Radioactive iodine
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching PubMed
radioactive iodine therapy thyroid
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from five major textbooks. Here is a thorough, well-organized overview of radioactive iodine.
Radioactive Iodine (RAI / ¹³¹I)
1. The Isotopes
Two main radioactive iodine isotopes are used clinically:
| Isotope | Half-life | Emission | Use |
|---|---|---|---|
| ¹²³I | 13 hours | γ only | Diagnostic scanning |
| ¹³¹I | 8 days | β + γ | Therapy (and diagnostic scans) |
| ¹²⁴I | ~4 days | Positron | PET/CT dosimetry in thyroid cancer |
The key property of all iodine isotopes - radioactive or not - is that they behave chemically identically to stable ¹²⁷I. The thyroid has no way to distinguish them, so it avidly concentrates all iodine via the sodium-iodide symporter (NIS) on follicular cells.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 973
2. Mechanism of Action
¹³¹I is administered orally (sodium iodide capsule or solution) and is:
- Rapidly absorbed from the GI tract
- Trapped by the thyroid via NIS, identical to dietary iodine
- Incorporated into thyroid follicles (within thyroglobulin, as part of T3/T4 synthesis)
The β-particles (which make up >99% of the tissue dose) have a range of only 400-2000 µm - meaning they destroy thyroid parenchyma locally with minimal radiation to surrounding structures (trachea, parathyroids, recurrent laryngeal nerves). Histologically, within weeks you see epithelial swelling and necrosis, follicular disruption, edema, and leukocyte infiltration. The γ-rays pass through tissue and can be detected externally for imaging.
- Katzung's Basic & Clinical Pharmacology 16e, p. 1087
- Goodman & Gilman's, p. 973
3. Clinical Uses
A. Diagnosis - Radioactive Iodine Uptake (RAIU) Test
A tracer dose of ¹²³I (or low-dose ¹³¹I) is given and thyroid uptake measured at 24 hours. Normal: 8-30% uptake.
- High uptake: Graves' disease, toxic adenoma, toxic multinodular goiter (endogenous overproduction)
- Low/suppressed uptake: Thyroiditis (hormone leak, not synthesis), exogenous thyroid hormone, iodine excess
A thyroid scan simultaneously maps the pattern of uptake - diffuse elevation in Graves' disease vs. a "hot nodule" in toxic adenoma.
- Textbook of Family Medicine 9e
B. Treatment of Hyperthyroidism
RAI is effective for three hyperthyroid conditions:
- Graves' disease (most common use in the US)
- Toxic multinodular goiter
- Autonomous (toxic) thyroid adenoma
Goal: Ablation of functioning thyroid tissue to induce euthyroidism or controlled hypothyroidism.
Efficacy: ~90% of Graves' disease patients are in remission within 6 months. If inadequate, re-treatment can be given 6-12 months later.
Dose: 4-15 mCi total, targeting delivery of ~8 mCi per gram of thyroid tissue based on 24-hour uptake; calculated as 80-150 µCi per gram.
When RAI is Preferred for Hyperthyroidism
RAI is the preferred choice in:
- Elderly patients and those with significant cardiac disease (avoids surgical risk)
- After relapse of Graves' post-thyroidectomy
- Failure of prolonged antithyroid drug (ATD) therapy
- Liver disease (ATDs hepatotoxic)
- Major adverse reactions to ATDs
RAI is contraindicated in:
-
Pregnancy (destroys the fetal thyroid - absolute contraindication)
-
Breastfeeding (secreted in breast milk)
-
Active/moderate-severe Graves' ophthalmopathy (can worsen eye disease - corticosteroid cover required if RAI is given)
-
Confirmed or suspected thyroid malignancy (surgery preferred)
-
Current Surgical Therapy 14e, p. 891; Goldman-Cecil Medicine
C. Treatment of Differentiated Thyroid Cancer (DTC)
DTC (papillary and follicular thyroid cancer) retains iodine uptake through NIS expression, though less avidly than normal thyroid tissue. RAI is used post-thyroidectomy for two purposes:
-
Remnant ablation - destroying residual normal thyroid tissue to:
- Improve specificity of surveillance (serum thyroglobulin, whole-body scanning)
- Prevent de novo cancer formation in remnant tissue
- Treat potential microscopic residual disease
-
Adjuvant/therapeutic treatment - treating clinically detectable metastatic or recurrent disease
ATA Guidelines on RAI use by risk:
| Risk Category | RAI Recommendation |
|---|---|
| Low-risk (intrathyroidal tumor <4 cm, no high-risk histology, no metastases) | Not recommended - no benefit in RCTs |
| Intermediate-risk (microscopic ETE, vascular invasion, regional nodes) | Consider - evidence for ~29% reduced mortality |
| High-risk (gross extrathyroidal extension, distant metastases) | Recommended |
A landmark 2022 RCT confirmed no disease-free survival benefit of RAI in low-risk PTC treated with total thyroidectomy.
Preparation for RAI in thyroid cancer:
- Low-iodine diet for 1-2 weeks prior
- TSH stimulation to >30 mIU/L (required to drive NIS expression in cancer cells):
- Thyroid hormone withdrawal for 3-4 weeks, OR
- Recombinant human TSH (rhTSH/Thyrogen) injection - equally effective, fewer symptoms
Doses:
- Remnant ablation: 30-50 mCi
- Treatment (metastatic): 100-150 mCi
- Maximum cumulative lifetime dose: ~600 mCi (controversial)
RAI does NOT work for: Medullary thyroid cancer (MTC), poorly differentiated thyroid cancer (PDTC), or anaplastic thyroid cancer (ATC) - these do not express NIS.
- Sabiston Textbook of Surgery, p. 1516; Cummings Otolaryngology
4. Practical Administration
- Prior to RAI for hyperthyroidism: if the patient has been on stable iodide (Lugol's, SSKI), uptake may be blocked for weeks - check 24-h RAIU with a tracer ¹²³I dose first
- For severely hyperthyroid, elderly, or cardiac-compromised patients: pre-treat with ATDs (methimazole or PTU) for 5-6 weeks to deplete stored hormone, then discontinue ATDs 5 days before RAI to avoid blocking uptake
- Response is gradual: symptoms improve over 2-3 months
5. Adverse Effects
| Effect | Details |
|---|---|
| Hypothyroidism | Most common long-term effect; eventually affects majority of treated patients; dose-dependent |
| Radiation thyroiditis | Acute release of preformed thyroid hormone, can transiently worsen hyperthyroidism or rarely precipitate thyroid storm |
| Graves' ophthalmopathy worsening | RAI can exacerbate GO; corticosteroids mitigate this |
| Sialadenitis | Salivary gland inflammation (also concentrates iodine) |
| Nasolacrimal duct obstruction | Higher cumulative doses |
| Infertility | Dose-dependent; higher doses used in thyroid cancer |
| Secondary malignancies | Particularly leukemia at high cumulative doses; risk is dose-dependent. A 2025 meta-analysis confirmed increased secondary hematologic malignancy risk with RAI in DTC (PMID: 40552857) |
| Fetal thyroid destruction | If given during pregnancy - absolute contraindication |
Fears about radiation-induced genetic damage and leukemia after the doses used for hyperthyroidism (<15 mCi) have not materialized over >50 years of clinical experience. Risk becomes significant at the cumulative high doses used in metastatic thyroid cancer.
- Katzung 16e; Sabiston; Goldman-Cecil
6. Thyroid Storm Caution
RAI itself can occasionally precipitate thyroid storm - the release of thyroid hormone from damaged follicles can overwhelm homeostasis, particularly if ATDs were withdrawn. This is a recognized but uncommon precipitant.
- Tintinalli's Emergency Medicine
7. Recent Evidence (2023-2026)
- PMID 40552857 (2025 Meta-Analysis): Confirmed dose-dependent increased risk of secondary hematologic malignancies after RAI for DTC - reinforces selective use in low-risk patients
- PMID 38870537 (2024 Systematic Review): RAI therapy for thyroid cancer coexisting with Hashimoto's thyroiditis - outcomes comparable to non-Hashimoto's patients
- PMID 37335288 (2023 Systematic Review): RAI has no meaningful role in medullary thyroid carcinoma - supports existing guideline recommendations
Summary: Radioactive iodine (¹³¹I) works by exploiting the thyroid's unique iodine uptake machinery to deliver a targeted β-radiation dose. It is first-line or preferred therapy for hyperthyroidism in most adults (especially Graves' disease), and a key adjuvant in differentiated thyroid cancer post-thyroidectomy. Its use in thyroid cancer has become increasingly selective, with evidence against routine use in low-risk disease. The main long-term consequence is hypothyroidism, which is expected and manageable with levothyroxine replacement.
Thyroidectomy indications, steps and types , complications
Finding Sources
Finding Sources
Searching PubMed
thyroidectomy complications outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed for a comprehensive answer. Let me compile it.
Thyroidectomy: Indications, Types, Steps & Complications
1. Indications
Thyroidectomy has three broad categories of indication:
A. Hyperthyroidism (when medical/RAI management has failed or is not preferred)
- Graves' disease - preferred when: active/moderate-severe Graves' ophthalmopathy, large goiter, suspicious nodule, patient preference, failure of antithyroid drugs, or pregnancy planned within 6 months of desired treatment
- Toxic multinodular goiter
- Toxic (autonomous) adenoma
B. Goiter
- Compressive symptoms - dysphagia, dyspnea, stridor, voice change, SVC obstruction
- Substernal/retrosternal goiter
- Cosmetic concern / large neck mass
- Failed or inappropriate RAI (e.g., very large gland, low uptake)
C. Thyroid Nodules and Cancer
-
Thyroid cancer - all histologic types (PTC, FTC, MTC, ATC)
-
Indeterminate/suspicious FNA (Bethesda IV, V, VI)
-
Bethesda III nodules in selected settings
-
Known or suspected malignancy on imaging or clinical features
-
Sabiston Textbook of Surgery, p. 1522
2. Types of Thyroidectomy
| Procedure | Definition | Typical Indication |
|---|---|---|
| Total thyroidectomy | All visible thyroid tissue excised bilaterally | Thyroid cancer, Graves' disease, bilateral MNG, MTC |
| Near-total thyroidectomy | <1 g remnant left at Berry's ligament | Variant of total, protects RLN |
| Subtotal thyroidectomy | 3-5 g remnant left (one or both sides) | Graves' disease (less used now); lower hypothyroidism rate but higher recurrence |
| Thyroid lobectomy / hemithyroidectomy | One lobe + isthmus + pyramidal lobe | Unilateral nodule, low-risk PTC <4 cm, indeterminate FNA |
| Isthmusectomy | Isthmus + pyramidal lobe only | Isthmic nodule or tracheal invasion at isthmus |
| Completion thyroidectomy | Remaining lobe removed after prior lobectomy | Malignancy confirmed on final pathology |
In modern practice, the vast majority of cases are either total thyroidectomy or thyroid lobectomy. Subtotal thyroidectomy has largely fallen out of favor due to higher recurrence rates for Graves' disease compared with total thyroidectomy.
- Sabiston, p. 1522
3. Preoperative Preparation
-
Biochemical thyroid function tests (TSH, fT4)
-
Neck ultrasound (mandatory)
-
FNA biopsy of nodules as indicated
-
For hyperthyroidism: render euthyroid pre-operatively with ATDs ± β-blockers; Lugol's solution / SSKI can be added within 10 days of surgery to reduce gland vascularity
-
For Graves' disease with high surgical risk: prophylactic calcitriol may be started pre-op
-
Voice/laryngeal assessment: all patients need baseline voice assessment; laryngoscopy is mandatory in those with voice changes, prior neck surgery, or posteriorly extending cancers
-
MEN2A patients: check calcium to rule out concurrent primary hyperparathyroidism
-
Sabiston, p. 1525-1526
4. Surgical Steps (Standard Open Technique)
Positioning & Incision
- Position: Supine, both arms tucked, neck extended with a shoulder roll; table in reverse Trendelenburg (reduces venous pressure and bleeding)
- Anesthesia: General endotracheal anesthesia; neuromonitoring ETT (with surface electrodes at vocal cords) used if intraoperative nerve monitoring (IONM) planned - muscle relaxants avoided after intubation
- Incision: Low transverse cervical incision (Kocher incision) ~2 cm above the sternal notch, placed within a natural skin crease
Exposure
- Superior and inferior skin flaps raised in the subplatysmal plane
- The midline raphe between the strap muscles (sternothyroid and sternohyoid) is divided vertically
- Strap muscles are retracted laterally to expose the thyroid lobe
- Strap muscles are divided (cut) only for very large goiters
Vascular Control (numbered sequence per illustration below)
- Middle thyroid vein divided early to allow medial rotation of the lobe
- Superior thyroid vessels (superior thyroid artery and vein) ligated and divided close to the thyroid capsule (to protect the external branch of the superior laryngeal nerve - EBSLN, which courses nearby)
- Inferior thyroid artery - identified and its branches ligated individually close to the gland (not the trunk) to protect blood supply to parathyroids and to stay away from the RLN
RLN and Parathyroid Identification
- Recurrent laryngeal nerve (RLN) - identified in the tracheoesophageal groove; traced from its entry into the larynx at the cricothyroid joint; IONM used to confirm integrity
- Parathyroid glands - both superior and inferior glands identified and their blood supply preserved; any inadvertently devascularized gland is minced and auto-transplanted into the sternocleidomastoid muscle
Final Dissection and Specimen Removal
- The lobe is dissected off the trachea, dividing the ligament of Berry (posterior thyroid suspensory ligament), where the RLN is at highest risk
- For total thyroidectomy: contralateral lobe addressed identically
- For lobectomy: isthmus divided with energy device or clamp/oversew; pyramidal lobe traced to its fibrous attachment cephalad and divided
- Specimen is oriented with sutures and sent for pathology
Closure
- Meticulous hemostasis; some surgeons use a Valsalva maneuver to test
- Strap muscles and platysma reapproximated with 3-0 absorbable sutures (small inferior midline opening left for any blood tracking)
- Subcuticular skin closure; drain generally not required
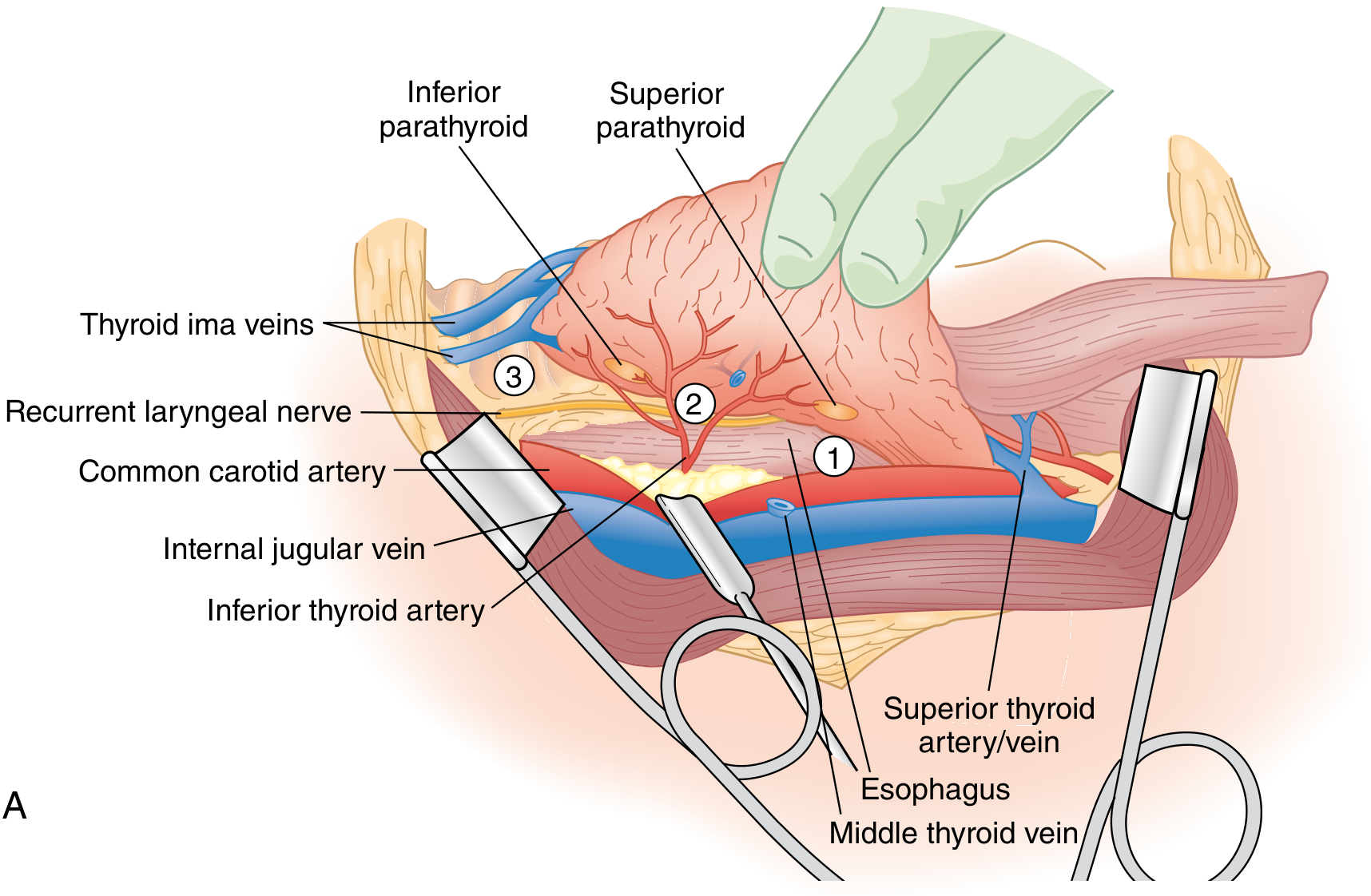
Surgical anatomy during thyroidectomy - key structures visible include the RLN, both parathyroid glands, inferior thyroid artery, and superior thyroid pedicle (Sabiston Textbook of Surgery)
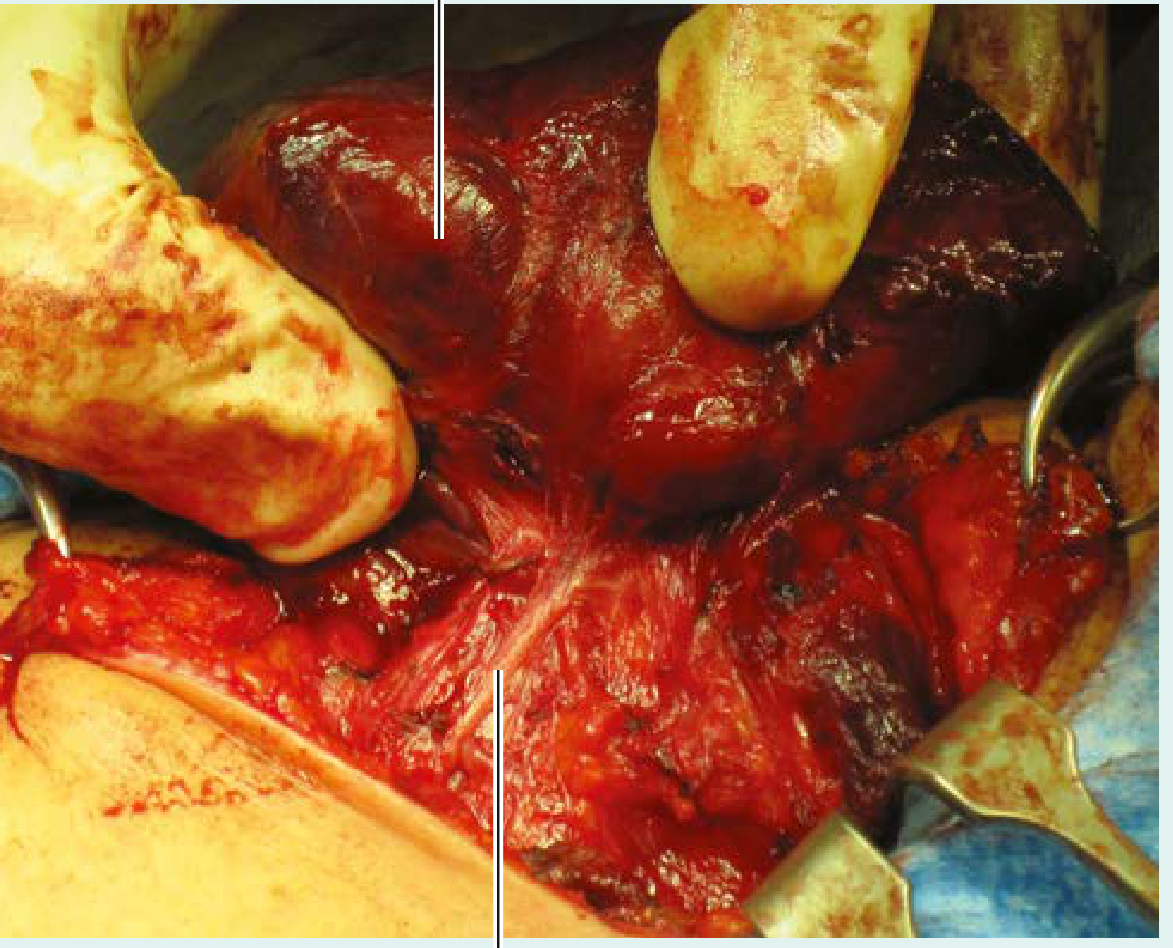
Intraoperative view: left lobe of enlarged thyroid (goiter) retracted to expose the left RLN (Gray's Anatomy for Students)
5. Alternative (Minimally Invasive / Remote-Access) Approaches
| Approach | Access Route | Notes |
|---|---|---|
| Minimally invasive video-assisted thyroidectomy (MIVAT) | Small (1.5-2 cm) central cervical incision | Endoscope-assisted; less cosmetic advantage |
| Endoscopic transaxillary | Axilla | Popular in East Asia; avoids neck scar |
| Robotic transaxillary (BABA, gasless) | Axillary ± breast ports | Longer operative time; better for large glands than pure endoscopic |
| Transoral endoscopic / robotic (TOETVA) | Via vestibule of the mouth | No external scar; risk of mental nerve injury |
These remote-access approaches offer cosmetic advantages but have longer operative times and higher complication rates in inexperienced hands. A 2023 systematic review of remote-access robotic thyroidectomy (PMID 36799913) confirmed equivalent oncologic outcomes to open surgery in properly selected patients.
6. Adjunctive Intraoperative Technologies
- Intraoperative nerve monitoring (IONM): Electromyographic monitoring of RLN via vagal or direct stimulation; increasingly used worldwide; reduces bilateral RLN injury risk especially in reoperative cases
- Near-infrared (NIR) fluorescence parathyroid imaging: Parathyroid tissue autofluoresces in NIR spectrum; allows real-time identification and reduces inadvertent devascularization
- Energy sealing devices (LigaSure, Harmonic): Reduce operative time and blood loss
7. Postoperative Care
- Position: Head and shoulders elevated 10-20° (low Fowler) to reduce venous pressure
- Diet: Advanced quickly as patient wakes
- Total thyroidectomy: serum calcium monitored; prophylactic oral calcium ± calcitriol started if at risk for hypocalcemia
- Thyroid hormone replacement (levothyroxine) started the same day for total thyroidectomy at weight-based dosing
- Discharge: Most patients leave within 2-24 hours (outpatient surgery increasingly standard)
- Return to normal activity within ~1 week
8. Complications
Early / Intraoperative
| Complication | Notes |
|---|---|
| Bleeding / neck hematoma | ~1%; can cause life-threatening airway compression requiring urgent bedside wound opening; superior venous pressure from valsalva or coughing is a trigger |
| RLN injury (transient) | 3-5%; hoarseness, dysphagia; usually resolves within 6 weeks |
| RLN injury (permanent) | ~1%; persistent hoarseness; bilateral injury causes stridor and may require tracheostomy |
| EBSLN injury | Produces high-pitch voice changes and fatigue (Amelita Galli-Curci's career-ending complication); under-diagnosed |
| Pneumothorax | Rare; associated with substernal goiter dissection |
Early Postoperative
| Complication | Notes |
|---|---|
| Transient hypocalcemia | Most common complication after total thyroidectomy; parathyroid stunning/temporary ischemia; presents as perioral tingling, Chvostek's/Trousseau's signs, muscle cramps |
| Permanent hypoparathyroidism | <1-2% in experienced hands; lifelong calcium + calcitriol replacement required |
| Tracheomalacia | Rare; softened tracheal rings after longstanding compression by goiter; may cause post-extubation stridor/collapse |
| Thyroid storm | Rare; may occur if patient was inadequately prepared (thyrotoxic) pre-op |
| Wound infection / seroma | Uncommon |
Late Complications
| Complication | Notes |
|---|---|
| Hypothyroidism | Expected after total thyroidectomy; managed with levothyroxine replacement |
| Hypoparathyroidism (permanent) | Lifelong need for calcium + active vitamin D (calcitriol) |
| Recurrence of disease | Especially Graves' after subtotal resection (up to 10-15%); or thyroid cancer recurrence |
| Dysphagia | Post-thyroidectomy dysphagia recognized as an under-reported complication (2026 systematic review PMID 41901524) - multifactorial (scar, nerve injury, strap muscle dysfunction) |
| Keloid / hypertrophic scar | Neck incision |
| Sympathetic chain injury | Rare; Horner's syndrome |
Risk Factors for Complications
-
Graves' disease carries higher absolute risk than other indications for RLN injury, hypoparathyroidism, and hematoma - though absolute risks remain low in experienced hands
-
Surgeon volume is the single most modifiable determinant: outcomes improve with increasing volume up to a threshold of ~26 cases/year; high-volume surgeons consistently show lower complication rates
-
Sabiston Textbook of Surgery, p. 1526-1528; Barash Clinical Anesthesia; Gray's Anatomy for Students
Recent Evidence Updates (2024-2026)
- PMID 38967517 (2024 Meta-Analysis): For intermediate-risk PTC, lobectomy and total thyroidectomy have comparable recurrence rates - supporting less aggressive resection in selected patients
- PMID 41901524 (2026 Systematic Review): Dysphagia is a common but underappreciated post-thyroidectomy complication deserving routine screening
- PMID 36799913 (2023 Systematic Review): Remote-access robotic thyroidectomy is safe and oncologically equivalent in selected patients at high-volume centers
Thyroid and parathyroid anatomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, well-illustrated content from multiple authoritative sources. Let me compile the full anatomy overview.
Thyroid and Parathyroid Anatomy
THYROID GLAND
1. Embryology
The thyroid develops from two anlages that fuse:
Median thyroid anlage
- Originates as an endodermal thickening in the floor of the pharynx at the foramen cecum (base of tongue)
- Descends caudally along the thyroglossal duct, which normally obliterates by week 5
- Reaches its final position anterior to the trachea by week 7
- Follicular cells begin producing thyroid hormone by week 10
- Gives rise to thyroid follicular cells (T3/T4 producers)
Lateral thyroid anlage
- Arises from the 4th and 5th pharyngeal pouches (ultimobranchial bodies)
- Fuses with the median anlage during descent
- Contributes ~one-third of final thyroid mass
- Gives rise to parafollicular C cells (calcitonin producers) - the median anlage does NOT carry these cells
Developmental anomalies of surgical relevance:
| Anomaly | Mechanism | Presentation | Treatment |
|---|---|---|---|
| Thyroglossal duct cyst | Failure of duct to resorb | Midline neck mass that rises with tongue protrusion | Sistrunk procedure (cyst + central hyoid bone) |
| Lingual thyroid | Failure to descend | Mass at tongue base; often only thyroid tissue in body | Excision or RAI; requires lifelong TH replacement |
| Ectopic thyroid tissue | Rests along descent path | Mass from tongue base to mediastinum | Surgical excision |
| Non-recurrent laryngeal nerve | Aberrant aortic arch (right side) | Usually silent; right-sided | Identify on preop imaging |
- Sabiston Textbook of Surgery, p. 1485-1487; Mulholland & Greenfield Surgery 7e
2. Gross Anatomy and Relations
- Weight: 15-30 g (normal)
- Shape: Bilobed with an isthmus; a pyramidal lobe projects superiorly from the isthmus in ~80% of people (midline, just left of center), extending as high as the hyoid bone
- Location: Anterior to the trachea, just inferior to the cricoid cartilage, within the central compartment of the neck
- Each lobe dimensions: ~5 cm craniocaudal × 2-3 cm AP × 3 cm wide
Anatomical relations:
| Direction | Structures |
|---|---|
| Anterior | Strap muscles (sternothyroid, sternohyoid), platysma, skin |
| Posterolateral | Carotid sheath (common carotid artery, internal jugular vein, vagus nerve) |
| Posteromedial | Trachea, esophagus (especially on the left), RLN in tracheoesophageal groove |
| Superior | Thyroid and cricoid cartilages |
Fascia and ligaments:
- Pretracheal fascia: Invests the thyroid; forms an easily mobilized dissection plane (except in thyroiditis or invasive cancer)
- Anterior suspensory ligament: Fascia condensation above the isthmus
- Ligament of Berry (posterior suspensory ligament): Firm posteromedial attachment to the trachea at cricoid level - the RLN is intimately associated here and is most vulnerable to injury at this point
Tubercle of Zuckerkandl: A posterolateral thyroid lobe extension at the level of the cricoid; important surgical landmark - the RLN often passes beneath it, and its identification during surgery facilitates nerve localization.
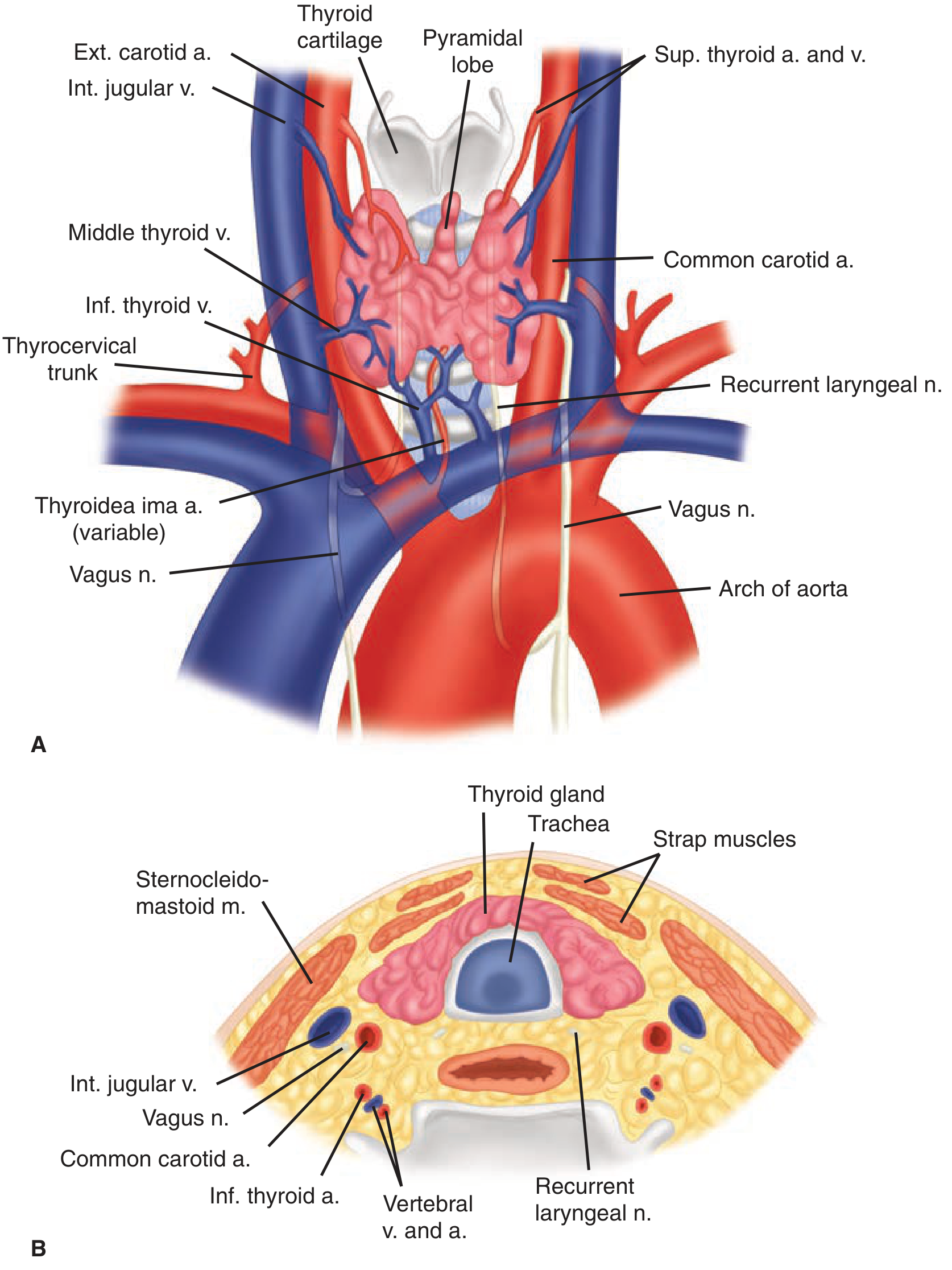
Thyroid anatomy: anterior view with arterial/venous supply (A) and cross-section showing relations (B) - Schwartz's Principles of Surgery 11e
3. Arterial Supply
| Artery | Origin | Territory |
|---|---|---|
| Superior thyroid artery | External carotid artery | Superior pole; divides into anterior and posterior branches at apex |
| Inferior thyroid artery | Thyrocervical trunk (subclavian artery) | Middle/inferior lobe; crosses the RLN - most important surgical landmark |
| Thyroidea ima artery (variant) | Aorta or innominate (1-4% of people) | Isthmus / inferior lobes; midline approach |
The inferior thyroid artery runs cephalad posterior to the carotid sheath before turning medially to enter the midthyroid lobe. Its perpendicular crossing of the RLN is the classic landmark for nerve identification.
Branches of both the inferior and superior thyroid arteries supply the parathyroid glands (predominantly the inferior thyroid artery).
- Schwartz's Principles of Surgery 11e, p. 1655; Sabiston, p. 1487
4. Venous Drainage
Three sets of veins - none run with the arteries except the superior:
| Vein | Drains into |
|---|---|
| Superior thyroid vein | Internal jugular vein (runs with superior artery) |
| Middle thyroid vein | Internal jugular vein (highly variable; lateral lobe) |
| Inferior thyroid vein | Brachiocephalic (innominate) veins via a plexus |
The middle thyroid vein is divided first in thyroidectomy to allow medial rotation of the lobe.
5. Lymphatic Drainage
Rich and extensive; first drains to Level VI (central neck) - perithyroidal nodes bordered by:
- Superior: hyoid bone
- Inferior: innominate vessels
- Lateral: carotid sheaths bilaterally
Further drainage goes to lateral neck (Levels II-V) and superior mediastinum. This pattern governs the surgical approach to thyroid cancer nodal disease (central neck dissection for Level VI; lateral neck dissection for Levels II-V).
6. Recurrent Laryngeal Nerve (RLN)
The most important nerve in thyroid surgery. Key anatomical facts:
Left RLN:
- Arises from vagus where it crosses the aortic arch
- Loops around the ligamentum arteriosum
- Ascends in the tracheoesophageal groove - a more medial, predictable course
Right RLN:
- Arises from vagus where it crosses the right subclavian artery
- Loops around the subclavian artery
- Ascends at a more oblique angle (less predictable than left)
Non-recurrent RLN (0.5-1% right; extremely rare left):
- Associated with aberrant right subclavian artery (arteria lusoria) / vascular anomaly
- Travels directly from vagus to larynx without looping - can be transected if not anticipated
Relationship with inferior thyroid artery (six anatomic patterns - see diagram below):
- The nerve is most commonly posterior to the artery (R: 53%, L: 69%)
- Or between its branches (R: 7%, L: 67%)
- Or anterior to it (R: 37%, L: 24%)
- The nerve may branch before entering the larynx - finding a thin structure should alert the surgeon that a branch is present
Highest risk point: The last few mm of the RLN as it enters the larynx at the cricothyroid joint, compressed against the Ligament of Berry.
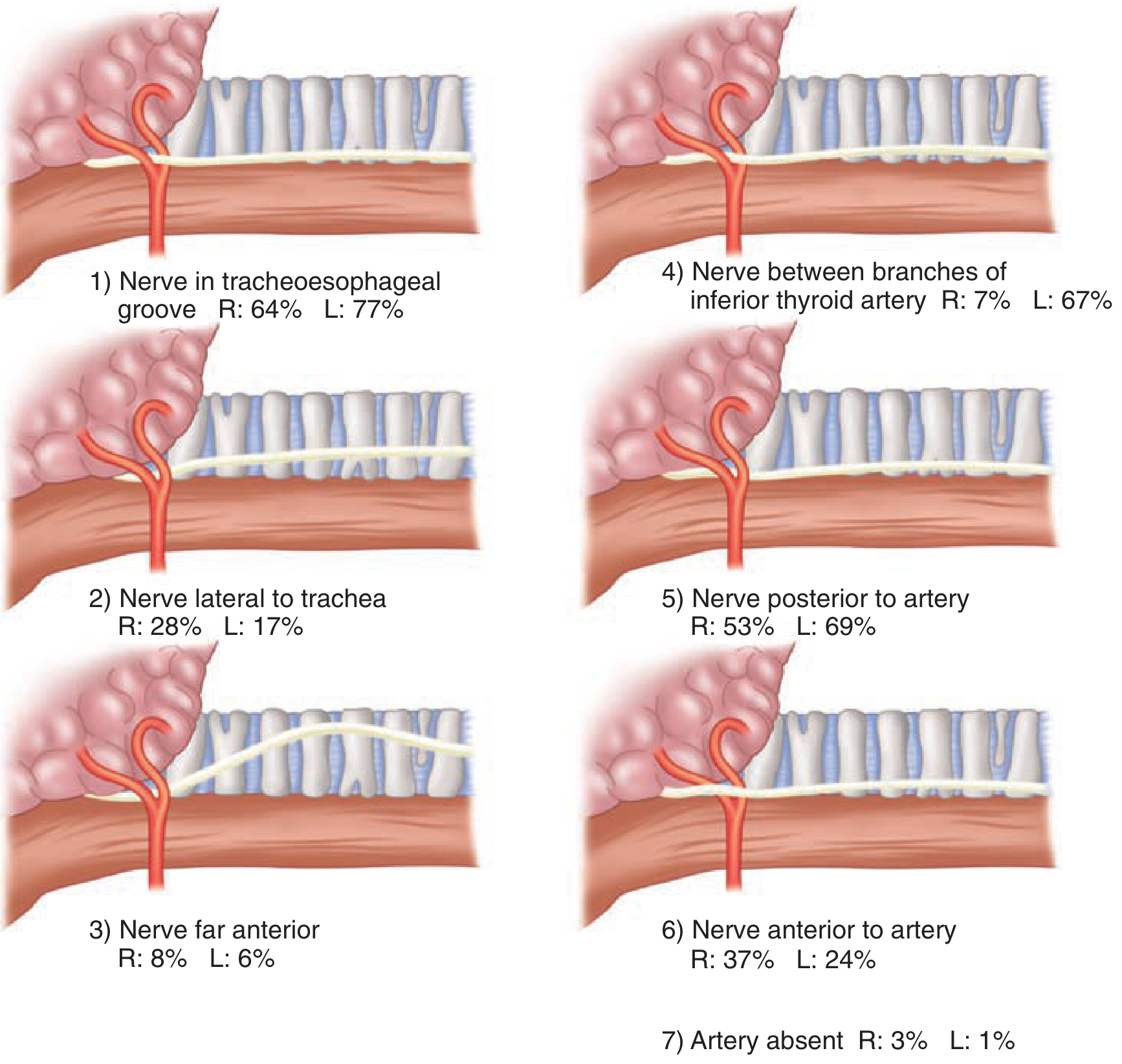
RLN-inferior thyroid artery relationship variants - Schwartz's Principles of Surgery 11e
7. External Branch of the Superior Laryngeal Nerve (EBSLN)
- Branch of the superior laryngeal nerve (from vagus)
- Innervates the cricothyroid muscle (tenses the vocal cord for high-pitch phonation)
- Runs closely with the superior thyroid artery as it approaches the superior pole - at risk when ligating the superior thyroid pedicle
- Injury causes: loss of high-pitch voice, vocal fatigue, inability to project ("Amelita Galli-Curci injury" - ended the soprano's career)
- Protected by ligating the superior thyroid vessels close to the thyroid capsule (not as a single trunk)
PARATHYROID GLANDS
1. Embryology and Numbers
| Gland | Embryologic Origin | Pouch |
|---|---|---|
| Superior parathyroid | Dorsal 4th pharyngeal pouch (with lateral thyroid anlage) | 4th |
| Inferior parathyroid | 3rd pharyngeal pouch (with thymus anlage) | 3rd |
- Most humans: 4 glands (84-87% of autopsy studies)
- 3 glands: 3-6%
- Supernumerary (5+) glands: ~5% - can number up to 12 glands
- Mirror-image symmetry between sides is a practical surgical aid for locating a missing gland
2. Gross Appearance
- Size: 30-50 mg each (approximately 3-6 mm)
- Color: Yellow-tan / Portland brick / caramel / mahogany; becomes more yellow (fattier) with age
- Shape: Oval, bean-shaped, or leaf-like
- "Gliding sign": Parathyroids glide within their surrounding fat pad as a discrete body - distinguishes them from adjacent fat (which is less distinct)
- Distinguished from surrounding fat by being darker and more defined than the surrounding yellow fat
3. Location
Superior Parathyroids
- Derived from the 4th pouch - shorter embryologic migration = more constant location
- Found in >80% of patients: posterior aspect of thyroid lobe within a 2 cm diameter area centered ~1 cm around the junction of the inferior thyroid artery and the RLN, in close proximity to the cricothyroid junction
- Located dorsal (deep/posterior) to the plane of the RLN
- Rests on the thyroid capsule posterolaterally at the upper lobe
Inferior Parathyroids
- Derived from the 3rd pouch - longer migration with thymus = more variable location
- Found in >56% of patients: inferior pole of thyroid (anterior, lateral, or posterior surface), within a globule of fat
- Located ventral (superficial/anterior) to the plane of the RLN
- Often closely associated with the thyrothymic ligament
Key rule for surgical localization: Superior gland = posterior to RLN; Inferior gland = anterior to RLN
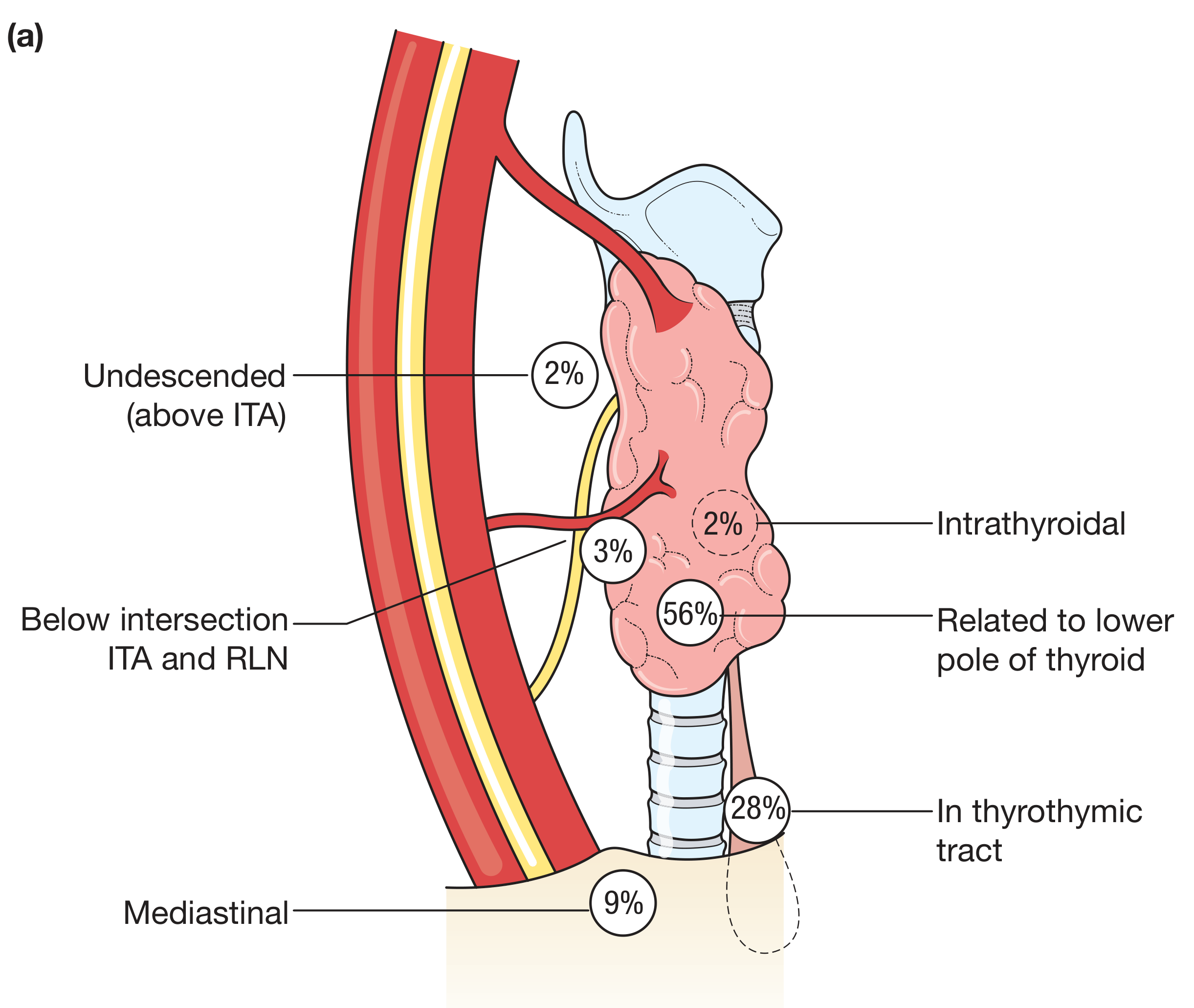
Locations of the inferior parathyroid gland with frequency percentages (Bailey & Love's Surgery 28e)
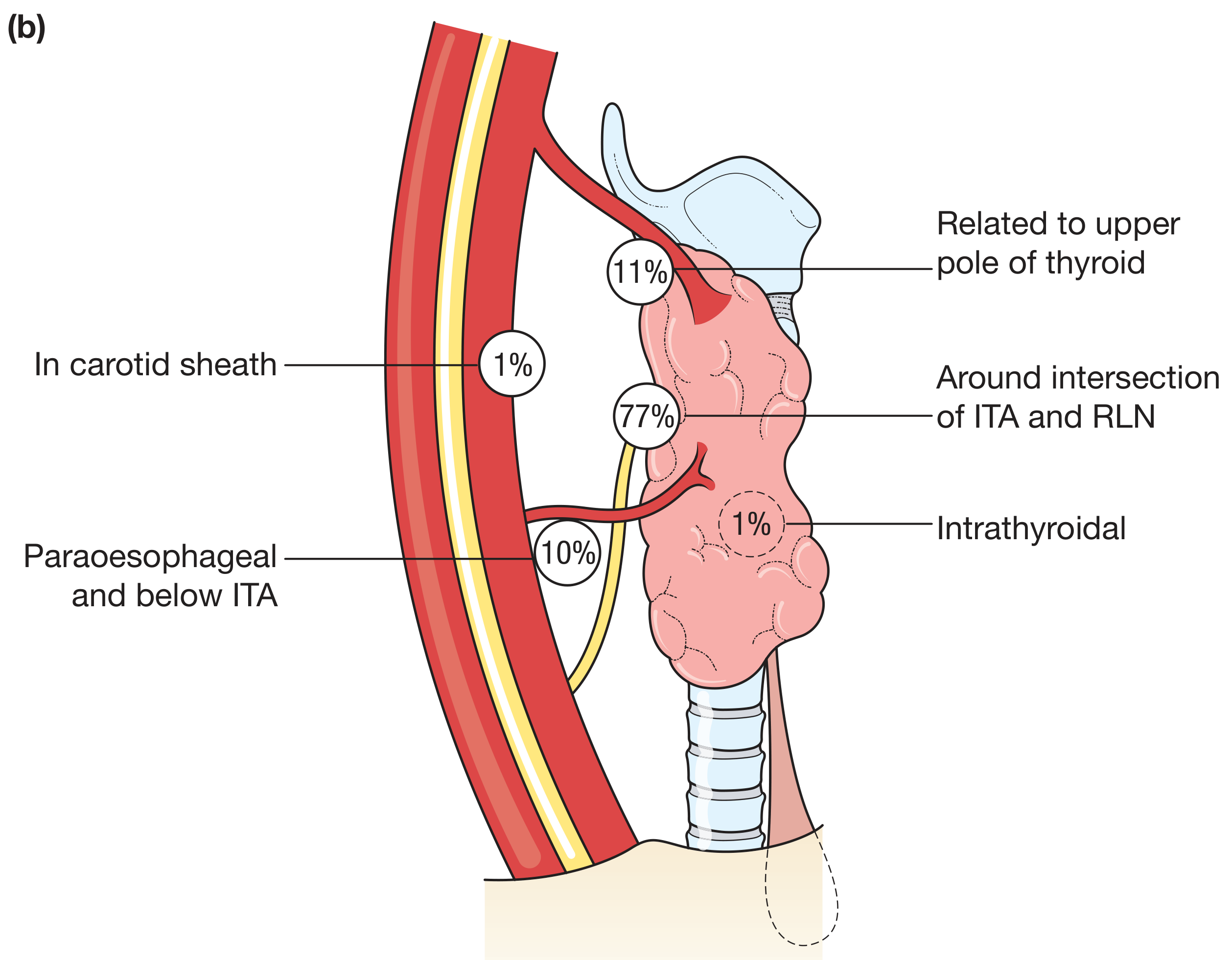
Locations of the superior parathyroid gland with frequency percentages (Bailey & Love's Surgery 28e)
4. Ectopic Parathyroid Locations
Most common sites for ectopic parathyroid adenomas (clinically relevant for hyperparathyroidism surgery):
- Anterior mediastinum / thymus (most common ectopic site)
- Retroesophageal / retrotracheal
- Intrathyroidal (up to 2-3%)
- Carotid sheath
- Undescended (above the ITA, near the upper thyroid pole)
5. Blood Supply
-
Both superior and inferior glands: Predominantly supplied by the inferior thyroid artery (branch of thyrocervical trunk)
-
Exception: ~10% of inferior glands receive dominant supply from the superior thyroid artery
-
Abundant anastomoses with: laryngeal, pharyngeal, esophageal, and tracheal arteries
-
Transient hypoparathyroidism (ischemia without devascularization) occurs in up to 20% of total thyroidectomies - usually resolves in weeks with calcium supplementation
-
Ligation of the inferior thyroid artery trunk during thyroidectomy does not always compromise parathyroid supply due to these collaterals - but branches should still be ligated individually near the thyroid capsule, not en masse
-
Cummings Otolaryngology Head & Neck Surgery; KJ Lee's Essential Otolaryngology; Bailey & Love's Surgery 28e
Quick Summary Table
| Feature | Thyroid | Parathyroid (Superior) | Parathyroid (Inferior) |
|---|---|---|---|
| Embryology | 3rd-5th pharyngeal pouches + endodermal floor | 4th pharyngeal pouch | 3rd pharyngeal pouch (with thymus) |
| Normal weight | 15-30 g | 30-50 mg | 30-50 mg |
| Number | 1 (bilobed) | 2 | 2 |
| Location | Anterior trachea below cricoid | Post. thyroid, ~1 cm above ITA-RLN junction | Inferior pole of thyroid; thyrothymic tract |
| Relation to RLN | N/A | Posterior (dorsal) to RLN | Anterior (ventral) to RLN |
| Blood supply | Superior + inferior thyroid aa. | Inferior thyroid artery (mainly) | Inferior thyroid artery (mainly) |
| Venous drainage | Superior, middle, inferior thyroid vv. | – | – |
| Cell types | Follicular cells (T3/T4), C cells (calcitonin) | Chief cells (PTH), oxyphil cells | Chief cells (PTH), oxyphil cells |
This is a shared conversation. Sign in to Orris to start your own chat.