Can you explain the ra myxoma
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information to provide a thorough answer. Here is a complete explanation of right atrial (RA) myxoma:
Right Atrial (RA) Myxoma
Overview
Myxoma is the most common primary tumor of the adult heart. Roughly 90% are atrial — the left atrium accounts for ~80% of those, making right atrial myxoma less common but clinically important. Overall, myxomas are benign and account for the largest share of the 80–90% of primary heart tumors that have no malignant potential.
- Robbins & Kumar Basic Pathology, p. ~470
- Harrison's Principles of Internal Medicine 22E, Ch. 282
Pathology & Morphology
Gross appearance: Myxomas are soft, gelatinous, translucent, often villous masses. They range from <1 cm to up to 10 cm. Most are pedunculated on a fibrovascular stalk, though sessile forms occur. They arise almost exclusively from the region of the fossa ovalis on the interatrial septum.
- In the RA, the tumor similarly attaches near the fossa ovalis and can swing toward — and intermittently obstruct — the tricuspid valve during diastole.
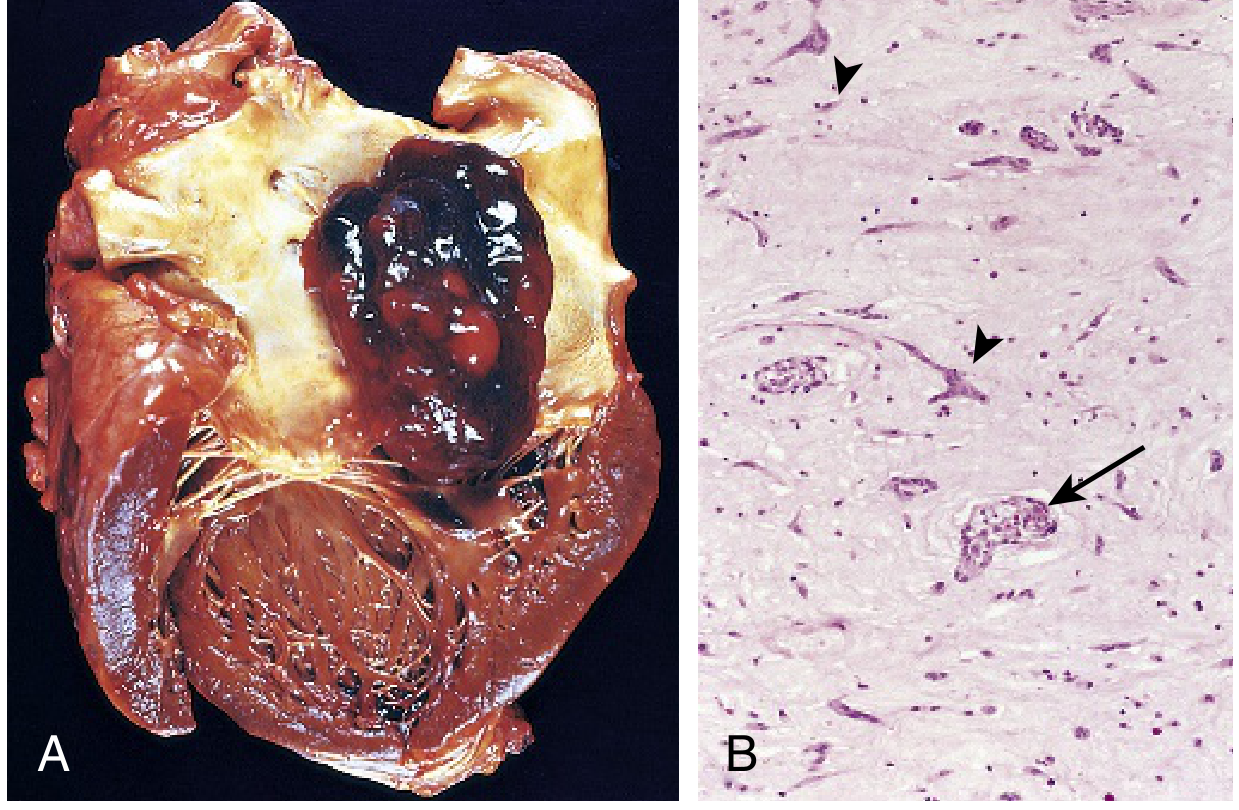
Histology:
- Stellate to multinucleate cells with hyperchromatic nuclei
- Embedded in an abundant acid mucopolysaccharide (glycosaminoglycan) ground substance
- Cells show endothelial, smooth muscle, and/or fibroblastic differentiation — all part of the neoplastic clone
- Vessel-like and gland-like formations are characteristic
- Hemorrhage, poorly organizing thrombus, and mononuclear inflammation are commonly present
Sporadic vs. Familial/Syndromic
| Feature | Sporadic | Familial / Carney Complex |
|---|---|---|
| Age | Older adults | Younger patients |
| Number | Usually solitary | Often multiple |
| Location | LA >> RA | Any chamber, including ventricles |
| Recurrence after resection | Low | Higher risk |
Carney complex (autosomal dominant, PRKAR1A mutation) is the prototypical syndromic setting, featuring myxomas at atypical sites, skin pigmentation, and endocrine tumors.
Clinical Presentation
RA myxoma manifests differently from the more common LA myxoma because it affects right-sided hemodynamics:
Obstructive Symptoms (right-sided)
- Tricuspid valve obstruction → mimics tricuspid stenosis
- Signs of right heart failure: peripheral edema, hepatomegaly, ascites, elevated JVP
- RA myxoma is actually a recognized, albeit uncommon, cause of tricuspid regurgitation as the tumor traumatizes the valve leaflets
- Syncope or dizziness, often positional (gravity alters tumor position)
Embolic Phenomena
- Tumor fragments or associated thrombus embolize to the pulmonary circulation → pulmonary emboli, pulmonary hypertension
- This distinguishes RA from LA myxoma, where emboli go systemically (stroke, peripheral ischemia)
Constitutional / Paraneoplastic Syndrome
Myxoma cells secrete IL-6, driving a systemic inflammatory response:
- Fever, malaise, weight loss, cachexia
- Arthralgias, rash, Raynaud's phenomenon, digital clubbing
- Lab abnormalities: ↑ ESR, ↑ CRP, hypergammaglobulinemia, anemia, leukocytosis, thrombocytopenia
This triad can masquerade as endocarditis, collagen vascular disease, or a paraneoplastic syndrome, leading to diagnostic delays.
Auscultation: "Tumor Plop"
A characteristic low-pitched early-to-mid diastolic sound heard when the tumor impacts the tricuspid valve or ventricular wall. It occurs 80–120 ms after S2 and can be mistaken for an opening snap or S3. For RA myxoma, the plop is heard along the right sternal border and may be louder on inspiration.
Diagnosis
| Modality | Role |
|---|---|
| Echocardiography (TTE/TEE) | First-line; identifies size, shape, attachment site, and motion; detects prolapse through tricuspid valve |
| CT | Delineates tumor composition and relationship to surrounding structures |
| MRI | Best characterizes tissue composition; useful for surgical planning |
3D echocardiography allows real-time visualization of the tumor prolapsing across the valve.
Treatment
Surgical resection is the only effective therapy. Key surgical principles:
- Cardiopulmonary bypass with ventricular standstill (cardioplegia before cardiac manipulation) to prevent tumor fragmentation
- For RA myxoma, a full-thickness section of interatrial septum should be resected if the tumor attaches at the fossa ovalis
- Large septal defects are patched with knitted Dacron cloth to prevent distortion or arrhythmia
- Prognosis is excellent — surgical cure is achieved in the vast majority
Recurrence is rare in sporadic cases but should be surveyed in familial/Carney complex settings.
Summary Table
| Feature | Detail |
|---|---|
| Frequency | ~10% of all atrial myxomas (LA >> RA) |
| Origin | Fossa ovalis, interatrial septum |
| Gross | Gelatinous, pedunculated, soft |
| Histology | Stellate cells in mucopolysaccharide matrix; vessel-like structures |
| Obstruction | Tricuspid valve → right heart failure signs |
| Embolism | Pulmonary circulation |
| Constitutional | IL-6-mediated fever, arthralgias, ↑ESR, ↑CRP |
| Auscultation | "Tumor plop" (right sternal border, louder on inspiration) |
| Diagnosis | Echocardiography (TTE/TEE) |
| Treatment | Surgical excision (curative) |
Sources: Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E; Fuster & Hurst's The Heart 15E; Schwartz's Principles of Surgery 11E
This is a shared conversation. Sign in to Orris to start your own chat.