Give me X-ray images of a patient with osteoporosis having femoral neck fracture.
osteoporosis femoral neck fracture X-ray radiograph image
Femoral Neck Fracture in Osteoporosis - X-ray Images
1. Annotated AP Pelvis - Femoral Neck Fracture vs. Normal Side

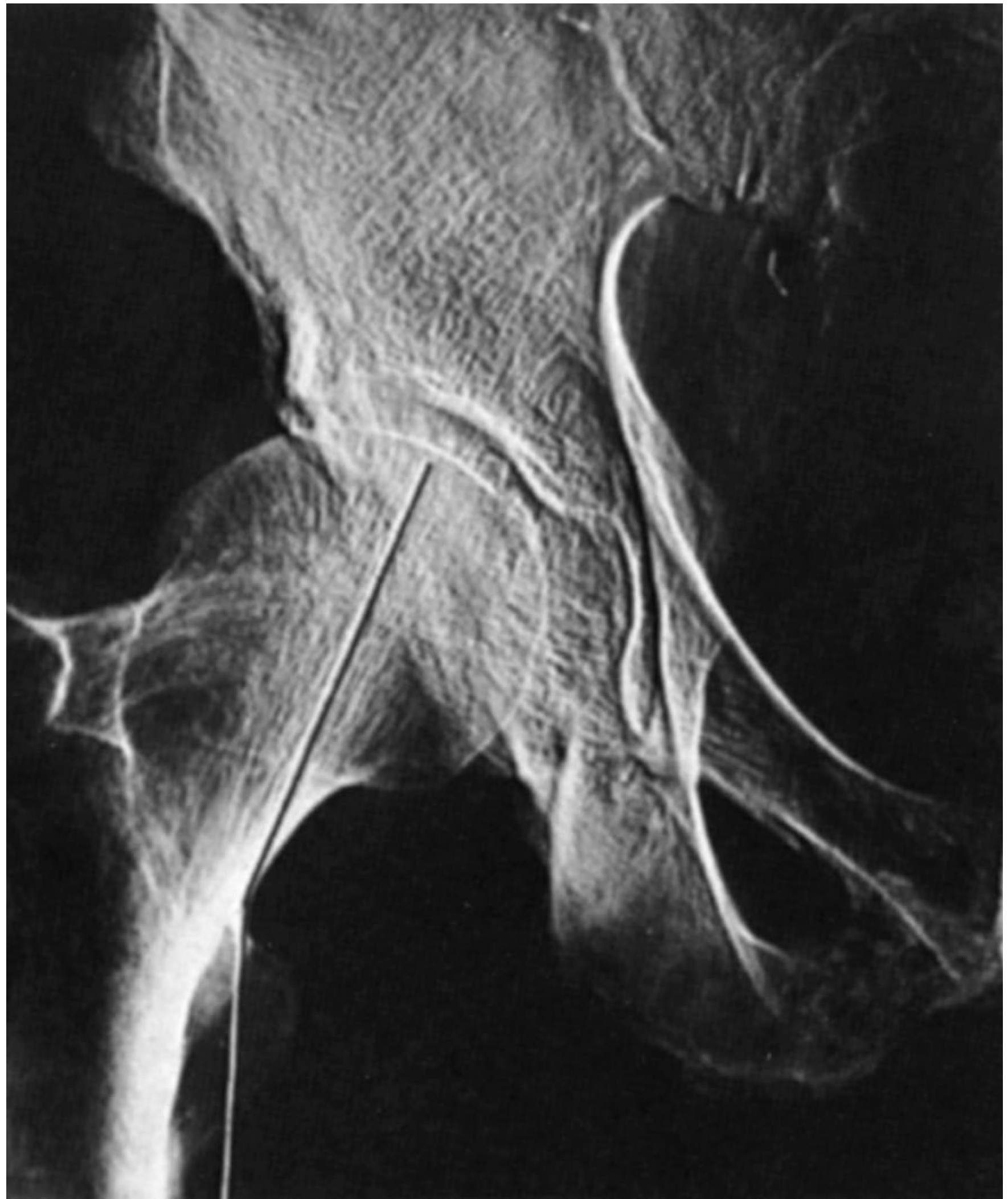
2. Displaced Subcapital Fracture (Textbook X-ray)

3. AP Hip - Displaced Femoral Neck Fracture (Radiopaedia)
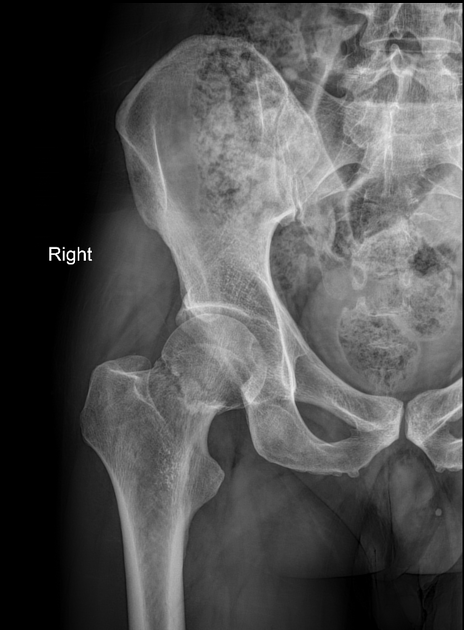
- Reduced bone density (osteoporotic pattern - sparse, coarse trabeculae)
- Loss of Shenton's line
- Varus angulation of the femoral head
- Upward displacement of the femoral shaft relative to the head
4. Fracture Classification Diagram - Sites of Proximal Femoral Fractures
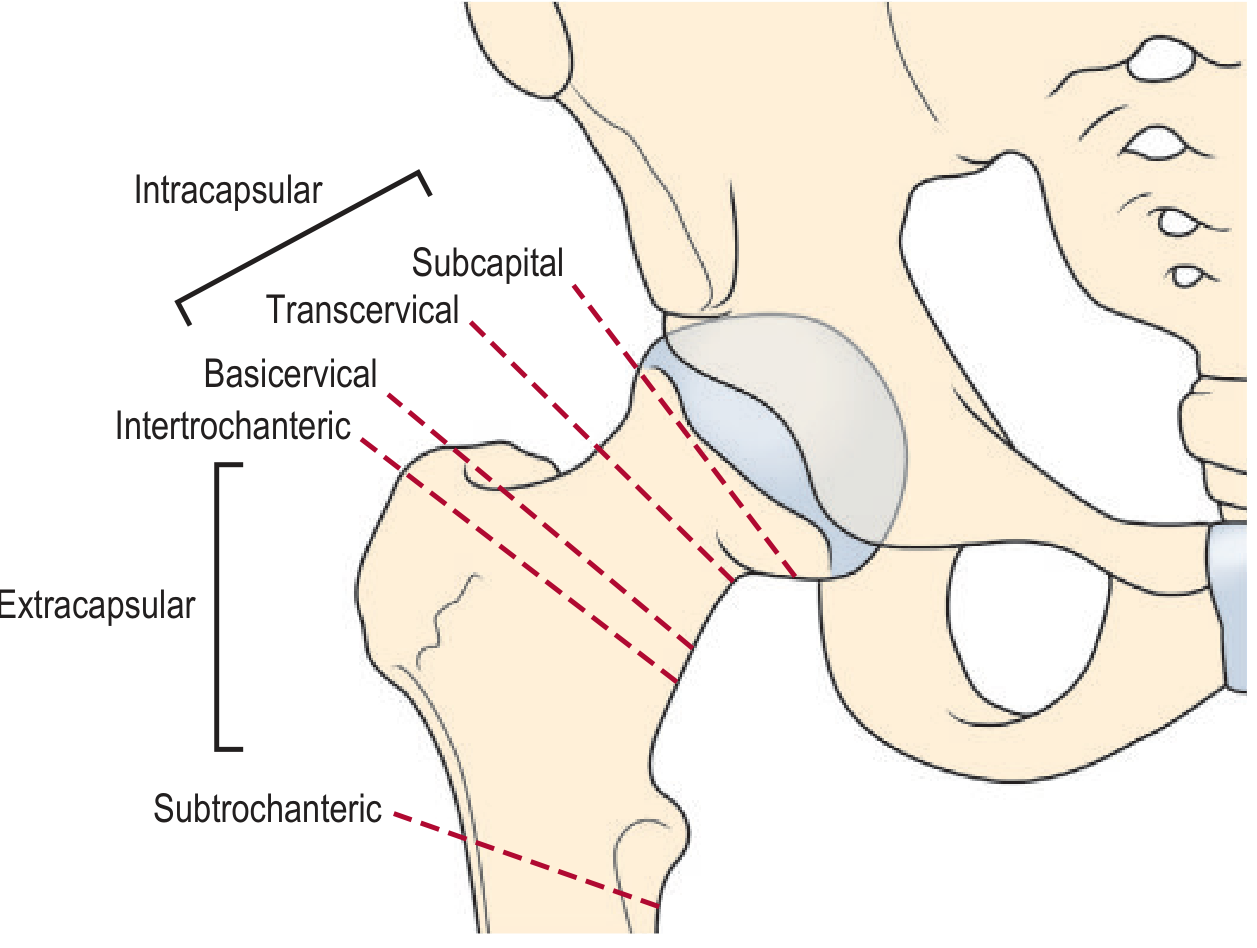
- Intracapsular (highest AVN risk): subcapital, transcervical, basicervical
- Extracapsular (lower AVN risk): intertrochanteric, subtrochanteric
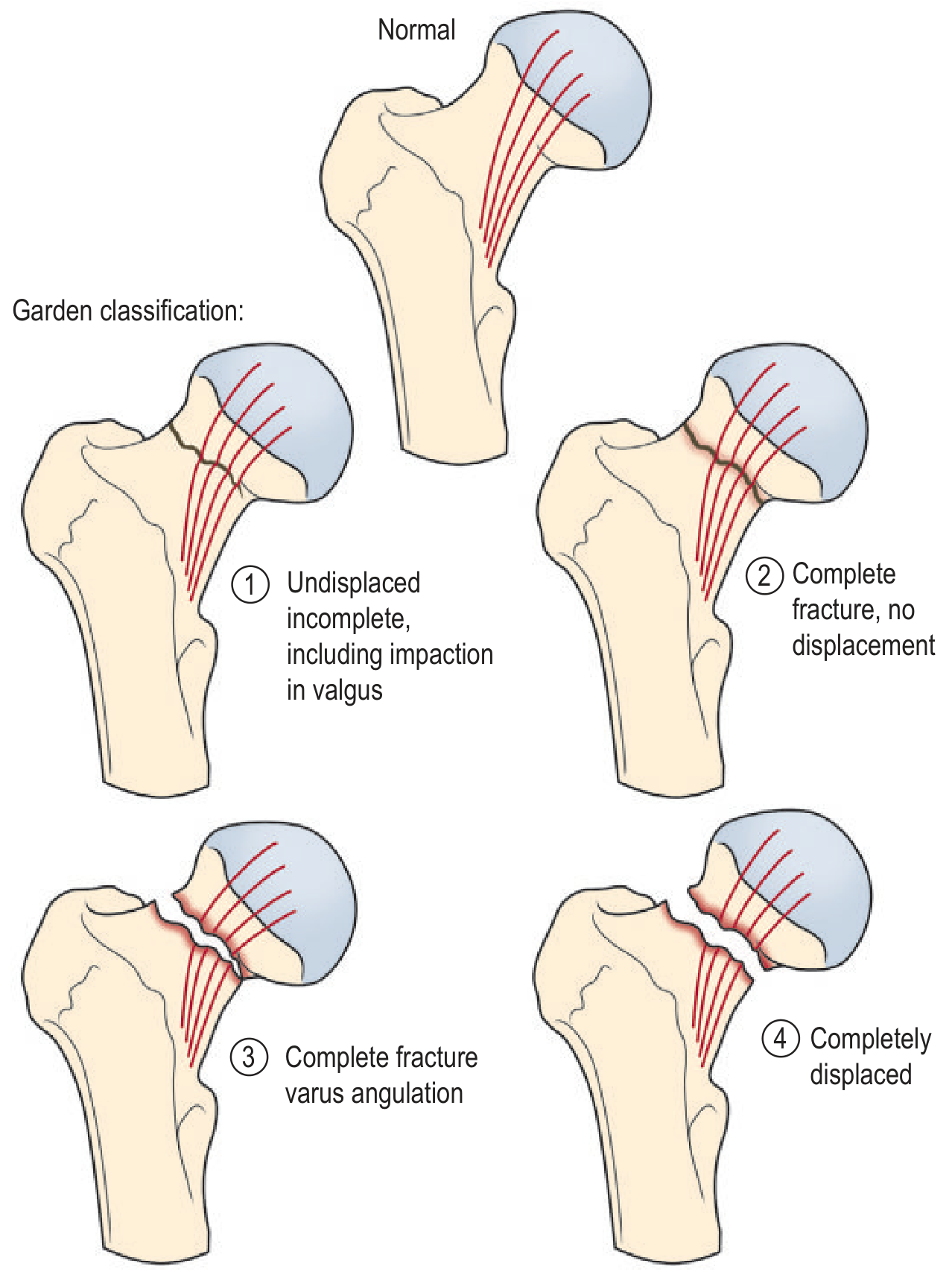
5. Garden Classification of Intracapsular Femoral Neck Fractures
| Grade | Description | AVN Risk |
|---|---|---|
| 1 | Undisplaced/incomplete (valgus impaction) | Low |
| 2 | Complete fracture, no displacement | Low-moderate |
| 3 | Complete fracture, varus angulation | High |
| 4 | Completely displaced | Very high (15-35%) |
Key Radiological Features to Look For in Osteoporosis + Femoral Neck Fracture
- Reduced bone density - diffusely osteopenic appearance (more "see-through")
- Fracture line - may be subtle in undisplaced/impacted fractures; look for a sclerotic/lucent line across the neck
- Loss of Shenton's line - the smooth arc formed by the inferior femoral neck and superior obturator foramen is disrupted
- Shortening and external rotation - of the affected limb on clinical exam
- Trabecular disruption - interruption of the normal trabecular pattern is the key clue for subtle/impacted fractures
Note: Approximately 15% of femoral neck fractures are initially difficult to detect on plain X-ray. If clinical suspicion is high but the X-ray appears normal, CT or MRI is indicated to exclude an occult fracture. - Grainger & Allison's Diagnostic Radiology
operation for this
surgical management femoral neck fracture osteoporosis hemiarthroplasty total hip replacement internal fixation
Surgical Management of Femoral Neck Fracture in Osteoporosis
Decision Algorithm
Femoral Neck Fracture
│
├── Undisplaced (Garden 1 & 2)
│ └── Internal Fixation (cannulated screws / DHS)
│
└── Displaced (Garden 3 & 4)
├── Physiologically OLDER / less active
│ └── Hemiarthroplasty (or THA if community ambulatory)
└── Physiologically YOUNGER (<60 yrs)
└── Internal Fixation (attempt head preservation)
Option 1: Internal Fixation with Cannulated Screws
Technique (Campbell's Operative Orthopaedics, Technique 60.1)
- Patient supine on fracture table; closed reduction using Whitman technique
- Fluoroscopic assessment of reduction quality
- Three partially threaded cannulated screws (6.5, 7.0, or 7.3 mm) inserted in an inverted triangle configuration
- A fourth screw in a diamond configuration when significant comminution is present
- Guide pins placed under fluoroscopy in two planes; screws placed with cortical support in the femoral neck
Diagram - Cannulated Screw Fixation
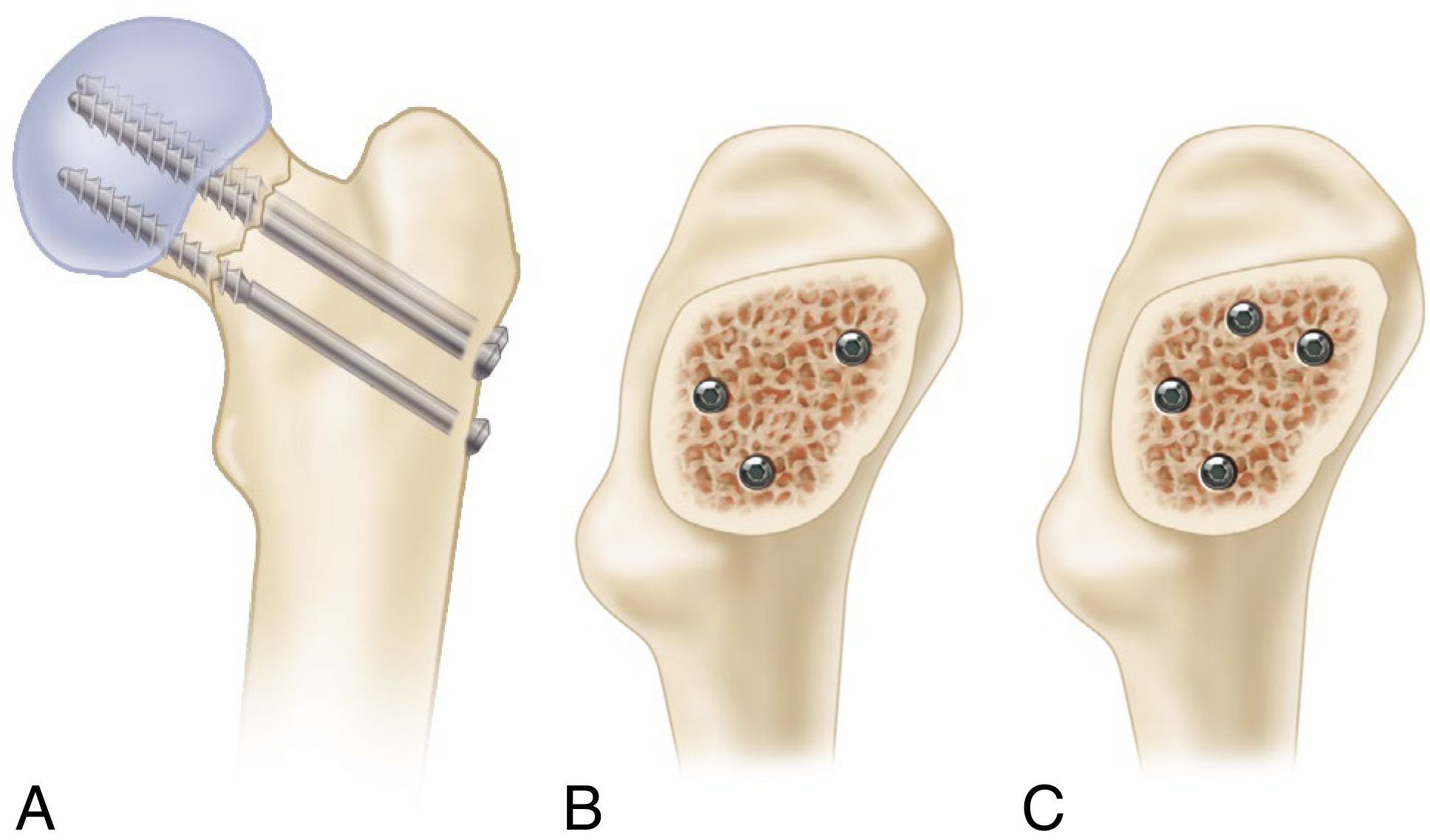
- (A) Side view: screws crossing the fracture line into the femoral head
- (B) Inverted triangle: standard 3-screw configuration (end-on view)
- (C) Diamond: 4-screw configuration for comminuted fractures
Option 2: Dynamic Hip Screw (DHS) / Sliding Hip Screw
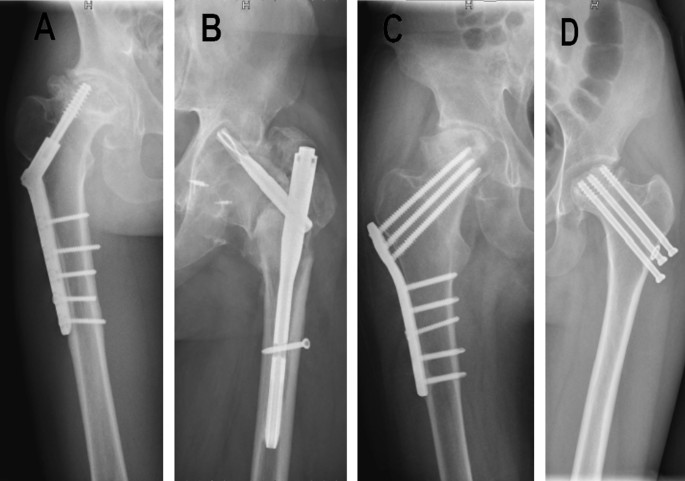
Post-op X-rays showing various fixation devices:
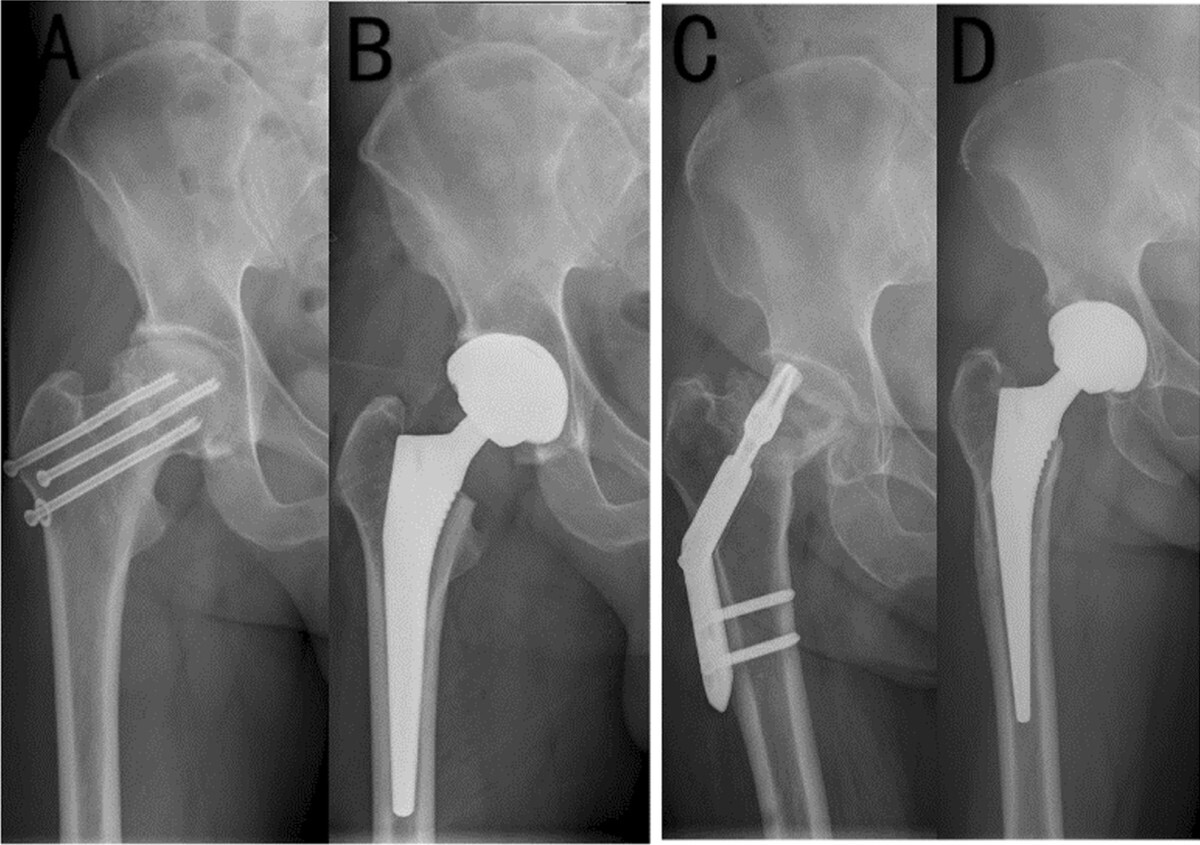
- (A) Cannulated screw fixation - parallel screws in femoral neck
- (B) Hemiarthroplasty - prosthetic femoral head replacing the fractured head
- (C) Dynamic hip screw + side plate
- (D) Total hip arthroplasty (THA)
Option 3: Hemiarthroplasty
Hemiarthroplasty vs THA:
| Feature | Hemiarthroplasty | Total Hip Arthroplasty (THA) |
|---|---|---|
| Acetabulum replaced? | No | Yes |
| Best for | Less active elderly | Active community ambulators |
| Dislocation risk | Lower | Higher (5-10%) |
| Complexity | Less | More |
| Cost | Lower | Higher |
| Revision rate | Similar long-term | Better function long-term |
Unipolar vs Bipolar:
- Unipolar - single fixed articulation; simpler and cheaper
- Bipolar - inner bearing between head and cup; theoretically reduces acetabular wear, though clinical benefit is debated
Cemented vs Cementless:
- Cemented stems are generally preferred in osteoporotic elderly patients - lower rates of periprosthetic fracture and better initial stability in poor-quality bone
Option 4: Total Hip Arthroplasty (THA)
Garden Alignment Index - Intraoperative Assessment
- AP view: angle between medial trabecular stream and femoral shaft should be 160-170°
- Lateral view: angle should be 180° (collinear)
- Angles outside these ranges indicate inadequate reduction and predict failure
Post-op Implant X-rays (Various Fixation Devices)
Summary Table
| Fracture Type | Patient | Preferred Operation |
|---|---|---|
| Undisplaced (Garden 1-2) | Any age | Cannulated screws (3-screw inverted triangle) |
| Displaced (Garden 3-4) | Young (<60 yrs) | Closed reduction + internal fixation |
| Displaced (Garden 3-4) | Elderly, less active | Hemiarthroplasty (cemented) |
| Displaced (Garden 3-4) | Elderly, active ambulator | Total Hip Arthroplasty (THA) |
| Basicervical / Intertrochanteric | Any | Dynamic Hip Screw (DHS) |
Key point in osteoporosis: Bone quality is poor, so internal fixation has a higher failure rate (AVN 15-35%, non-union ~30% in displaced fractures). Arthroplasty is preferred in displaced fractures in elderly osteoporotic patients because it provides immediate stable fixation and allows early full weight-bearing, reducing the risk of prolonged immobility complications (DVT, pressure sores, pneumonia). - Campbell's Operative Orthopaedics, 15th Ed 2026
find recent research papers or guidelines for these operations
"femoral neck fracture"[MeSH Terms] AND "arthroplasty"[MeSH Terms]
"femoral neck fracture"[MeSH Terms] AND "internal fixation"[MeSH Terms]
"hip fracture"[MeSH Terms] AND "guideline"[pt]
femoral neck fracture hemiarthroplasty total hip arthroplasty
femoral neck fracture internal fixation cannulated screws outcome
hip fracture osteoporosis surgical management guidelines
femoral neck fracture dynamic hip screw sliding hip screw outcome
Recent Research Papers & Guidelines: Femoral Neck Fracture Surgery
🏛️ GUIDELINES & POLICY (2024-2026)
1. WHO Benchmarks for Hip Fracture Care & Osteoporosis Treatment (2026)
Evidence Level: Authoritative WHO-linked Review
- ≥50% of patients receive surgery within 48 hours of fracture
- ≥50% of patients receive pharmacological osteoporosis treatment post-fracture
- Fracture Liaison Services (FLS) are evidence-based tools for secondary fracture prevention
- Orthogeriatric co-management models reduce mortality
- Health systems must close data gaps and variability in surgical pathways
- Urgently calls for new national policies tailored to geopolitical contexts
2. Osteosynthesis, Hemiarthroplasty, THA in Hip Fractures: All I Need to Know (2024)
Evidence Level: Practice Guideline / Narrative Review
- National surgical guidelines for hip fractures are established but THA implementation as primary treatment varies widely
- Reviews epidemiology, classification systems, and all three main treatment options
- Emphasizes that THA is increasingly used for active elderly patients but with caveats on dislocation risk
- Supports tailored implant selection based on patient physiology, not age alone
🔩 INTERNAL FIXATION PAPERS (2023-2025)
3. Femoral Neck System (FNS) vs. Cannulated Screws + Medial Plate - Prospective Multicenter RCT (2025)
Evidence Level: Randomized Controlled Trial (165 vs. 166 patients, 2-year follow-up)
| Outcome | FNS | CS + Medial Plate |
|---|---|---|
| Bone union rate | No significant difference | No significant difference |
| Harris Hip Score (3 months) | Higher ✓ | Lower |
| Operation time | Shorter ✓ | Longer |
| Intraoperative blood loss | Less ✓ | More |
| Fluoroscopy frequency | Less ✓ | More |
| Coxa vara incidence | Higher ✗ | Lower |
| 2-year function | No significant difference | No significant difference |
4. Optimal Fixation Strategies for Displaced FNF in Patients 18-59 Years - 26-Center Study (2024)
Evidence Level: Large multicenter comparative cohort (565 patients, 26 Level 1 trauma centers)
- Multiple cannulated screws (MCS): 55% failure rate
- Fixed-angle (FA) constructs: 36% failure rate (p<0.001)
- Best construct: Sliding hip screw + medial femoral neck buttress plate (FNBP) + antirotation screw = only 11% failure rate
Clinical implication: Traditional multiple cannulated screw fixation performs poorly for displaced fractures in young patients. Fixed-angle constructs with medial plate augmentation should be prioritized.
5. FNS vs. Cannulated Screws - Meta-Analysis & Systematic Review (2023)
Evidence Level: Review / Meta-Analysis
6. Systematic Review: Post-Op Outcomes of FNF Interventions (2024)
Evidence Level: Systematic Review (PRISMA) - 68,567 patients across 117 studies
- FNS groups had similar or lower complication rates, reoperations, and mortality vs. cannulated screws, cancellous screws, and DHS groups
- No significant safety difference between FNS and traditional devices
- Calls for more prospective controlled studies to firmly establish FNS superiority
🦴 HEMIARTHROPLASTY vs. THA PAPERS (2023-2025)
7. Hemiarthroplasty vs. THA in Elderly - Medicare Data Analysis (2023)
Evidence Level: Large population-based study (61,695 elderly Medicare patients, 2017-2019)
| Outcome (12 months) | THA | Hemiarthroplasty |
|---|---|---|
| Dislocation rate | 2.9% | 1.9% (p=0.001) |
| Revision/conversion | No significant difference | No significant difference |
- 83.4% received hemiarthroplasty, 16.6% received THA
- THA carries significantly higher dislocation risk at 12 months
- No difference in revision rates between the two
Clinical implication: THA's higher dislocation risk should be factored into patient selection, especially for less active elderly patients.
8. Conversion THA after Failed Internal Fixation - Systematic Review (2025)
Evidence Level: Systematic Review (1,260 patients, 12 retrospective studies)
| Prior Fixation | Dislocation | Periprosthetic Fracture | Aseptic Loosening | Infection | Reoperation |
|---|---|---|---|---|---|
| Intramedullary nail | 6.01% | 3.14% | 2.59% | 3.41% | 3.82% |
| Plate/screw system | Lower overall | 11.57% (highest) | - | - | - |
| Cannulated screws | 10.04% (highest dislocation) | Lower | - | - | - |
Key finding: Conversion THA carries elevated complications regardless of prior fixation method. Surgeons should counsel patients about this before choosing initial fixation strategy.
Summary Table: Best Evidence by Procedure
| Procedure | Best Recent Evidence | Key Message |
|---|---|---|
| Cannulated screws | Roser 2024 (PMID 39007655) | 55% failure in displaced FNF; supplement with medial buttress plate + AR screw to reduce to 11% |
| FNS (Femoral Neck System) | Wen 2025 RCT (PMID 40457366); Sheffels 2024 SR (PMID 39554300) | Faster, less blood loss, equivalent union; slightly more coxa vara |
| Hemiarthroplasty vs. THA | Edelstein 2023 (PMID 37678258) | THA has higher dislocation risk (2.9% vs. 1.9%); similar revision rates |
| Conversion THA after fixation failure | Di Martino 2025 SR (PMID 40956324) | High complication rates; worst dislocation risk after cannulated screw fixation |
| Global guidelines | WHO 2026 (PMID 41198933); Ridha 2024 guideline (PMID 38324951) | Surgery within 48h; start osteoporosis treatment post-fracture; orthogeriatric co-management |