Cyanotic heart disease precipitation
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough answer on precipitants of cyanotic heart disease (hypercyanotic/tet spells).
Precipitation of Cyanotic Heart Disease (Hypercyanotic Spells)
Overview
"Precipitation" in cyanotic congenital heart disease refers to the triggers and pathophysiologic mechanisms that precipitate hypercyanotic spells (also called tet spells, hypoxic spells, or "blue spells"). Though classically described in Tetralogy of Fallot (TOF), these spells can also occur in tricuspid atresia, transposition of the great arteries (TGA), and Eisenmenger's syndrome. They are most common in infants aged 2–18 months.
Core Pathophysiology
The central mechanism is a transient imbalance between pulmonary blood flow (PBF) and systemic blood flow that dramatically increases right-to-left shunting:
| Mechanism | Effect |
|---|---|
| ↑ Right ventricular outflow tract obstruction (RVOTO) | Less blood reaches the lungs |
| ↑ Pulmonary vascular resistance (PVR) | Diverts blood away from lungs |
| ↓ Systemic vascular resistance (SVR) | Favors right-to-left shunting across VSD |
| Hypovolemia / tachycardia | Reduces PBF |
The RVOTO in TOF is dynamic — infundibular (subpulmonary) muscle is susceptible to spasm driven by sympathetic tone, worsening obstruction acutely.
Precipitating Triggers
1. Decrease in SVR
Any event that acutely lowers systemic vascular resistance increases the right-to-left shunt across the VSD:
- Crying
- Defecation / straining
- Waking from sleep
- Feeding
- Fever
2. Increased Sympathetic Stimulation
Catecholamine surges increase heart rate and infundibular muscle tone, worsening dynamic RVOTO:
- Agitation, pain, anxiety
- Vigorous physical exertion
3. Hypovolemia / Peripheral Vasodilation
- Bathing (warm water → peripheral vasodilation → ↓ SVR)
- Dehydration, diarrhea, vomiting
- Blood loss or anemia (also reduces oxygen-carrying capacity)
4. Tachycardia
Reduces diastolic filling time → decreased RV filling → increased dynamic RVOTO
5. Iatrogenic Triggers
- Cardiac catheterization — can cause spasm of RVOT muscle, directly precipitating a hypercyanotic episode — SCHWARTZ'S PRINCIPLES OF SURGERY, 11th Ed.
- Painful procedures → pulmonary vasospasm → pulmonary hypertensive crisis (mimics tet spell)
The Vicious Cycle
Once a spell begins, it self-perpetuates:
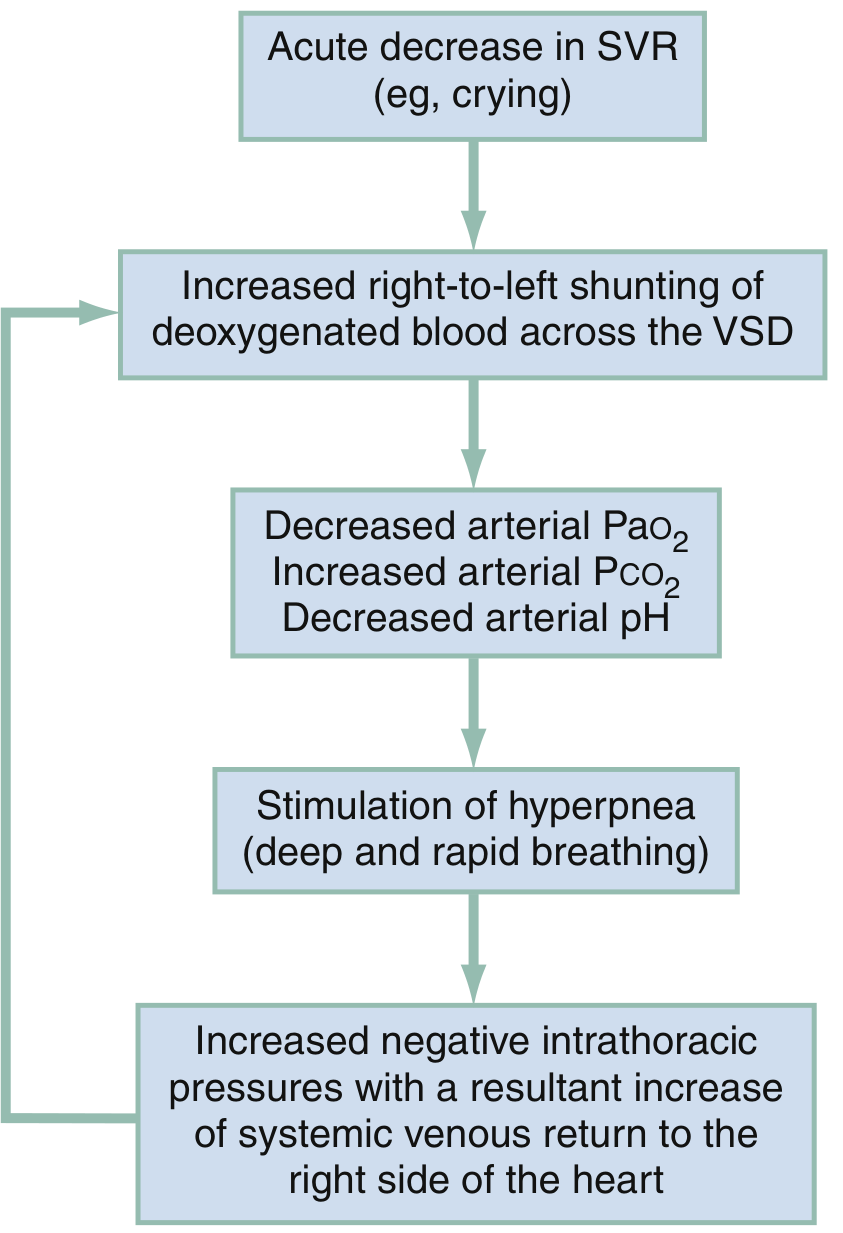
Fig. Pathophysiologic mechanisms of a hypoxic (tet) spell — Rosen's Emergency Medicine, 10th Ed.
- Trigger → acute ↓ SVR or ↑ RVOTO
- Increased R→L shunting across VSD
- ↓ PaO₂, ↑ PaCO₂, ↓ arterial pH
- Metabolic acidosis stimulates hyperpnea (deep, rapid breathing)
- Hyperpnea increases negative intrathoracic pressure → ↑ systemic venous return to RV
- Greater RV volume is shunted R→L across the VSD → worsening cyanosis
- Cycle perpetuates — can progress to syncope, seizures, stroke, or death
— Rosen's Emergency Medicine, p. 3211
Clinical Presentation of a Spell
- Paroxysmal hyperpnea + worsening cyanosis
- Prolonged crying, irritability → limpness
- Intensity of the systolic murmur decreases (less flow across RVOTO, more shunting across VSD)
- Severe spells: syncope, cerebrovascular accident, death
Management of Precipitated Spells
| Intervention | Mechanism |
|---|---|
| Knee-to-chest / squatting position | ↑ SVR → ↓ R→L shunt; older children spontaneously squat |
| Supplemental O₂ | Limited effect alone, but reduces PVR modestly |
| Morphine 0.1–0.2 mg/kg IM | Sedation → ↓ catecholamines → ↓ RVOTO spasm; note: may lower SVR via histamine |
| Fentanyl 1 μg/kg IV/IM or 1.5–2 μg/kg IN | Preferred alternative (no histamine release) |
| Midazolam 0.2–0.3 mg/kg IN | Sedation, anxiolysis |
| Ketamine 1–2 mg/kg IV / 3–5 mg/kg IM | Excellent: sedation + ↑ SVR |
| NaHCO₃ 1 mEq/kg IV | Breaks acidosis → ↓ hyperpnea drive |
| Phenylephrine 0.01–0.02 mg/kg IV | α-agonist → ↑ SVR → ↓ R→L shunting |
| Propranolol 0.1–0.2 mg/kg IV | Reduces infundibular spasm; β-blockade also used long-term for spell prevention |
| IV fluid bolus | Corrects hypovolemia → ↑ PBF |
— Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Mulholland & Greenfield's Surgery, 7th Ed.
Prevention (Long-term)
- Oral propranolol — suppresses incidence of spells by reducing RVOT spasm and heart rate
- Transfusion for anemic infants (polycythemia is compensatory; anemia worsens spells)
- Early surgical repair (complete repair 4–6 months; earlier if spells occur or cyanosis worsens)
- Modified Blalock-Taussig-Thomas shunt as palliation in high-risk neonates
Key Points to Remember
- Peak incidence of tet spells: 2–4 months (some sources say 3–18 months)
- Any cause of ↓ SVR or ↑ RVOTO or ↑ PVR can precipitate a spell
- Squatting is the classic spontaneous compensatory maneuver in older children
- Distinguish from pulmonary hypertensive crisis (triggered by painful procedures in CHD with large VSDs — treat with ventilation, O₂, NaHCO₃, pulmonary vasodilators)
- Murmur softens or disappears during a spell (paradoxically), because less blood traverses the obstructed RVOT
This is a shared conversation. Sign in to Orris to start your own chat.