Candle stick fracture
Reading File
Finding Sources
Searching the Web
candlestick torus buckle fracture children orthopedics
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
Reading File
Here is a thorough overview of the candlestick (torus/buckle) fracture:
Candlestick Fracture (Torus / Buckle Fracture)
What Is It?
A candlestick fracture is another name for a torus fracture (also called a buckle fracture). The term "torus" comes from the Latin word for a round protuberance or bulge - describing what the bone looks like when it buckles. The "candlestick" name comes from the same visual analogy: the cortex bulges outward like wax on a candlestick.
It is an incomplete fracture unique to children, caused by the plastic, less brittle nature of their bones.
Mechanism
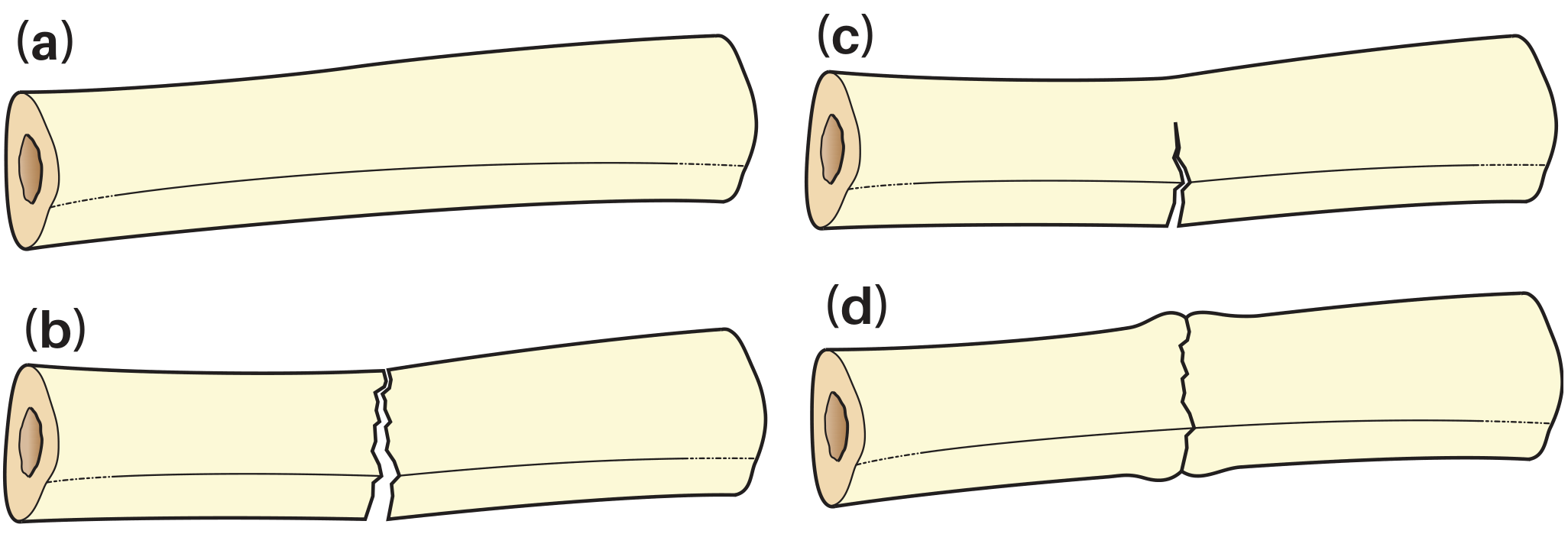
Compressive forces (axial loading) cause the cortex to buckle on the compression side rather than fracture completely across the bone. The periosteum and the far cortex remain intact. This is in contrast to:
- (a) Normal bone - no injury
- (b) Adult transverse fracture - complete failure across the whole bone
- (c) Greenstick fracture - cortex fails on the tension side only
- (d) Torus/buckle fracture - cortex buckles on the compression side
(See diagram below)
Common Sites
- Distal radius (most common - after a fall on an outstretched hand / FOOSH injury) - most frequent pediatric fracture in emergency departments
- Distal radius + ulna together
- Distal tibia (near the ankle)
- Any metaphysis subject to axial loading
Clinical Features
- Occurs in children (bones are softer and more pliable)
- Mechanism: typically a fall on an outstretched hand
- No visible deformity of the limb shape
- Soft tissue swelling over the injury site
- Point tenderness over the metaphysis
- Painless motion at joints proximal to the injury (e.g., elbow and shoulder are normal in an isolated wrist buckle fracture)
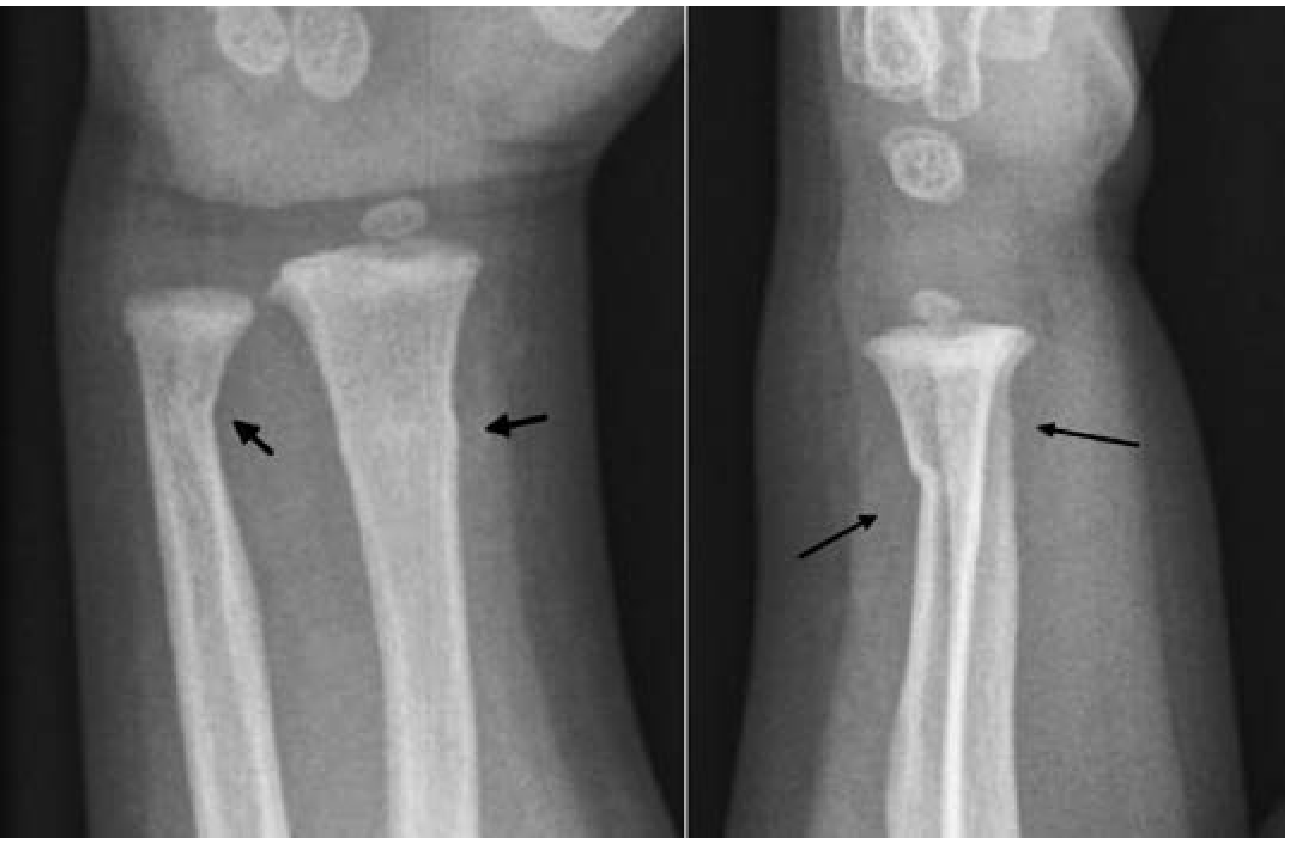
Radiology
X-ray findings can be subtle:
- Look for asymmetry, bulging, or deviation of the cortical margin at the metaphyseal flare
- Soft tissue swelling is usually evident
- No angulation, displacement, or rotational deformity - this is a key distinguishing feature
- The fracture is confined to the metaphysis (within ~1 cm of the growth plate)
Classification - Pediatric Fracture Spectrum
| Type | Description |
|---|---|
| Torus / buckle | Compression cortex buckles; both cortices intact |
| Greenstick | Tension cortex cracks; compression cortex intact |
| Plastic deformation | No visible fracture line; bone simply bows |
| Complete fracture | Both cortices fail |
Management
Torus fractures are very stable - they do NOT require reduction.
| Setting | Management |
|---|---|
| ED (distal radius buckle, no deformity/displacement/neurovascular injury) | Volar splint |
| Follow-up | Orthopedics within 1 week |
| Healing time | 4-6 weeks |
Key points:
- No reduction needed - the fracture is already aligned
- No risk of re-displacement (unlike greenstick or complete fractures)
- Does not put the child at higher risk for future fractures
- No long-term effect on growth or function when treated appropriately
Why This Only Happens in Children
Children's bone is more plastic and less brittle than adult bone due to:
- Higher collagen-to-mineral ratio
- Thicker, more elastic periosteum
- Active growth plates
Adult bone "cracks like chalk" under the same force that makes a child's bone buckle like Play-Doh.
Sources:
- Tintinalli's Emergency Medicine, p. 948
- Bailey and Love's Short Practice of Surgery, 28th Ed.
- The Harriet Lane Handbook, 23rd Ed., Table 2.2
- Children's Mercy - Buckle Fractures in Children
This is a shared conversation. Sign in to Orris to start your own chat.