Jvp, hepato jugular reflex
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of JVP and the hepatojugular reflex.
Jugular Venous Pressure (JVP)
What It Measures
The JVP is the single most important bedside measurement for estimating volume status and right atrial (central venous) pressure. The internal jugular vein is preferred — the external jugular is valved and not directly in line with the SVC and right atrium.
How to Measure
- Patient positioned at 45° (or sitting upright if elevated pressure is suspected)
- JVP is quantified as the vertical distance from the top of the jugular venous pulsation to the sternal angle (angle of Louis)
- >4.5 cm above the sternal angle at 30° elevation is abnormal
- Note: the sternal angle systematically underestimates CVP; the clavicle is an easier reference point — venous pulsations above the clavicle in the sitting position are clearly abnormal (distance from clavicle to right atrium is ≥10 cm)
- Bedside CVP is measured in cmH₂O; convert to mmHg: 1.36 cmH₂O = 1.0 mmHg
JVP vs. Carotid Pulse — Key Differences
| Feature | JVP | Carotid |
|---|---|---|
| Waveform | Biphasic (in sinus rhythm) | Monophasic |
| Obliterated by palpation | Yes | No |
| Changes with posture/inspiration | Yes | No |
The JVP Waveform
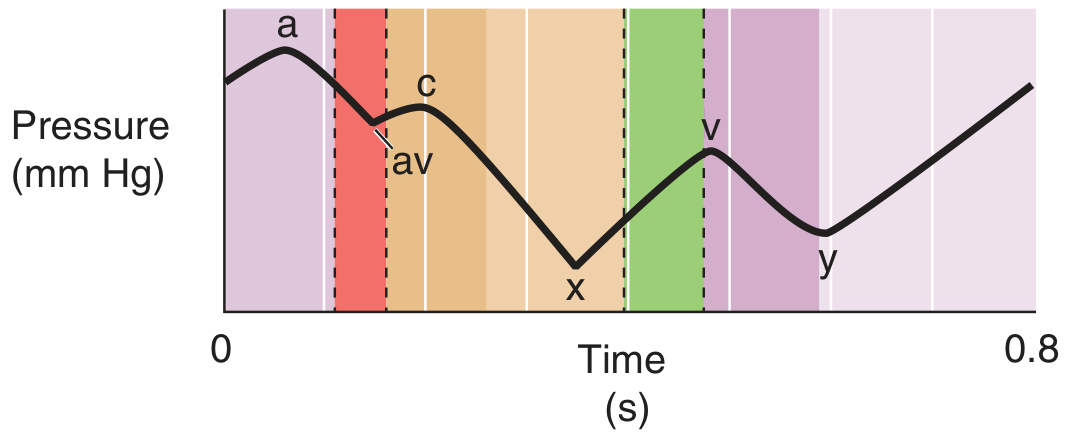
JVP waveform — Medical Physiology
Peaks (Positive Deflections)
| Wave | Cause |
|---|---|
| a | Right atrial presystolic contraction (just after P wave, before S1) |
| c | Pressure rise in right ventricle early in systole + bulging of closed tricuspid valve into right atrium |
| v | Filling of right atrium against closed tricuspid valve during ventricular systole |
Descents (Negative Deflections)
| Descent | Cause |
|---|---|
| av (x') | Relaxation of right atrium + closure of tricuspid valve |
| x | Ventricular contraction and shortening during ejection phase — pulls on veins, lowering pressure |
| y | Opening of tricuspid valve → blood drains from right atrium |
Clinical Variants of the JVP Waveform
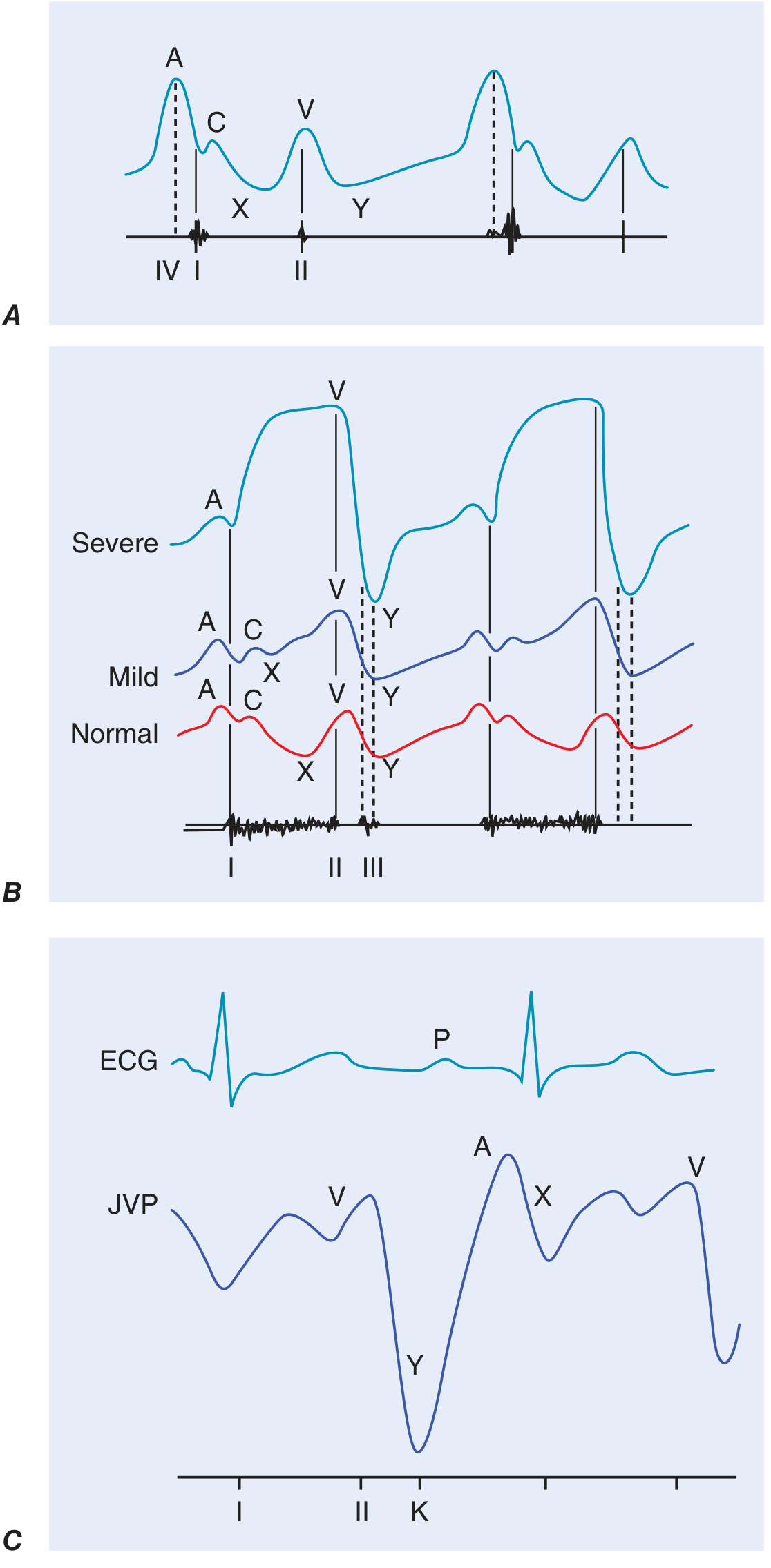
Panel A: prominent A wave with reduced RV compliance. Panel B: progressive "ventricularization" of waveform in tricuspid regurgitation (mild → severe). Panel C: prominent rapid Y descent with pericardial knock (K) in constrictive pericarditis. — Harrison's Principles of Internal Medicine 22E
| Condition | Waveform Change |
|---|---|
| Reduced RV compliance (RVH, pulmonary HTN, PS) | Prominent a wave |
| AV dissociation | Cannon a waves (RA contracts against closed tricuspid) |
| Atrial fibrillation | No a wave |
| Tricuspid regurgitation | Large cv wave — waveform becomes "ventricularized" |
| Constrictive pericarditis | Prominent, rapid y descent + pericardial knock |
| Cardiac tamponade | Prominent x descent, absent y descent |
| Kussmaul's sign | Paradoxical rise in JVP with inspiration (constrictive pericarditis, severe RV failure) |
Hepatojugular Reflux (Abdominojugular Reflux)
How to Perform
- Apply firm, consistent pressure over the right upper quadrant of the abdomen
- Maintain pressure for >15 seconds
- Assess the jugular venous pulsations throughout
- Assess the response after 10 seconds of continuous pressure (to allow respiratory artifacts and abdominal muscle tensing to subside)
- Instruct the patient NOT to hold their breath or Valsalva — this is a critical instruction to ensure a valid test
Positive Result
- A sustained rise of >3 cm in JVP during abdominal compression = positive test
Physiology
The maneuver displaces blood from the abdominal venous reservoir into the right heart. A volume-overloaded state with limited compliance of an overly distended or constricted venous system prevents the right ventricle from accommodating this extra volume, so pressure backs up and JVP rises.
Clinical Significance
- Predicts a pulmonary artery wedge pressure >15 mmHg in patients with heart failure
- A positive result indicates the right atrial pressure is >10 mmHg, which has an 88% positive predictive value for a pulmonary artery wedge pressure >22 mmHg in advanced heart failure
- Useful in diagnosing right heart failure and volume overload
Diagnostic Performance (JVP vs. Other Signs in Heart Failure)
| Sign | Sensitivity | Specificity | LR+ |
|---|---|---|---|
| JVP >12 mmHg | 65% | 64% | 1.79 |
| Hepatojugular reflux | 83% | 27% | 1.13 |
| Ascites (moderate/massive) | 21% | 92% | 2.44 |
| Rales (>1/3 lung fields) | 15% | 89% | 1.32 |
| Edema (>2+) | 41% | 66% | 1.20 |
— Braunwald's Heart Disease & Harrison's Principles of Internal Medicine 22E
Clinical Pearl
An elevated JVP carries prognostic significance in both symptomatic heart failure and asymptomatic LV systolic dysfunction — it is associated with higher risk of subsequent hospitalization for heart failure and death from heart failure.
This is a shared conversation. Sign in to Orris to start your own chat.