Left it dislocation
Reading File
Finding Sources
Finding Sources
Searching the Web
left hip dislocation types classification management orthopedics
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have comprehensive information from multiple authoritative textbooks. Here is a full, well-organized response on left hip dislocation:
Left Hip Dislocation
Hip dislocations are orthopedic emergencies. The same principles apply whether left or right - the side determines the examination findings and imaging interpretation but not the management pathway.
Overview
Native hip dislocations result from high-energy trauma (most commonly motor vehicle collisions). Up to 95% of patients have associated injuries. The hip joint is intrinsically stable due to its deep bony socket and strong ligamentous/muscular support, so enormous force is required to dislocate it. - Tintinalli's Emergency Medicine
Posterior dislocations account for >90% of all hip dislocations; the remaining 10% are anterior (superior or inferior). - Tintinalli's Emergency Medicine
Types of Hip Dislocation
1. Posterior Dislocation (>90%)
Mechanism: A posterior force applied to a flexed knee - the classic "dashboard injury" in a head-on collision. The hip is in flexion at the time of impact; the more flexion present, the lower the risk of an associated acetabular fracture.
Clinical appearance:
- Left leg shortened
- Adducted and internally rotated (this is the key finding that distinguishes it from a femoral neck fracture, which typically presents with external rotation)

Associated injuries:
- Acetabular fractures
- Femoral neck and shaft fractures
- Sciatic nerve injury (~10% of cases - runs just posterior to the joint)
- Ligamentous knee injury
2. Anterior Dislocation (~10%)
Mechanism: Forced abduction of the thigh (e.g., fall or MVC), causing the femoral head to lever out through an anterior capsular tear.
Three subtypes based on where the femoral head comes to rest:
| Subtype | Also Called | Hip Position | Clinical Appearance |
|---|---|---|---|
| Inferior | Obturator | Flexed at time of injury | Abducted, externally rotated, flexed |
| Superior (pelvic) | Iliac | Extended | Extended, externally rotated |
| Pubic | - | Extended | Extended, externally rotated |
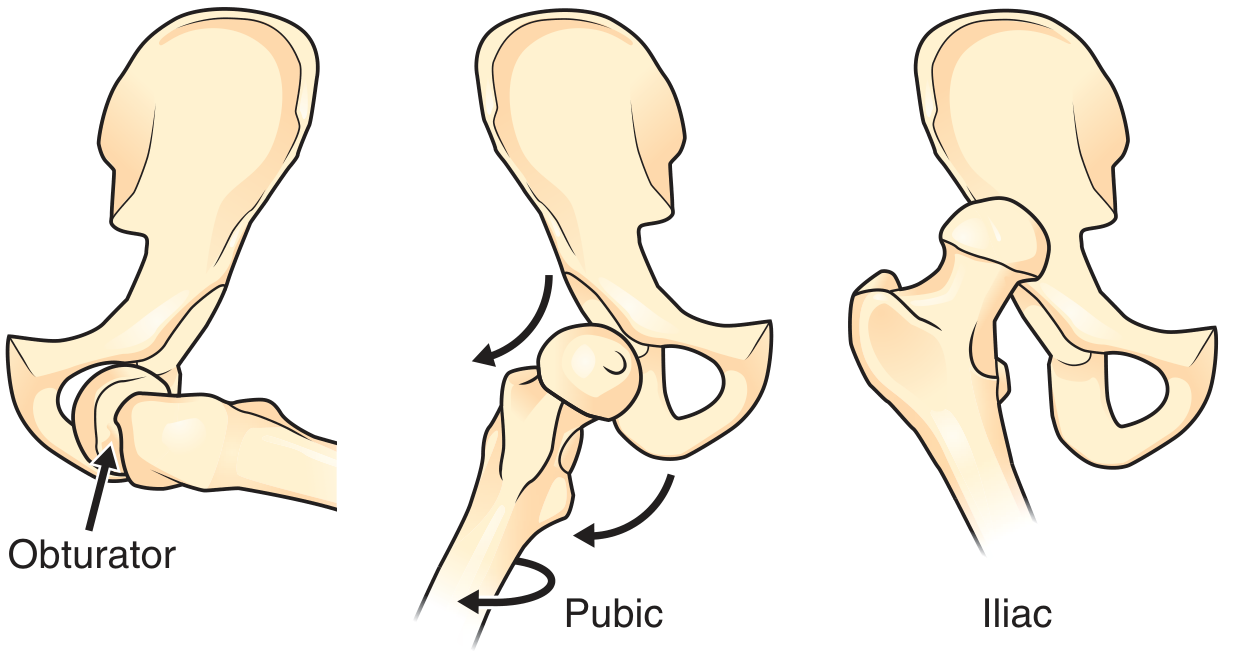
Key difference from posterior: The left leg is abducted and externally rotated (opposite of posterior dislocation). - Roberts and Hedges' Clinical Procedures in Emergency Medicine
Complication: Femoral artery or nerve injury (less common than sciatic nerve in posterior dislocations but must be checked).
Imaging
- AP pelvis + AP/lateral hip - first-line; identifies the direction of dislocation
- CT pelvis - mandatory after identifying dislocation to assess for:
- Acetabular fractures
- Femoral head fractures
- Incarcerated intra-articular fragments (which prevent closed reduction)
Management - Orthopedic Emergency
Time to reduction is critical. Risk of avascular necrosis (AVN) of the femoral head:
- <10% when reduced within 6 hours
- Rises to ~25% when delay extends from 10-15 hours
Reduction must occur within 6 hours of injury under procedural sedation (IV) or general anesthesia if needed. Anterior dislocations mandate reduction in the operating room.
Closed Reduction Techniques for Posterior Dislocation
All techniques require in-line traction with hip flexed to 90°:
Allis Technique (most common):
- Patient supine; assistant presses down on the ASIS to stabilize the pelvis
- Operator applies upward traction in line with the deformity, flexing hip to 90°
- Gently internally and externally rotate until reduction occurs
- Can stand on the stretcher to use body weight for leverage
Stimson (Gravity) Technique:
- Patient prone; pelvis overhangs the stretcher edge
- Hip, knee, and ankle flexed to 90°
- Downward pressure applied to the posterior proximal tibia
- Gently rotate internally/externally to facilitate reduction
- Caution: Prone position may be risky in multiply injured patients or those needing deep sedation
Whistler Technique:
- Patient supine, both knees flexed to 130°
- Assistant stabilizes pelvis; operator stands beside the affected limb
- Arm placed under the affected knee; other hand anchors ankle to the stretcher
- Raise the shoulder to elevate the affected knee - the femoral head moves anteriorly around the acetabular rim and relocates
Closed Reduction for Anterior Dislocation
Modified Allis:
- Supine; assistant applies lateral countertraction on the thigh
- Flex hip slightly, apply traction along the long axis of the femur
- Gently adduct and internally rotate to reduce
Reverse Bigelow:
- Hip in partial flexion and abduction
- Apply traction in line with the deformity, then adduct, sharply internally rotate, and extend
- Caution: Risk of femoral neck fracture in osteoporotic bone with sharp rotation
Open Reduction Indications
- Failed closed reduction
- Unsatisfactory reduction
- Irreducible fracture
- Complex fracture-dislocations
Post-Reduction Care
- Confirm reduction with imaging (X-ray and CT)
- Check neurovascular status
- Abduction pillow to maintain position and prevent re-dislocation
- Orthopedic admission and follow-up mandatory
- All anterior dislocations require hospital admission
Complications
| Complication | Notes |
|---|---|
| Avascular necrosis (AVN) | Most feared; risk rises steeply with delay |
| Post-traumatic arthritis | Especially with associated fractures |
| Sciatic nerve injury | ~10% of posterior dislocations; most recover |
| Femoral nerve/artery injury | Rare; associated with anterior dislocations |
| Re-dislocation | Risk with inadequate reduction or associated instability |
Sources: Tintinalli's Emergency Medicine; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Miller's Review of Orthopaedics 9th Edition
This is a shared conversation. Sign in to Orris to start your own chat.