Brachytherapy
Checking Date & Time
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive overview. Here is a synthesized answer from multiple authoritative sources.
Brachytherapy — General Overview & Principles
Definition
Brachytherapy (from Greek brachys = short distance) is a radiation therapy technique in which a radioactive source is placed within or in close proximity to the target tissue. Because radiation dose obeys the inverse square law — falling off as the square of the distance from the source — very high doses can be delivered to the tumour while sparing surrounding healthy tissues.
"As long as the sources are placed precisely within the tumour, there is minimal exposure to radiation of healthy tissues further away from the sources. This allows very high doses to be administered to the target volume." — Grainger & Allison's Diagnostic Radiology
Classification
By Placement
| Type | Description | Examples |
|---|---|---|
| Interstitial | Sources inserted directly into tissue | Prostate seeds, breast catheters |
| Intracavitary | Sources placed inside a body lumen | Cervical tandem-and-ring, vaginal cylinder, endobronchial catheter |
| Surface/Mould | Sources applied to surface | Skin tumours |
By Dose Rate
| Category | Dose Rate | Notes |
|---|---|---|
| LDR (Low Dose Rate) | < 2 Gy/hr | Continuous, often permanent seeds (e.g., ¹²⁵I in prostate) |
| IDR (Intermediate Dose Rate) | 2–12 Gy/hr | Less commonly used |
| HDR (High Dose Rate) | > 12 Gy/hr | Remote afterloading; outpatient; most common modern form |
By Duration
- Permanent implants — Radioactive seeds left in the patient; activity decays over time (e.g., ¹²⁵I, ¹⁰³Pd in prostate LDR)
- Temporary implants — Applicators/catheters placed, source delivered, then removed (e.g., HDR ¹⁹²Ir afterloading)
Radiation Sources
| Isotope | Energy | Application |
|---|---|---|
| Iridium-192 (¹⁹²Ir) | ~380 keV | HDR afterloading (prostate, cervix, breast, bronchus) |
| Iodine-125 (¹²⁵I) | 28 keV | LDR permanent prostate seeds |
| Palladium-103 (¹⁰³Pd) | 21 keV | LDR permanent prostate seeds |
| Cesium-137 (¹³⁷Cs) | 662 keV | Historical LDR intracavitary gynaecological |
| Gold-198 (¹⁹⁸Au) | 412 keV | Permanent interstitial implants |
| Radium-226 | — | Historical only; no longer used |
Technique: Remote Afterloading
Modern brachytherapy (outside of LDR prostate seeds) uses remote afterloading:
- Inactive applicators (hollow tubes, needles, or catheters) are placed in or around the tumour — ideally under real-time imaging (ultrasound, CT, or fluoroscopy).
- The patient is taken to a shielded room.
- A remote afterloading machine (e.g., Nucletron Flexitron, Varian GammaMedPlus) robotically advances the ¹⁹²Ir source along each applicator.
- The source dwells for a calculated number of seconds at 5 mm intervals within the tumour volume — the dwell time at each position determines local dose.
- The source is retracted and the applicators removed (or left for the next fraction).
This eliminates manual handling of live sources and protects staff from radiation exposure.
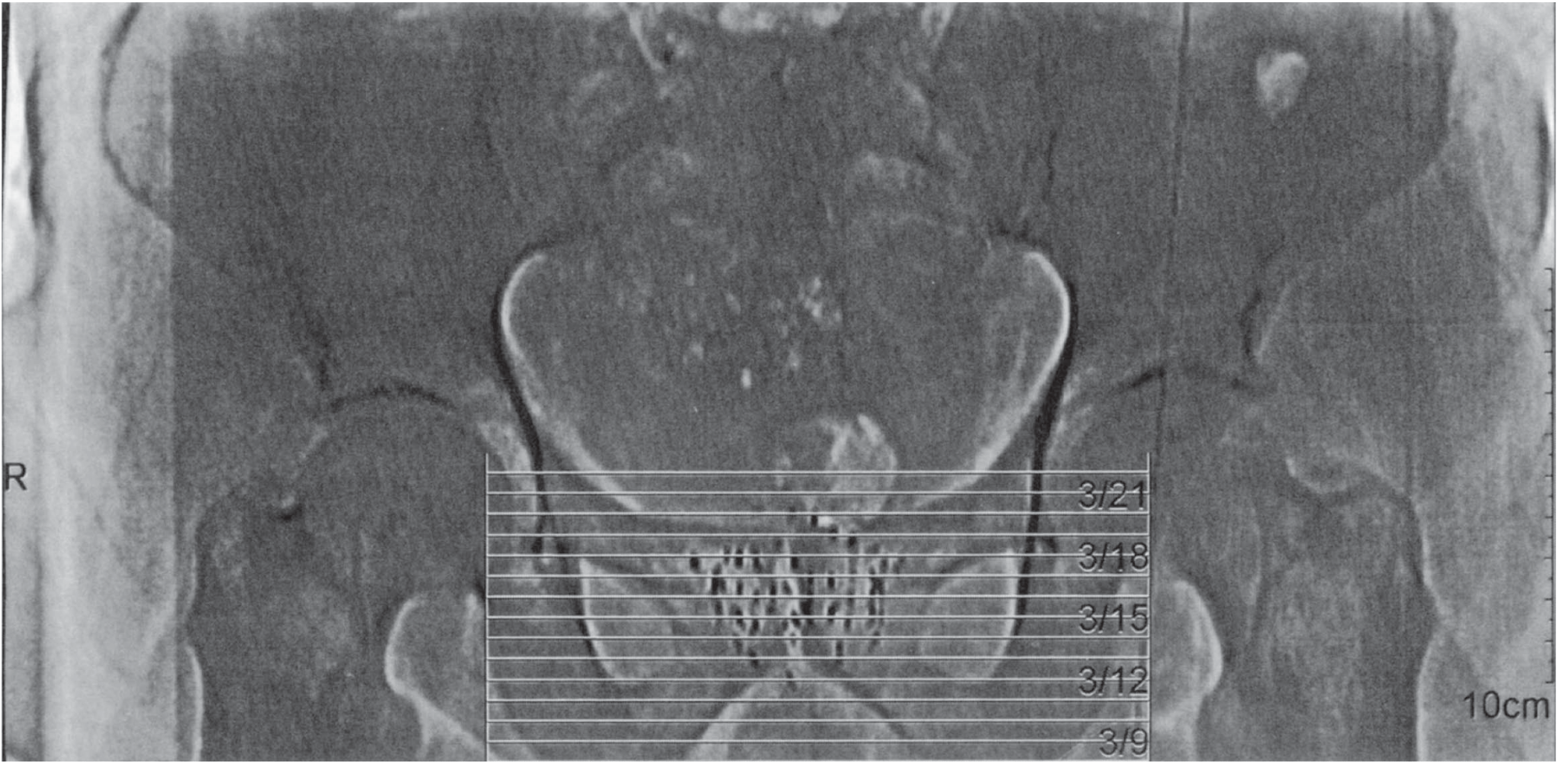
Ultrasound-guided permanent interstitial brachytherapy of the prostate — Smith and Tanagho's General Urology, 19th Ed.
Dosimetry & Imaging
- Dosimetry is computed by summing contributions from each source position within the volume.
- CT is preferred for accurate applicator localisation.
- MRI provides superior soft-tissue delineation, particularly for prostate and gynaecological cancers.
- Specific MRI sequences (proton-rich) can identify ¹²⁵I seeds in the prostate.
- Because sources move with the tumour (unlike external beam), patient setup errors and tumour motion are less clinically significant.
Clinical Applications
1. Prostate Cancer
- LDR seed implant: ¹²⁵I or ¹⁰³Pd seeds implanted transperineally under transrectal ultrasound (TRUS) guidance. Used for low-to-intermediate risk disease.
- HDR brachytherapy: ¹⁹²Ir afterloading, typically 2+ fractions; used as monotherapy or boost after EBRT for intermediate/high-risk disease.
- Potency preservation rates appear superior to prostatectomy or EBRT alone.
2. Gynaecological Cancers
- Cervical cancer: Tandem-and-ring or tandem-and-ovoid intracavitary brachytherapy is a cornerstone of radical treatment, delivering boost dose after EBRT.
- Endometrial cancer (adjuvant): Vaginal vault brachytherapy (HDR 21 Gy in 3 fractions to 5 mm depth) — vaginal control rates 98–100%. The PORTEC-2 trial demonstrated equivalence of vaginal brachytherapy vs. pelvic EBRT for high-risk early-stage endometrial cancer.
3. Breast Cancer
- Accelerated partial breast irradiation (APBI) via interstitial catheters or intracavitary balloon (MammoSite) device.
- Shorter treatment duration than whole breast EBRT (days vs. weeks).
4. Endobronchial / Lung (Palliation)
- Polyethylene catheter placed via flexible bronchoscopy adjacent to central airway tumour; HDR ¹⁹²Ir delivered in ~3 sessions over 1 week.
- Primary goal is palliation: improves cough (20–70%), dyspnoea (25–80%), haemoptysis (70–90%).
- Not appropriate when a fistula involves the airway, or when the tumour directly invades major vessels.
- Fatal haemoptysis reported in up to 5–10% of patients.
5. Other Sites
- Head and neck (tongue, lip, floor of mouth)
- Skin tumours (surface moulds)
- Bile duct / oesophageal tumours
- Soft tissue sarcoma (interstitial catheters placed intraoperatively)
Advantages Over External Beam Radiation Therapy (EBRT)
| Advantage | Mechanism |
|---|---|
| Very high tumour dose | Proximity; inverse square law confines dose |
| Sparing of normal tissue | Rapid dose falloff beyond applicator |
| Reduced treatment motion uncertainty | Sources move with tumour |
| Shorter overall treatment time | HDR delivered in minutes; LDR continuous |
| Outpatient delivery (HDR) | Remote afterloading allows day-case treatment |
Complications
- Early: Local pain/discomfort, urinary symptoms (prostate), vaginal discharge
- Late: Radiation proctitis, urinary incontinence/stricture, fistula, radiation bronchitis/stenosis (endobronchial)
- Endobronchial-specific: Fatal haemoptysis (5–10%), airway stenosis, fistula formation
Key Isotopes at a Glance
¹²⁵I — 28 keV, T½ 60 days → Permanent prostate LDR
¹⁰³Pd — 21 keV, T½ 17 days → Permanent prostate LDR
¹⁹²Ir — ~380 keV, T½ 74 days → HDR afterloading (most applications)
¹³⁷Cs — 662 keV, T½ 30 yr → Historical gynaecological LDR
Sources: Grainger & Allison's Diagnostic Radiology | Smith & Tanagho's General Urology, 19th Ed. | Schwartz's Principles of Surgery, 11th Ed. | Murray & Nadel's Textbook of Respiratory Medicine | Berek & Novak's Gynecology | Campbell-Walsh-Wein Urology
This is a shared conversation. Sign in to Orris to start your own chat.