Spinopelvic harmony for 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have all the key information needed for a comprehensive 10-mark answer on spinopelvic harmony. Let me compile this.
Spinopelvic Harmony
Spinopelvic harmony (also called sagittal balance or spinopelvic alignment) refers to the optimal relationship between the lumbar spine and the pelvis in the sagittal plane, such that the body maintains an upright posture with minimal muscular energy expenditure.
Key Spinopelvic Parameters
Three angular measurements define spinopelvic alignment:
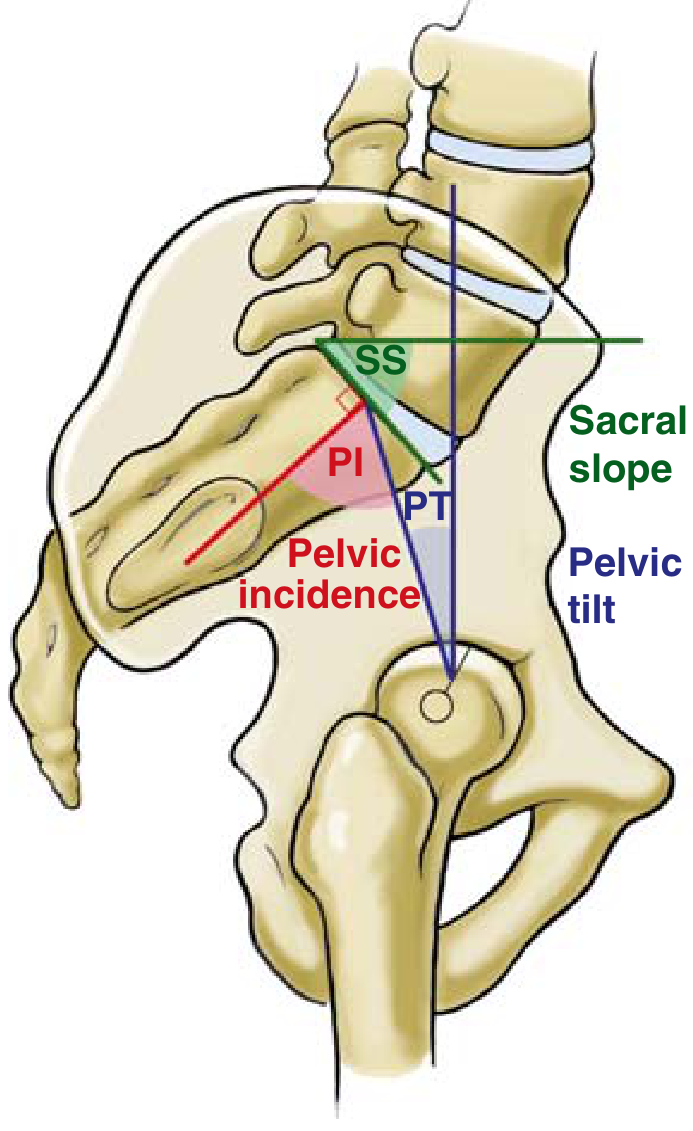
FIG. 3.33 — Miller's Review of Orthopaedics, 9th Ed.
1. Pelvic Incidence (PI)
- Definition: The angle between a line drawn perpendicular to the midpoint of the sacral end plate and a line connecting that same midpoint to the centre of the femoral heads.
- Normal: ~50°
- Key property: Morphological — fixed, unaffected by posture. It is anatomically determined and does not change with body position.
- Formula: PI = PT + SS (this is the fundamental equation of spinopelvic harmony)
2. Sacral Slope (SS)
- Definition: The angle between a line parallel to the sacral end plate and the horizontal reference line.
- Positional parameter — changes with posture.
- Represents the inclination of the sacrum relative to horizontal.
- High SS → pelvis is anteverted → promotes lumbar lordosis.
- Low SS → pelvis is retroverted → flattens lumbar lordosis.
3. Pelvic Tilt (PT)
- Definition: The angle between a line from the midpoint of the sacral end plate to the centre of the femoral heads and a vertical reference line.
- Positional parameter — changes with posture.
- Represents degree of pelvic retroversion (backward rotation).
- High PT → pelvis retroverting as a compensatory mechanism.
- Normal PT: ~12–15°.
The Core Equation: PI = PT + SS
Since PI is fixed by anatomy:
- When the pelvis rotates anteriorly → SS ↑, PT ↓
- When the pelvis rotates posteriorly → SS ↓, PT ↑
- PI remains constant throughout
Spinopelvic Harmony: The Concept
Harmony exists when lumbar lordosis (LL) is appropriately matched to pelvic incidence:
LL ≈ PI ± 9° (Ideal lumbar lordosis = PI − 9° to PI + 9°)
- A patient with a high PI requires more lumbar lordosis to maintain balance.
- A patient with a low PI requires less.
- If LL < PI − 9° → lordosis deficiency → flat-back deformity, forward tilt of the trunk, compensatory hip extension and knee flexion.
- If LL > PI + 9° → excess lordosis → hyperlordotic posture.
Compensatory Mechanisms When Harmony Is Lost
When spinopelvic mismatch occurs (e.g., loss of lumbar lordosis in degenerative flat-back), the body compensates in sequence:
| Mechanism | Description |
|---|---|
| Pelvic retroversion | ↑ PT (pelvis tilts backward) to push sacrum horizontal |
| Hip extension | Extends hips to shift CoM posteriorly |
| Knee flexion | Compensates for forward lean |
| Thoracic hypokyphosis | Reduces upper-trunk forward projection |
| Cervical hyperextension | Final compensation to maintain horizontal gaze |
These compensatory mechanisms come at a high energy cost and eventually lead to pain and disability.
Clinical Relevance
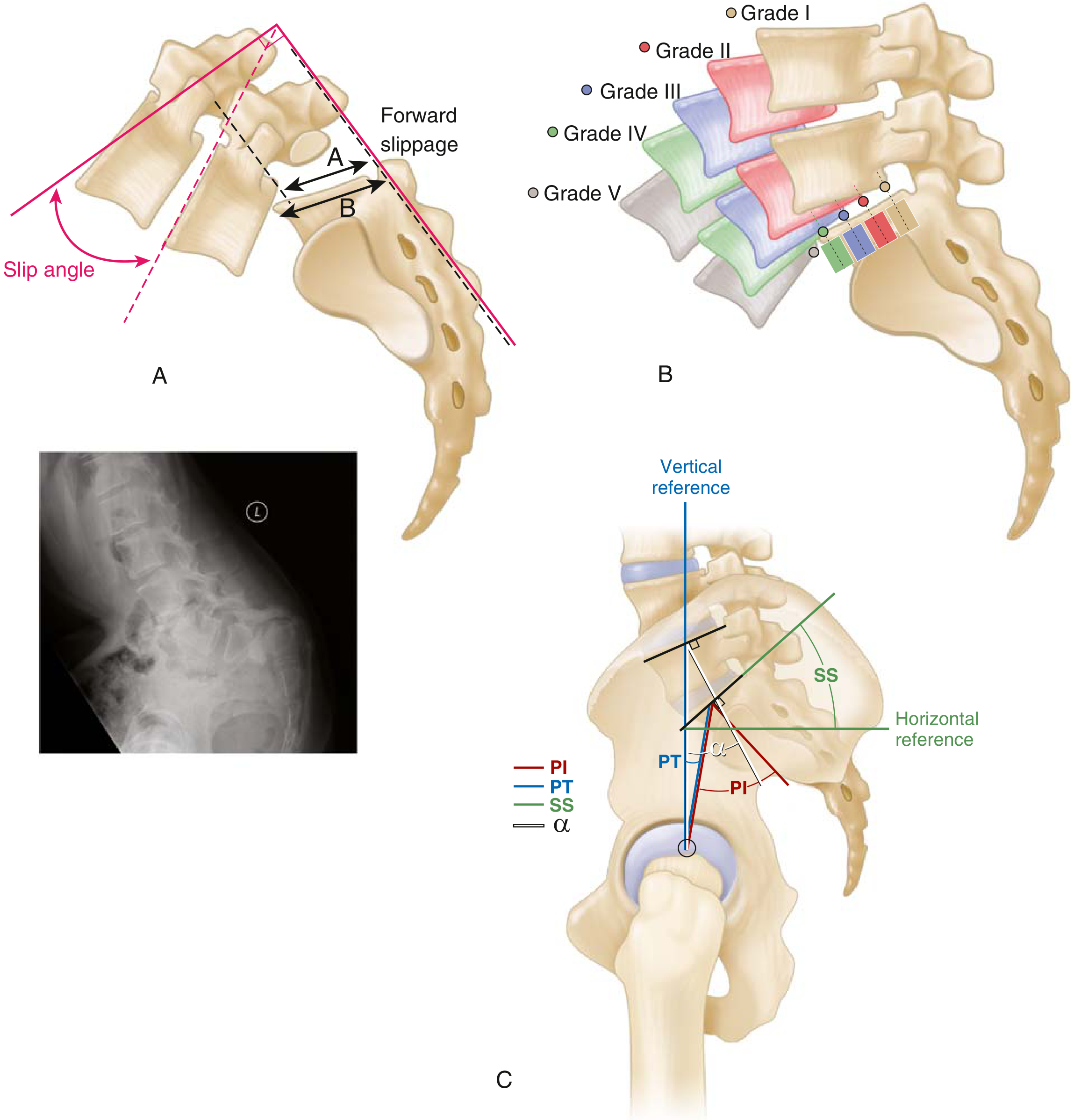
1. Spondylolisthesis
- Increased PI predisposes to spondylolisthesis (especially isthmic type at L5–S1).
- High PI → high sacral slope → increased shear forces at L5–S1 pars interarticularis.
- The slip angle (angle between superior end plate of L5 and a perpendicular to the posterior sacrum) correlates with instability; >45–50° is associated with increased risk of pseudarthrosis and progression.
- The L5 incidence angle (α angle) — line from midpoint of upper L5 end plate to centre of femoral heads, subtended against a perpendicular to the upper L5 end plate — guides surgical planning.
2. Adult Spinal Deformity / Sagittal Imbalance
- Goal of corrective surgery is to restore PI − LL < 10°.
- Failure to restore harmony results in poor surgical outcomes, proximal junctional kyphosis, and implant failure.
3. Total Hip Arthroplasty (THA)
- Pelvic tilt affects acetabular cup orientation; spino-pelvic alignment must be assessed pre-operatively to optimise cup anteversion and reduce dislocation risk.
Summary Table
| Parameter | Type | Measurement | Normal Value |
|---|---|---|---|
| Pelvic Incidence (PI) | Morphological (fixed) | Perpendicular to sacral end plate ↔ line to femoral head centre | ~50° |
| Sacral Slope (SS) | Positional | Sacral end plate vs. horizontal | ~40° |
| Pelvic Tilt (PT) | Positional | Sacral midpoint–femoral head line vs. vertical | ~12–15° |
| Lumbar Lordosis (LL) | Spinal | L1 to S1 Cobb angle | ~50–60° |
Formula: PI = PT + SS | Harmony: LL ≈ PI ± 9°
— Miller's Review of Orthopaedics, 9th Edition | Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3
Spinopelvic harmony with its application in Orthopedics with appropriate illustrative diagrams for 10 marks
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Spinopelvic Harmony and its Applications in Orthopedics (10 marks)
Definition
Spinopelvic harmony is the balanced sagittal relationship between spine and pelvis that allows upright posture, horizontal gaze, and energy-efficient standing/walking.
It is assessed by spinopelvic parameters and their relation to lumbar lordosis.
It is assessed by spinopelvic parameters and their relation to lumbar lordosis.
Core Spinopelvic Parameters
-
Pelvic Incidence (PI)
- Angle between:
- line perpendicular to midpoint of sacral end plate, and
- line from sacral midpoint to center of femoral heads.
- Morphologic parameter, largely constant for an individual.
- Mean around 50°.
- Angle between:
-
Pelvic Tilt (PT)
- Angle between line from sacral midpoint to femoral head center and vertical.
- Positional parameter; rises with pelvic retroversion (compensation).
-
Sacral Slope (SS)
- Angle between sacral end plate and horizontal.
- Positional parameter; correlates with lumbar lordosis.
Fundamental relation
[
\mathbf{PI = PT + SS}
]
This equation is central to spinopelvic harmony.
Harmony with Lumbar Lordosis
- PI influences required lumbar lordosis (LL).
- Clinical target in adult deformity planning: PI-LL mismatch < 10° (or LL approximately matched to PI).
- If LL is inadequate for PI, patient compensates via pelvic retroversion (↑PT), hip extension, knee flexion.
Additional Illustration (spondylolisthesis and spinopelvic angles)
Orthopedic Applications
1) Spondylolysis / Spondylolisthesis
- High PI and high SS are associated with greater shear force at lumbosacral junction and predisposition to slip progression.
- Slip angle and spinopelvic parameters guide prognosis and surgery.
- Used in deciding need for fusion and extent of correction.
2) Adult Spinal Deformity (kyphosis, flat-back, sagittal imbalance)
- Preoperative planning is based on PI, PT, SS, LL, sagittal vertical axis.
- Goal: restore harmonious alignment to reduce pain, fatigue, and implant failure.
- Inadequate restoration leads to persistent disability and adjacent segment issues.
3) Total Hip Arthroplasty (THA)
- Spinopelvic motion affects functional acetabular orientation.
- Patients with stiff spine/spinopelvic junction (e.g., sacral slope change <10° from sit to stand) have higher dislocation risk.
- Important in cup positioning, selecting implants (e.g., dual mobility in high-risk cases), and evaluating recurrent instability.
4) Hip-Spine Syndrome
- Back deformity can alter pelvic posture and hip biomechanics.
- Helps determine whether primary pathology is hip-driven or spine-driven and sequence of surgeries.
5) Pediatric/Adolescent deformity follow-up
- Useful in monitoring sagittal compensation and progression risk patterns.
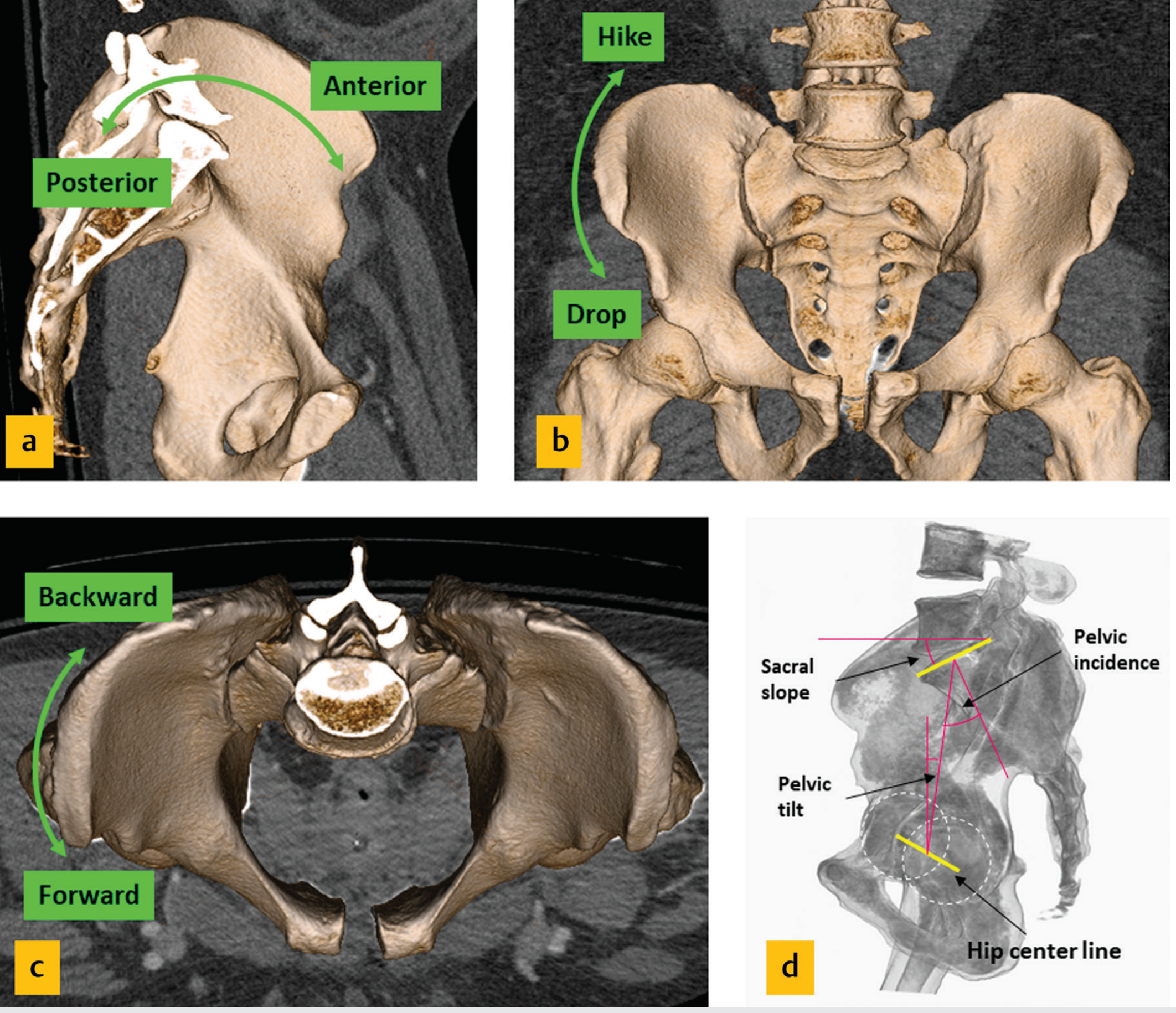
Pelvic motion and compensation concept
Conclusion
Spinopelvic harmony is a key biomechanical concept linking pelvic morphology and spinal alignment.
Understanding PI, PT, SS and their relation to LL is essential in modern orthopedics for:
Understanding PI, PT, SS and their relation to LL is essential in modern orthopedics for:
- spinal deformity correction,
- spondylolisthesis management,
- THA planning and instability prevention,
- comprehensive hip-spine assessment.
High-yield take-home line:
PI is fixed; PT and SS are positional; and maintaining PI-LL harmony is the cornerstone of sagittal balance.
PI is fixed; PT and SS are positional; and maintaining PI-LL harmony is the cornerstone of sagittal balance.
Sources: Miller’s Review of Orthopaedics, 9th ed, relevant figures and text sections on pelvic incidence, spondylolisthesis, and spinopelvic alignment in THA; Imaging Anatomy Text and Atlas Vol. 3, function of pelvis sections.
Spinopelvic harmony with its application in Orthopedics with appropriate illustrative diagrams for 10 marks
Spinopelvic Harmony with Applications in Orthopedics (10 marks)
Definition
Spinopelvic harmony is the optimal sagittal alignment between the spine and pelvis that allows energy-efficient standing, balanced posture, and horizontal gaze.
Key spinopelvic parameters
-
Pelvic Incidence (PI)
- Angle between:
- a line perpendicular to the sacral endplate midpoint, and
- a line joining this midpoint to femoral head center.
- Morphologic/anatomic parameter (largely fixed in adults).
- Average around 50°.
- Angle between:
-
Pelvic Tilt (PT)
- Angle between line from sacral midpoint to femoral head center and vertical.
- Positional parameter (increases with pelvic retroversion).
-
Sacral Slope (SS)
- Angle between sacral endplate and horizontal.
- Positional parameter; influences lumbar lordosis.
Fundamental equation
[
\boxed{PI = PT + SS}
]
Relation to lumbar lordosis
- PI determines required lumbar lordosis (LL).
- Harmony exists when LL is matched to PI (commonly PI-LL mismatch ideally <10° in deformity correction).
- Loss of harmony causes compensations: increased PT, hip extension, knee flexion, fatigue, and pain.
Illustrative diagram: spondylolisthesis and spinopelvic angles
Applications in Orthopedics
1) Spondylolysis and spondylolisthesis
- High PI/high SS may increase shear at L5-S1 and predispose slip progression.
- PT, SS, PI and slip angle help in risk stratification and surgical planning.
- Guides decision on fusion level and degree of correction.
2) Adult spinal deformity
- Central in pre-op planning for kyphosis/flat-back/sagittal imbalance.
- Correction goals include restoration of PI-LL harmony and reducing compensatory pelvic retroversion.
- Better harmony correlates with better function and outcomes.
3) Total Hip Arthroplasty (THA)
- Spinopelvic mobility affects functional acetabular orientation.
- Stiff spinopelvic junction (small SS change from sitting to standing) increases dislocation risk.
- Helps in cup positioning and implant strategy (e.g., dual-mobility options in selected patients).
4) Hip-spine syndrome
- Helps differentiate spine-driven vs hip-driven symptoms.
- Important for sequencing spine and hip procedures.
5) Pediatric/adolescent deformity monitoring
- Useful in progression assessment and long-term sagittal alignment planning.
Additional conceptual pelvic motion diagram
Conclusion
Spinopelvic harmony is a core biomechanical principle in orthopedic practice. Understanding PI, PT, SS, and their relation to lumbar lordosis is essential for management of spinal deformity, spondylolisthesis, and THA stability.
High-yield line: PI is fixed, PT and SS are positional, and restoration of PI-LL harmony is key to good outcomes.
High-yield line: PI is fixed, PT and SS are positional, and restoration of PI-LL harmony is key to good outcomes.
This is a shared conversation. Sign in to Orris to start your own chat.