Snake bite in India diagnosis management and treatment with image reference
Reading File
Finding Sources
Finding Sources
Searching the Web
snake bite India diagnosis management treatment guidelines 2024
Searching PubMed
"snakebite" AND "India" AND "management"
Reading File
Reading File
Reading File
Reading Web Page
snake bite India diagnosis management antivenom treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to write a detailed, well-illustrated answer. Let me compile everything.
Snake Bite in India: Diagnosis, Management & Treatment
Epidemiology
India has one of the highest snakebite burdens in the world. At least 45,000 people die annually following snakebites in India alone - more than anywhere else globally. Snakebite is predominantly an occupational disease of rural agricultural workers, with seasonal peaks during rice planting and harvesting. Despite this toll, it remains a neglected public health issue. An estimated 15,000-30,000 deaths occur annually in Pakistan and India combined.
- India has ~216 snake species, of which 52 are venomous
- Only 50% of bites by venomous species result in actual envenomation
- 70% of all snakebites are from non-venomous snakes
The "Big Four" Medically Important Snakes in India
The Indian Polyvalent Anti-Snake Venom (PAV) covers the four most clinically significant species:
1. Common Cobra (Naja naja) - Elapidae
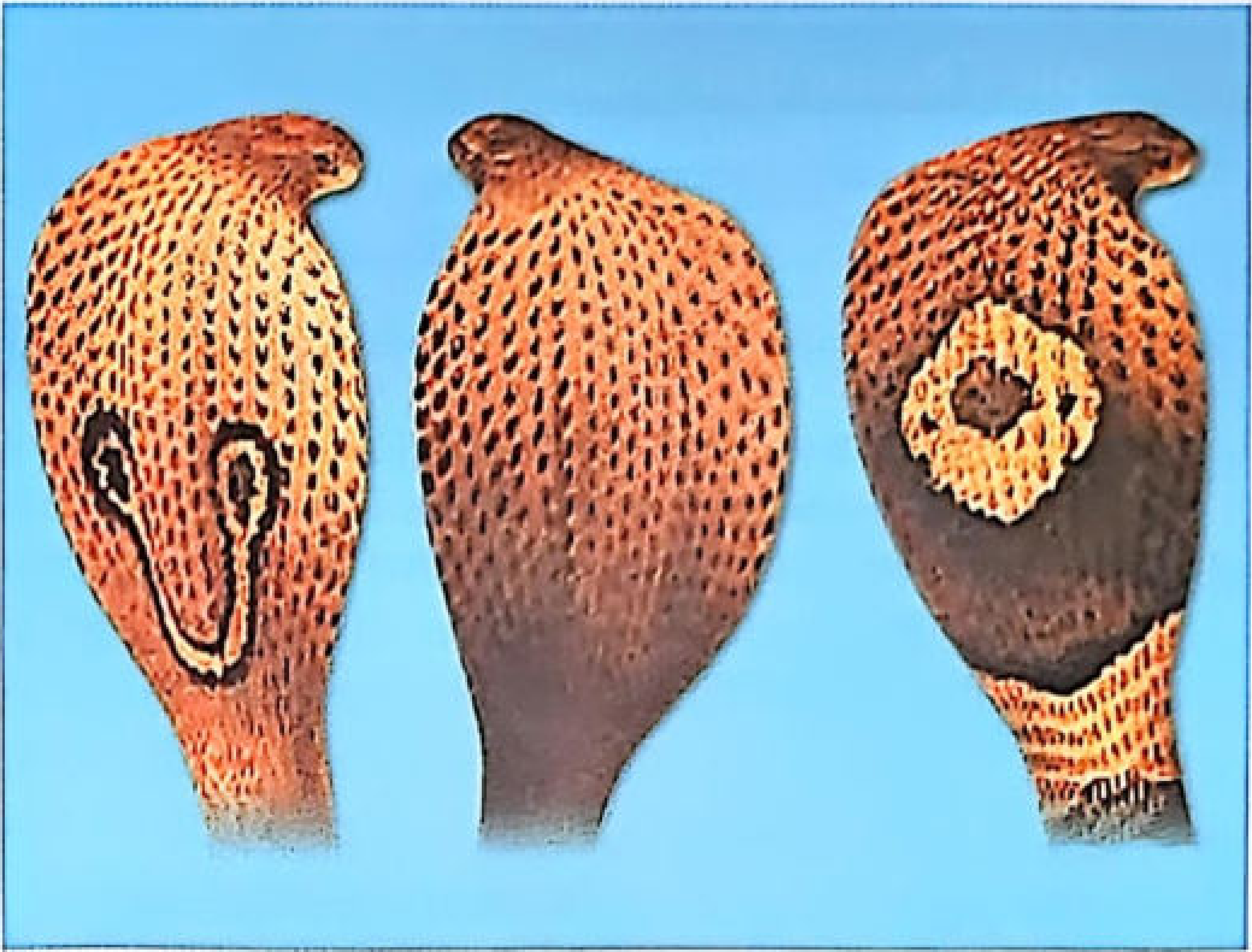
Fig. 32.1: Cobra hood patterns - Binocellate (1), Black (2), Monocellate (3) - from KS Narayan Reddy's Essentials of Forensic Medicine & Toxicology
- Spectacle mark on dorsal hood (binocellate/monocellate)
- Large head scales; round pupil; grooved, short fangs
- Three varieties: N. naja (most of India), N. kaouthia (Bengal, Odisha, UP), N. oxiana (J&K, Punjab, Rajasthan)
- Venom: Neurotoxic (postsynaptic alpha-neurotoxin)
2. Common Krait (Bungarus caeruleus) - Elapidae

Fig. 32.2: Common Krait (Bungarus caeruleus) - from KS Narayan Reddy's Essentials of Forensic Medicine & Toxicology
- Steel-blue, 1.0-1.5 m; single or double white bands across back
- Key ID: hexagonal scales in central row; entire (undivided) subcaudal plates
- Nocturnal; found throughout India; bites sleeping victims
- The most common venomous snake in India
- Venom: Neurotoxic (presynaptic beta-neurotoxin - blocks ACh release; harder to reverse with neostigmine)
3. Banded Krait (Bungarus fasciatus)

Fig. 32.3: Banded Krait - from KS Narayan Reddy's Essentials of Forensic Medicine & Toxicology
- Jet black 5cm-wide bands alternating with deep yellow bands; 1.5-2 m
- Found in Bengal, Odisha, MP, Andhra, Assam
4. Russell's Viper (Daboia russelii) - Viperidae
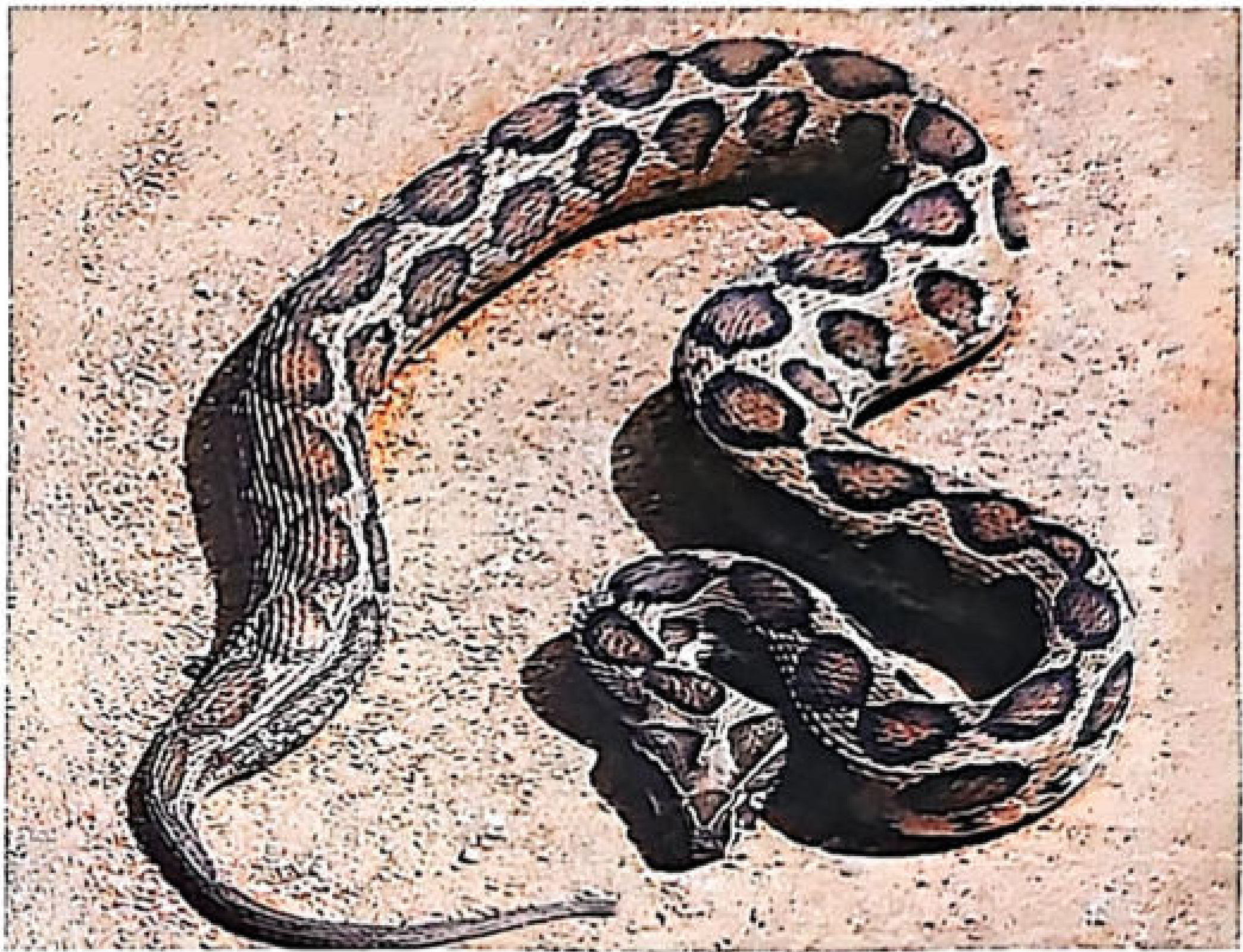
Fig. 32.4: Russell's Viper (Daboia russelii) - from KS Narayan Reddy's Essentials of Forensic Medicine & Toxicology
- Flat, heavy triangular head; V-shaped mark pointing forwards
- Three rows of diamond-shaped black/brown spots; whitish body with dark semilunar spots
- Short, tapering tail; hisses loudly; found throughout India
- Venom: Hemotoxic/cytotoxic + some neurotoxicity (especially in South India/Sri Lanka)
5. Saw-Scaled Viper (Echis carinatus)
- Brown, ~0.5 m; triangular head; wavy white lines on flanks with diamond-shaped areas between
- White mark on top of head resembling a bird's footprint
- Found throughout India
- Venom: Hemotoxic (potent pro-coagulant)
Cobra vs. Viper - Key Differences
| Trait | Cobra (Elapid) | Viper |
|---|---|---|
| Body | Long, cylindrical | Short, narrow neck |
| Head | Small, large shields | Large, triangular, small scales |
| Pupil | Round | Vertical (elliptical) |
| Fangs | Grooved, short, fine | Canalized, long, folding |
| Venom | Neurotoxic | Hemotoxic |
| Tail | Round | Tapering |
| Reproduction | Lay eggs | Give birth to young |
Venom Composition & Mechanisms
Elapid venoms (Cobra, Krait):
- Postsynaptic neurotoxins (cobra): block nicotinic ACh receptors - partially reversible with neostigmine
- Presynaptic neurotoxins (krait beta-bungarotoxin): prevent ACh release at nerve terminals - largely irreversible with neostigmine
Viperid venoms (Russell's viper, Saw-scaled viper):
- Rich in proteases, phospholipases, and procoagulant enzymes
- Cause venom-induced consumption coagulopathy (VICC)
- Russell's viper also contains phospholipase A2 causing rhabdomyolysis and AKI
Clinical Features
Local Envenoming
Seen predominantly with Viperidae and some Elapidae (Asian cobras):
- Fang marks (may be single or paired); persistent bleeding from fang marks = coagulopathy
- Local swelling starting within minutes (Viperidae) - can involve entire limb + adjacent trunk within days
- Linear erythema/bruising along lymphatics; tender lymphadenopathy
- Blisters (serous or haemosanguinous), bullae, ecchymosis
- Necrosis in 10-15% of viper bites - skin, subcutaneous tissue, muscle
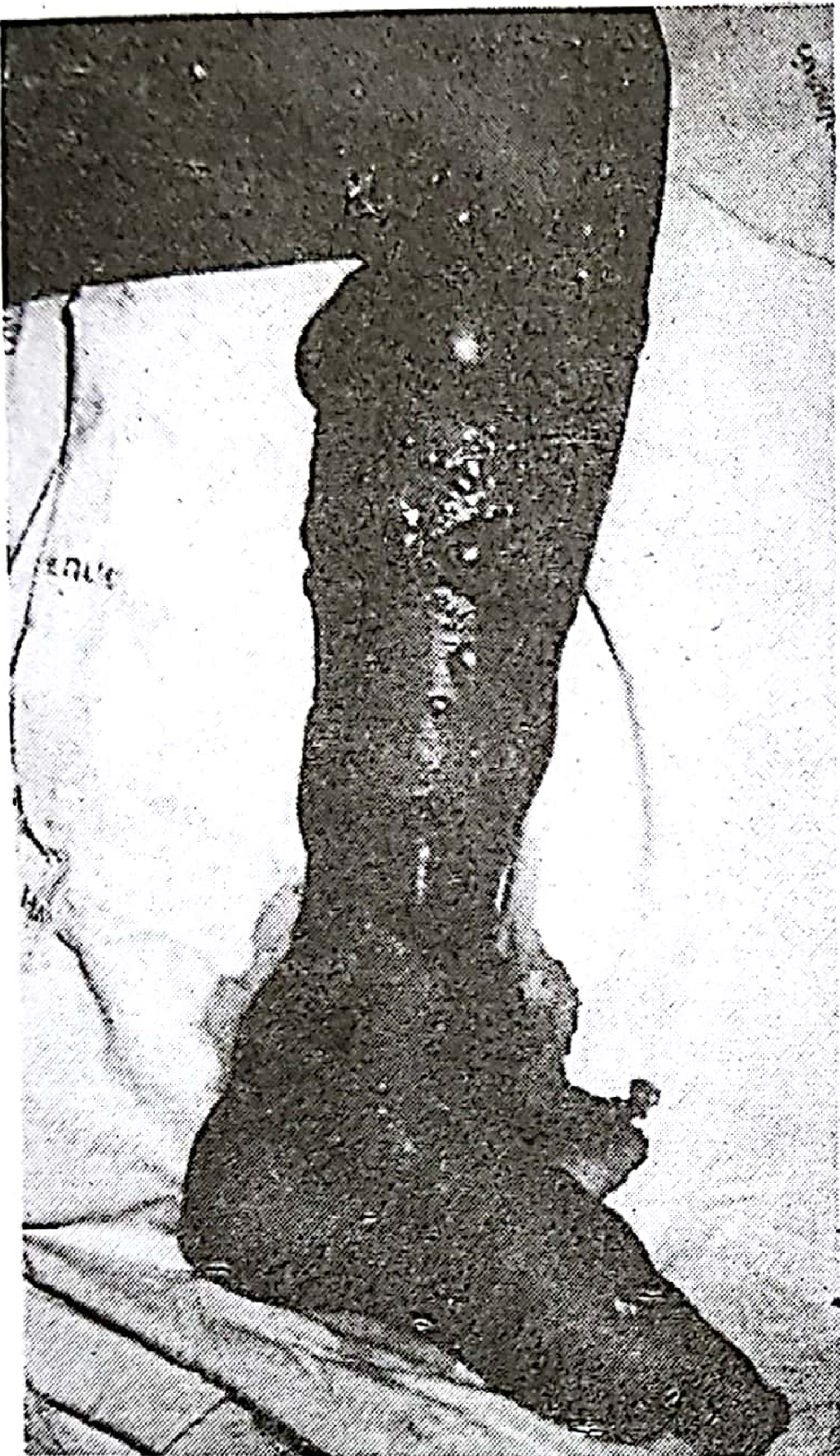
Severe local envenoming - extensive blistering and tissue destruction from viper bite - Pye's Surgical Handicraft
Krait bite: Virtually no local signs - bite may not wake a sleeping victim; no significant swelling or burning pain
Systemic Envenoming
Neurotoxic (Cobra/Krait):
- Ptosis (earliest sign) → ophthalmoplegia → dysarthria → dysphagia
- Descending paralysis - inability to raise head ("broken neck sign")
- Respiratory failure (cause of death)
- Patient conscious but unable to speak; coma then respiratory arrest
- Cobra: drowsiness/heavy eyelids, + possible cardiac toxicity
- Krait: intense drowsiness/intoxication; albuminuria
Hemotoxic/Cytotoxic (Russell's viper, Saw-scaled viper):
- Severe pain at bite site within 8 minutes; redness
- Persistent bleeding from bite + other sites (gums, epistaxis, hemoptysis, hematuria)
- Prolonged bleeding/clotting time; DIC
- Epistaxis, hemoptysis, ecchymoses, intracranial haemorrhage, GI/GU bleeding
- Renal failure (myoglobinuria, hemolysis, direct tubular toxicity) - "mahogany-coloured" urine
- Hypotension, shock in severe cases
- In some regions, Russell's viper also causes neurotoxicity + pituitary haemorrhage (Sheehan-like syndrome)
Early Warning Signs of Severe Envenoming (WHO criteria):
- Snake identified as very dangerous species
- Rapid early extension of local swelling from bite site
- Early tender enlargement of regional lymph nodes
- Collapse (hypotension, shock), severe nausea/vomiting, diarrhoea
- Heavy eyelids/inappropriate drowsiness; early ptosis/ophthalmoplegia
- Early spontaneous systemic bleeding from any site
- Dark brown/black urine (myoglobinuria/haemoglobinuria)
Diagnosis
Clinical Assessment
- History: time, circumstances, snake description, symptom progression
- Examine fang marks, local swelling extent, lymphadenopathy
- Neurological exam: ptosis, eye movements, reflexes, respiratory effort
- Watch for bleeding from gums, injection sites, venepuncture sites
Key Bedside Test: 20-Minute Whole Blood Clotting Test (20WBCT)
This is the single most important test in Indian settings where coagulation labs may not be available:
- Take a few mL of fresh venous blood in a clean dry glass tube
- Leave undisturbed for 20 minutes, then gently tilt
- If blood is still liquid = incoagulable = viper bite with VICC
- Repeat every 6 hours to determine repeat dose requirement
- Normalization of clotting = endpoint of therapy
- After normalization, repeat at 12-hour intervals for 48 hours to detect recurrence
Laboratory Investigations
| Test | Purpose |
|---|---|
| 20WBCT | Bedside coagulation screen (viper bite) |
| PT/INR, aPTT, fibrinogen | Coagulopathy assessment |
| Platelet count | DIC monitoring |
| CBC, blood film | Haemolysis, anaemia |
| Serum creatinine, urea | Renal function |
| Urine examination | Haematuria, proteinuria, myoglobinuria |
| CK, LDH | Rhabdomyolysis |
| ECG | Cardiac involvement |
| Serum electrolytes | K+ (hyperkalaemia in rhabdomyolysis) |
Note: Monovalent ASV is not available in India. Venom Detection Kits (VDK) are not routinely available. Species identification relies on clinical features and snake description.
Management
First Aid (Community/Pre-Hospital)
Recommended (Government of India National Protocol):
- Reassure the patient - fear/anxiety worsen symptoms
- Immobilize the bitten limb with a splint/sling - prevent muscular movement that enhances venom absorption
- Transport quickly, comfortably and passively to hospital
- Remove rings, bracelets, watches, tight footwear from bitten limb
- If snake identified as neurotoxic elapid - apply pressure immobilization bandage (firm crêpe bandage from bite site upward, do not occlude circulation)
- Recovery position (left lateral) to protect airway
Absolutely Do NOT:
- Apply tight tourniquets or constricting bands (dangerous, do not work)
- Incise, cut, suck, cauterize or excise the bite site
- Apply ice packs, electric shocks, or herbal remedies
- Give alcohol or stimulants (vasodilators - speed venom absorption)
- Elevate the bitten extremity (hastens systemic absorption)
Hospital Assessment: Critical vs. Non-Critical Arrival
Critical Arrival - any of these signs of systemic envenomation:
- Descending paralysis, ptosis, respiratory distress
- Spontaneous bleeding
- Hypotension/shock
- Dark urine
- Incoagulable blood (20WBCT positive)
All patients should be observed for a minimum of 24 hours. Exceptions only if snake is reliably identified as non-venomous.
Anti-Snake Venom (ASV) - The Definitive Treatment
Indian Polyvalent ASV (PAV)
Prepared by hyperimmunizing horses against the four common Indian venomous snakes. Each 1 mL of PAV neutralizes:
- 0.60 mg dried Indian Cobra (Naja naja) venom
- 0.45 mg dried Common Krait (Bungarus caeruleus) venom
- 0.60 mg dried Russell's Viper (Daboia russelii) venom
- 0.45 mg dried Saw-Scaled Viper (Echis carinatus) venom
Each vial neutralizes approximately 6-8 mg of venom (half-life ~90 hours).
Produced at: Haffkine Institute (Mumbai), King Institute (Chennai), Serum Institute (Pune), and Kasauli (Himachal Pradesh).
Important: No monovalent or species-specific ASV is commercially available in India. Sea snake and pit viper-specific ASV is also unavailable, though the polyvalent may have some cross-reactivity.
Indications for ASV
ASV should be given when ANY of the following are present:
- Rapidly developing swelling involving at least half the bitten limb within a few hours
- Swelling crossing a joint within 1-2 hours of onset
- Incoagulable blood (20WBCT positive) or spontaneous systemic bleeding
- Signs of neurotoxicity (ptosis, ophthalmoplegia, respiratory distress)
- Cardiovascular abnormalities (hypotension, arrhythmia)
- Dark brown/black urine (myoglobinuria)
- Rapidly developing severe local necrosis
Note: Purely localized swelling with or without bite marks alone is NOT an indication for ASV.
ASV Dosing (Indian Standard Guidelines)
| Severity | Dose |
|---|---|
| Minimal (local swelling, no systemic reaction) | 5 vials |
| Moderate (swelling beyond bite site + systemic reaction) | 10 vials |
| Severe (marked local reaction + severe symptoms) | 10-15 vials |
Children require the same dose as adults (not weight-based, since children receive a proportionally larger venom load).
Administration:
- Lyophilized powder dissolved in 500 mL normal saline/distilled water
- IV infusion over 1 hour
- For neurotoxic poisoning: second dose of 10 vials after 1 hour if no improvement
- For hemotoxic: repeat dose after 6 hours if 20WBCT remains incoagulable (liver needs 6 hours to restore clotting factors)
- Most effective if given within 4 hours; less effective at 8 hours; doubtful after 24 hours (though still indicated if systemic envenomation persists)
Test dose of ASV should NOT be given - it is a poor predictor of early anaphylactoid reactions and may presensitize the patient.
Managing ASV Reactions
At first signs of urticaria, itching, shivering, chills, nausea, hypotension, bronchospasm, angioedema:
- Stop ASV infusion immediately
- Adrenaline 0.5 mg IM (1:1000) for adults; 0.01 mg/kg for children
- Hydrocortisone IV + antihistamine for longer protection
- If no improvement in 10-15 minutes: second dose of adrenaline
- Restart ASV infusion once condition improves
Specific Management by Snake Type
Neurotoxic (Cobra/Krait Bite)
- ASV as above
- Airway management is paramount - monitor respiratory rate and SpO2 continuously
- If SpO2 <90%: mechanical ventilation required
- Neostigmine test (for postsynaptic neurotoxicity - primarily cobra):
- Adults: neostigmine 1.5 mg IM + atropine 0.6 mg IV
- Children: neostigmine 0.04 mg/kg + atropine 0.05 mg/kg
- Repeat twice at 10-minute intervals; if improvement shown, continue neostigmine 0.5 mg IM half-hourly + atropine
- Primarily useful for cobra bites (postsynaptic block); less effective for krait (presynaptic)
- "Broken neck sign" (inability to raise head) may persist 3-5 days despite ASV - does not indicate treatment failure
Hemotoxic (Russell's Viper/Saw-Scaled Viper Bite)
- Monitor 20WBCT every 6 hours
- ASV: repeat if 20WBCT still positive at 6 hours
- Fresh whole blood or FFP if severe bleeding (blood bank ASV cannot undo damage already done)
- Monitor renal function closely - snakebite accounts for >70% of AKI in some South Asian regions
- Manage hypotension: IV fluids, plasma expanders; dopamine 2.5-5 mcg/kg/min for refractory shock
- Dialysis (peritoneal or haemodialysis) if oliguria fails to respond to conservative management
- Heparin is NOT effective and may worsen bleeding - never use in snakebite
- Antifibrinolytic agents are NOT effective
Renal Failure (Common with Russell's Viper)
- Maintain hydration; cautious rehydration + diuretics + low-dose dopamine for oliguria
- Peritoneal dialysis or haemodialysis when uraemia develops
- Monitor for hyperkalaemia (from rhabdomyolysis)
Surgical Management
- Early surgery is generally NOT recommended in the acute phase, especially in coagulopathic/hypotensive patients
- Fasciotomy is controversial and rarely needed; measure compartment pressures before performing (most "compartment syndrome" signs are from the envenoming itself, not true elevated pressures)
- Blisters and bullae: leave intact; aspirate only if large and at risk of rupture (fine needle aspiration)
- Wound care: prophylactic antibiotics (penicillin or erythromycin; add gentamicin or cefuroxime if wound was tampered with); tetanus toxoid booster
- Debridement: indicated at earliest signs of established necrosis; requires adequate anaesthesia (tissue damage often far more extensive than surface appearance suggests)
- Split-skin grafting recommended immediately after debridement
- Amputation: last resort; every effort should be made to preserve limb
Complications
| System | Complication |
|---|---|
| Respiratory | Neuromuscular respiratory failure (elapid) |
| Renal | AKI - most common cause of death with viper bites |
| Hematologic | DIC, bleeding from all sites |
| Neurological | Persistent paralysis, pituitary haemorrhage (Russell's viper) |
| Local | Compartment syndrome, necrosis, gangrene, secondary infection |
| Surgical | Keloid formation, chronic ulcers (risk of malignant change after 8+ years) |
| Ophthalmologic | Cobra venom in eyes - spitting cobras (irrigate with water/saline immediately) |
Referral Criteria
Transfer to tertiary centre if:
- Requiring mechanical ventilation
- AKI needing dialysis
- Refractory shock
- Severe coagulopathy/haemorrhage
- Extensive necrosis requiring advanced surgical management
Prevention
- Wear boots and protective clothing in agricultural fields
- Use a torch when walking at night
- Sleep on raised beds (not on floor, especially in krait territory)
- Do not reach into dark holes or under logs
- Snake-bite should be made a notifiable disease in India
- Snakebite programme: standard treatment guidelines, training, adequate ASV supply at all health levels
Sources:
- KS Narayan Reddy's Essentials of Forensic Medicine & Toxicology, 36th Ed. (2026)
- Pye's Surgical Handicraft, 22nd Ed.
- Park's Textbook of Preventive & Social Medicine
- Goldman-Cecil Medicine, International Ed.
- NHM India Standard Treatment Guidelines - Snakebite
- India National Action Plan for Snakebite Envenoming (NAPSE)
- Bhaumik S et al. Core outcome set for snakebite envenomation in South Asia. Inj Prev 2026 [PMID: 39266207]
This is a shared conversation. Sign in to Orris to start your own chat.