased osmolality in body fluid homeostasis.
Role of Decreased Plasma Osmolality in Homeostasis
What Causes Decreased Osmolality?
Plasma osmolality decreases (body fluids become diluted) when:
- A person drinks excess water
- Excessive IV fluids are given
- Solute loss exceeds water loss
Normal plasma osmolality = 280–295 mOsm/L
How the Body Responds — Step-by-Step
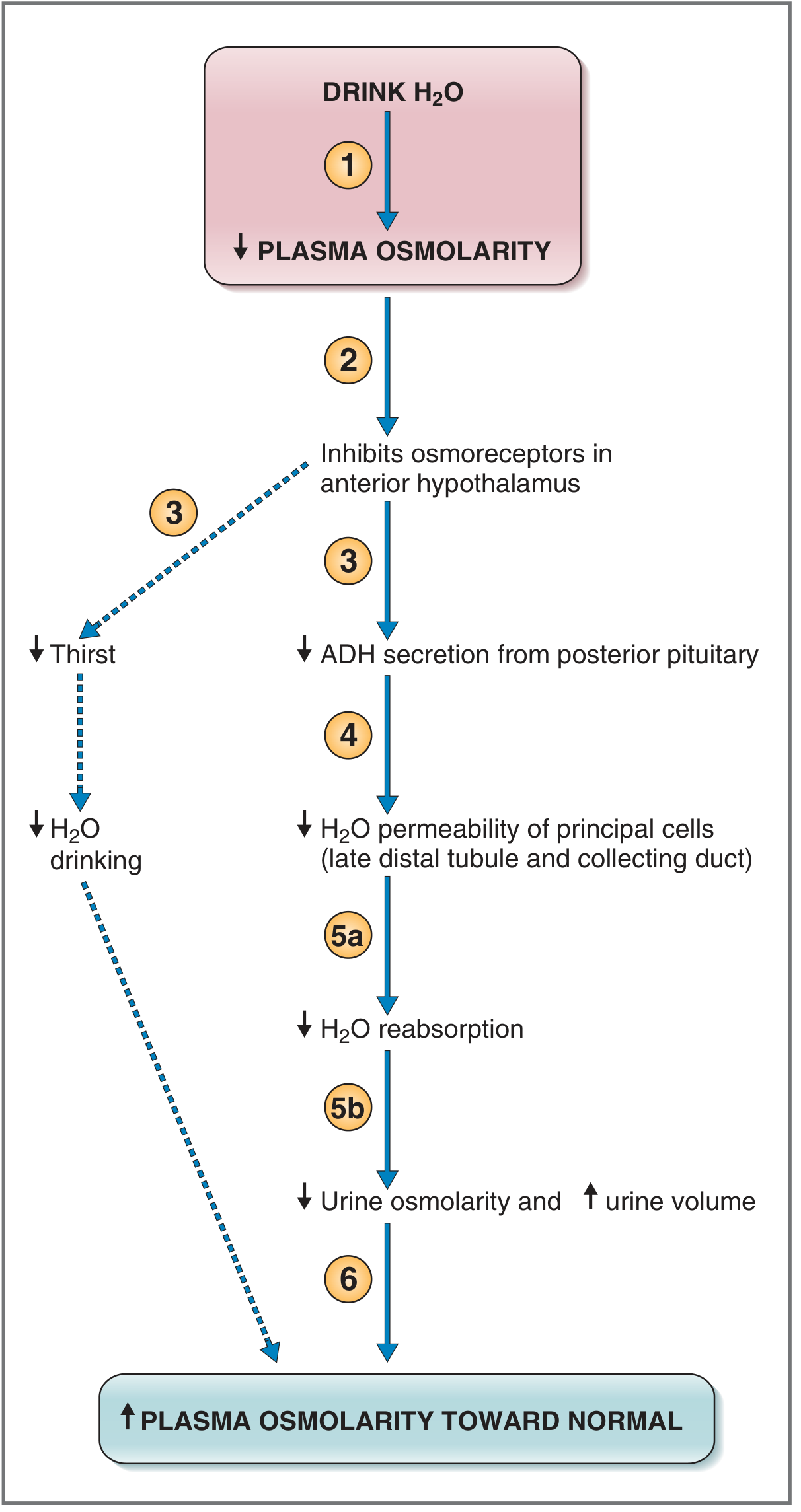
Complete Cascade:
Person drinks water (excess H₂O)
↓
① Plasma osmolality DECREASES
(solute amount same, but more water = dilution)
↓
② Osmoreceptors in the ANTERIOR HYPOTHALAMUS are INHIBITED
(these receptors are exquisitely sensitive — respond to
changes as small as 1 mOsm/L)
↓
③ Two simultaneous effects:
A) THIRST is suppressed → ↓ water drinking behavior
B) ADH secretion from POSTERIOR PITUITARY is INHIBITED
↓
④ Lower circulating ADH levels reach the kidneys
→ ↓ water permeability of principal cells in
late distal tubule & collecting duct
↓
⑤a ↓ Water reabsorption by the collecting ducts
⑤b Excess water stays in tubule → excreted as urine
→ ↓ Urine osmolarity + ↑ Urine volume (dilute urine)
↓
⑥ Less water returned to circulation
+ Thirst suppressed (less drinking)
↓
Plasma osmolality rises back toward NORMAL (negative feedback)
Key Role: ADH is the Central Hormone
| Osmolality | ADH Level | Kidney Action | Urine |
|---|---|---|---|
| ↑ High (dehydration) | ↑ High | ↑ Water reabsorption | Concentrated, low volume |
| ↓ Low (excess water) | ↓ Low / suppressed | ↓ Water reabsorption | Dilute, high volume |
Where Does Decreased Osmolality Fit in the Previous Topic (BP Regulation)?
In the ADH mechanism for blood pressure regulation (from your previous image):
- ADH is released when BP decreases
- But if osmolality also decreases at the same time, it opposes ADH release
- The body must balance both signals:
- ↓ BP → tries to stimulate ADH
- ↓ Osmolality → tries to suppress ADH
- In general, severe hypotension can override osmolality signals and still trigger ADH release (volume/pressure takes priority over osmolality in emergencies)
Summary Table
| Signal | Effect on ADH | Body Response |
|---|---|---|
| ↑ Osmolality | ↑ ADH released | Water retained → osmolality normalizes |
| ↓ Osmolality | ↓ ADH suppressed | Water excreted → osmolality normalizes |
| ↓ Blood pressure | ↑ ADH released | Water retained + vasoconstriction → BP normalizes |
| ↑ Blood volume | ↓ ADH (via atrial receptors) | Water excreted → volume normalizes |
Bottom line: Decreased osmolality acts as a negative feedback signal that suppresses ADH and thirst, causing the kidneys to excrete excess water (dilute urine) and restore normal plasma osmolality. This is a classic example of osmoregulation maintaining fluid homeostasis.
— Costanzo Physiology 7th Edition, pp. 304–305
Tonsils
Checking Date & Time
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here are complete notes on Tonsils drawn from Gray's Anatomy, Color Atlas of Human Anatomy, and KJ Lee's Otolaryngology.
TONSILS — Complete Notes
Definition
Tonsils are collections of lymphoid tissue in the mucosa of the pharynx, surrounding the openings of the nasal and oral cavities. They are secondary lymphoid organs and part of the body's immune defense system. Because of their proximity to the epithelium, they are also called lymphoepithelial organs.
Waldeyer's Tonsillar Ring
All tonsils together form a ring of lymphoid tissue around the pharynx called Waldeyer's Tonsillar Ring (Lymphoid Ring). It includes:
| Tonsil | Location |
|---|---|
| Pharyngeal tonsil (Adenoids) | Roof of nasopharynx (midline) |
| Palatine tonsils | Lateral walls of oropharynx (between palatoglossal & palatopharyngeal arches) |
| Lingual tonsil | Posterior 1/3 of tongue (base of tongue) |
| Tubal tonsils | Near opening of pharyngotympanic (Eustachian) tube |
| Lateral pharyngeal bands | Behind posterior tonsillar pillars |
Types of Tonsils — Individual Details
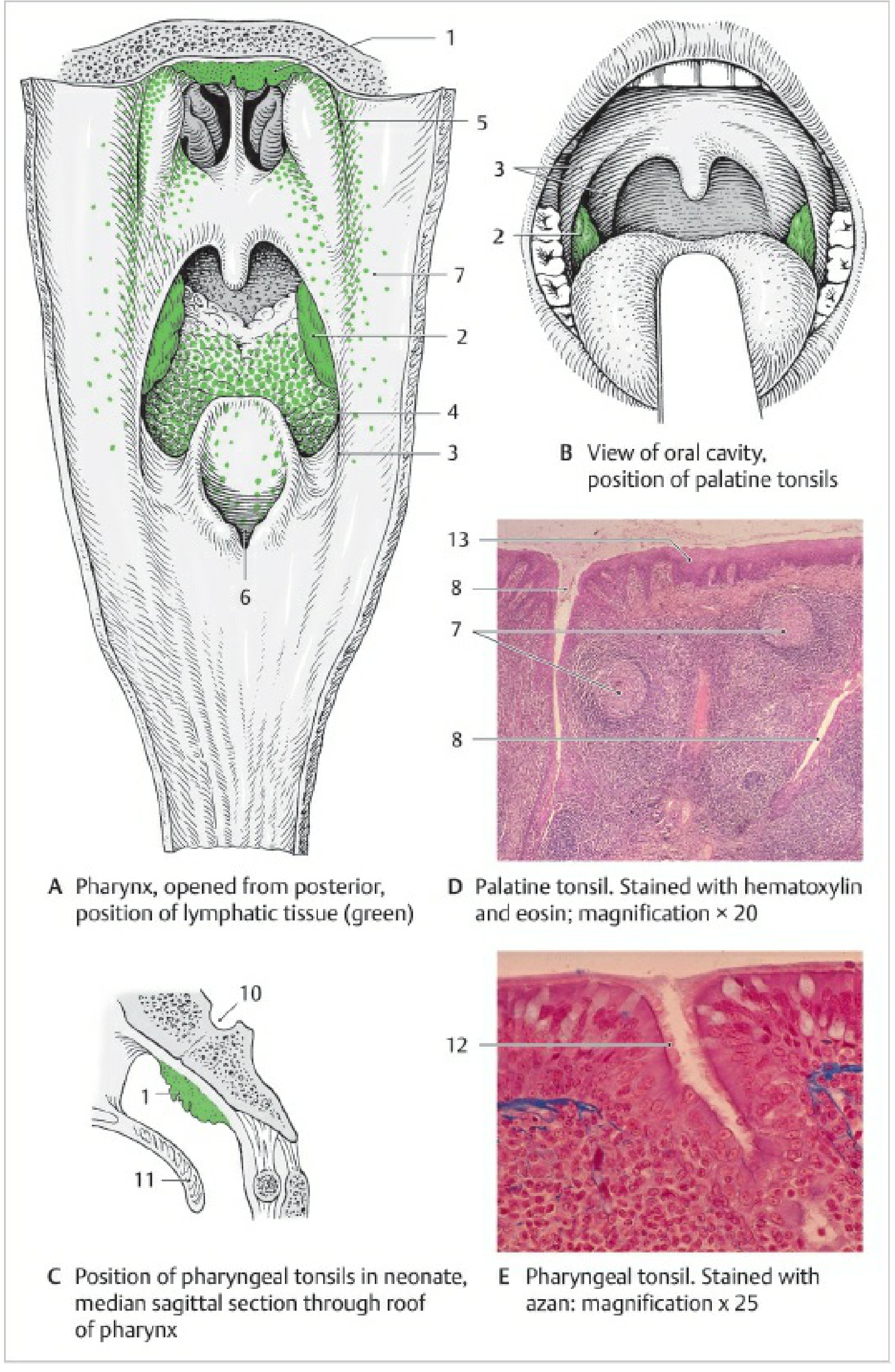
1. Pharyngeal Tonsil (Adenoids)
- Located on the roof of the nasopharynx, behind the choanae
- Shape: cauliflower-like
- Epithelium: pseudostratified ciliated columnar (respiratory) epithelium
- Has shallow infoldings (not deep crypts) between sagittally oriented mucosal elevations
- Clinical: In children, can enlarge (called adenoids/polyps) → obstructs choanae → mouth breathing, sinusitis, sleep disturbance, and if Eustachian tube is blocked → chronic ear infections
2. Palatine Tonsils
- Located in the tonsillar fossa (hollow between the palatine arches)
- Visible through the open mouth when the tongue is depressed
- Epithelium: stratified non-keratinized squamous epithelium
- Has 10–20 tonsillar crypts (deep invaginations)
- Contains aggregated lymphoid follicles with germinal centers
- Site of vigorous B lymphocyte proliferation → produces all immunoglobulin types
- Clinical:
- Acute tonsillitis — bacterial infection → sore throat (angina) + dysphagia
- Peritonsillar abscess — complication of acute tonsillitis
- Tonsillolith — calcifications in crypts → halitosis, foreign body sensation
- Mononucleosis — viral cause of tonsillar enlargement
- Tonsillectomy — surgical removal (evidence suggests it may increase long-term autoimmune risk)
3. Lingual Tonsil
- Located on the base of tongue (posterior 1/3)
- Has bumpy surface with cryptlike infoldings surrounded by secondary nodules
- Mucous-secreting posterior lingual glands open at the base of crypts
- Clinical: Lingual tonsillar hypertrophy → sleep-disordered breathing, difficult intubation
4. Tubal Tonsil
- Located at the inner (pharyngeal) opening of the Eustachian tube
- Viewed as a continuation of the pharyngeal tonsil
- Clinical: Enlargement → obstructs Eustachian tube → hearing impairment, nasal speech, chronic ear infections
General Structure of Tonsils
- Secondary lymphoid follicles directly beneath mucosal epithelium
- Each follicle has:
- Light-staining germinal center
- Dark-staining lymphocyte halo (cap thickened toward epithelium)
- Crypts — deep infoldings that increase surface area for antigen exposure
- Lymphocyte diapedesis — lymphocytes and granulocytes migrate into the epithelium, making the epithelial boundary indistinct
- Enclosed by a tough fibrous capsule
- Efferent lymphatics drain into deeper cervical lymph nodes (no afferent lymphatics)
Development (Embryology)
- Palatine tonsils develop from the dorsal remnants of the lateral extension of the 2nd pharyngeal pouch
- Tonsillar crypts appear at ~12th week of gestation
- Capsule develops by 20th week
- Tonsillar pillars (palatoglossus and palatopharyngeus muscles) derive from the 2nd and 3rd pharyngeal arches
Blood Supply
Arterial Supply to Palatine Tonsil (5 arteries)
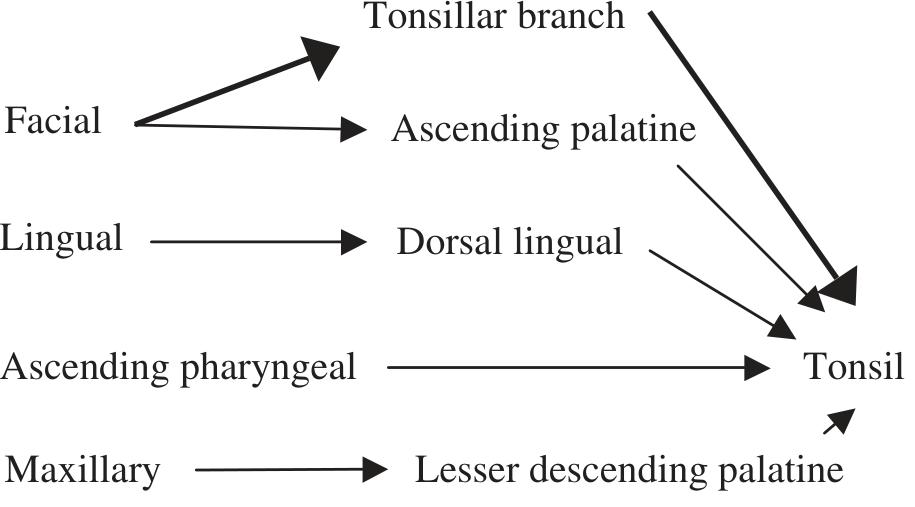
| Artery | Parent Vessel |
|---|---|
| Tonsillar branch (main supply) | Facial artery |
| Ascending palatine | Facial artery |
| Dorsal lingual | Lingual artery |
| Ascending pharyngeal | External carotid artery |
| Lesser descending palatine | Maxillary artery |
- The tonsillar branch of the facial artery is the major supply — penetrates the superior constrictor muscle to reach the tonsil
Venous Drainage
- Lingual and pharyngeal veins → drains into internal jugular vein
Nerve Supply & Lymphatic Drainage
- Nerve supply: Glossopharyngeal nerve (CN IX) and lesser palatine nerves
- Lymphatics: Drain to upper deep cervical lymph nodes (especially jugulodigastric node — the "tonsillar node")
Immunological Function
- Act as an "immunological early warning system" — encounter pathogens entering through mouth and nose
- Generate local immune responses via:
- Proliferation of B lymphocytes → antibody production (all Ig types) + memory B cells
- Generation of T helper and cytotoxic T cells
- Tonsils are part of MALT (Mucosa-Associated Lymphoid Tissue) — specifically the pharyngeal component
Summary Table
| Feature | Pharyngeal | Palatine | Lingual | Tubal |
|---|---|---|---|---|
| Location | Roof of nasopharynx | Oropharynx lateral walls | Base of tongue | Near Eustachian tube |
| Epithelium | Respiratory (pseudostratified ciliated) | Squamous non-keratinized | Squamous | Respiratory |
| Crypts | Shallow infoldings | 10–20 deep crypts | Flat infoldings | Minimal |
| Enlargement | Adenoids | Tonsillitis | Lingual hypertrophy | Tubal hypertrophy |
| Major complication | Ear infections, mouth breathing | Peritonsillar abscess | Airway obstruction | Hearing loss |
Sources: Gray's Anatomy for Students; Color Atlas of Human Anatomy Vol. 2; KJ Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.