I have all the key source material needed. Let me now compile the comprehensive lower limb osteology guide.
Complete Osteology of the Lower Limb - MS1 Guide
Sources: Gray's Anatomy for Students; Morgan & Mikhail's Clinical Anesthesiology 7e; Campbell's Operative Orthopaedics 15e
1. HIP BONE (Os Coxae)
The hip bone is formed by the fusion of three bones - ilium, ischium, and pubis - which meet at the acetabulum (at approximately 16 years of age). The two hip bones plus the sacrum and coccyx form the pelvis.
Ilium
The largest of the three parts; forms the superior portion.
| Feature | Details |
|---|
| Iliac crest | Superior curved border; palpable from ASIS to PSIS; ends anteriorly at the ASIS and posteriorly at the PSIS; highest point at the level of L4 (used for lumbar puncture landmark) |
| ASIS (Anterior Superior Iliac Spine) | Anterior end of the iliac crest; origin of sartorius and attachment of inguinal ligament |
| AIIS (Anterior Inferior Iliac Spine) | Below the ASIS; origin of the straight head of rectus femoris |
| PSIS (Posterior Superior Iliac Spine) | Posterior end of iliac crest; overlies the S2 sacral foramen; dimple of Venus in skin |
| PIIS (Posterior Inferior Iliac Spine) | Below the PSIS, above the greater sciatic notch |
| Iliac fossa | Concave medial surface; origin of iliacus muscle |
| Auricular surface | Posterior medial surface; articulates with the sacrum (sacroiliac joint) |
| Gluteal surface (posterior/lateral) | Three gluteal lines (anterior, posterior, inferior) marking origins of gluteal muscles |
| Iliopectineal (arcuate) line | Marks the pelvic brim (inlet) on the medial surface |
| Iliac tubercle | Thickening on the outer lip of the iliac crest, ~5 cm posterior to the ASIS |
Ischium
Forms the posteroinferior part.
| Feature | Details |
|---|
| Ischial tuberosity | Large roughening on the posteroinferior surface; bears the body weight when sitting; origin of hamstrings (biceps femoris long head, semitendinosus, semimembranosus) and adductor magnus (hamstring part) |
| Ischial spine | Projects medially from the posterior border; attachment of sacrospinous ligament; divides the greater sciatic notch (above) from the lesser sciatic notch (below) |
| Greater sciatic notch | Superior to the ischial spine; converted to the greater sciatic foramen by the sacrospinous ligament |
| Lesser sciatic notch | Between the ischial spine and ischial tuberosity; converted to the lesser sciatic foramen |
| Ischial ramus | Projects forward and medially to join the inferior pubic ramus |
Pubis
Forms the anteroinferior part.
| Feature | Details |
|---|
| Body | Medial portion; articulates with the opposite pubic body at the pubic symphysis |
| Pubic crest | Superior border of the body |
| Pubic tubercle | Rounded eminence at the lateral end of the pubic crest; attachment of the inguinal ligament; landmark for the femoral canal |
| Superior pubic ramus | Extends laterally from the body to the acetabulum; bears the pecten pubis (pectineal line) |
| Inferior pubic ramus | Extends downward and laterally to join the ischial ramus |
| Obturator foramen | Large opening formed by the pubis and ischium; mostly closed by the obturator membrane; transmits the obturator nerve and vessels through the obturator canal (superolateral gap) |
Acetabulum
Formed by all three bones (ilium = 2/5, ischium = 2/5, pubis = 1/5). Features:
- Lunate surface - horseshoe-shaped articular area for the femoral head
- Acetabular fossa - central non-articular depression; contains fat pad and ligamentum teres
- Acetabular notch - inferior gap in the lunate surface; bridged by the transverse acetabular ligament
2. FEMUR
The longest and strongest bone in the body. The angle between the neck and shaft (angle of inclination) is approximately 126° in adults; reduced in coxa vara, increased in coxa valga. There is also a forward twist of the neck relative to the shaft (angle of anteversion, ~10-15°).
Proximal End
| Feature | Details |
|---|
| Head | Two-thirds of a sphere; articular surface; small fovea capitis (pit) for the ligamentum teres |
| Neck | Connects the head to the shaft at 126°; the superior surface is under compression, the inferior surface under tension in normal walking |
| Greater trochanter | Large lateral projection at the junction of neck and shaft; can be palpated; attachment for gluteus medius (lateral surface), gluteus minimus (anterior surface), obturator internus and gemelli (medial surface via trochanteric fossa), piriformis (apex) |
| Lesser trochanter | Posteromedial projection below the neck; insertion of iliopsoas |
| Trochanteric fossa | Depression on the medial surface of the greater trochanter; attachment of obturator internus and gemelli |
| Intertrochanteric line | Anterior; runs between the two trochanters; attachment of the iliofemoral ligament (strongest ligament in the body) |
| Intertrochanteric crest | Posterior; bears the quadrate tubercle (insertion of quadratus femoris) |
Shaft
| Feature | Details |
|---|
| Linea aspera | Prominent posterior longitudinal ridge; has medial and lateral lips; attachment for adductors (medial lip), vastus medialis (medial lip), vastus lateralis (lateral lip), short head of biceps femoris (lateral lip), and gluteus maximus via the iliotibial tract |
| Pectineal line | Runs from the lesser trochanter to the linea aspera; attachment for pectineus |
| Gluteal tuberosity | Upper lateral lip of linea aspera; attachment for gluteus maximus |
| Nutrient foramen | On the posterior surface; directed proximally (blood supply from below) |
Distal End
| Feature | Details |
|---|
| Medial and lateral condyles | Large articular prominences; articulate with the tibia |
| Intercondylar fossa (notch) | Posterior gap between the condyles; contains the cruciate ligaments |
| Medial epicondyle | Medial projection above the medial condyle; attachment for the tibial collateral ligament and medial head of gastrocnemius |
| Lateral epicondyle | Lateral projection; attachment for the fibular collateral ligament and lateral head of gastrocnemius |
| Adductor tubercle | Small prominence just above the medial epicondyle; insertion of adductor magnus (adductor/anterior part) |
| Patellar surface | Anterior; smooth groove between the condyles; articulates with the patella |
| Linea aspera diverges | Distally, the linea aspera splits into the medial supracondylar ridge and lateral supracondylar ridge, enclosing the popliteal surface |
Clinical Notes
- Neck of femur fractures: most common in elderly osteoporotic women; the leg shortens and externally rotates
- Mid-shaft fractures: risk to the profunda femoris artery and significant blood loss (1-2 L)
- Supracondylar fractures: risk to the popliteal artery (posterior relationship)
3. PATELLA
The largest sesamoid bone in the body; lies within the quadriceps tendon.
- Apex: inferior; attachment of the patellar ligament
- Base: superior; attachment of rectus femoris
- Anterior surface: roughened; separated from skin by the prepatellar bursa
- Posterior (articular) surface: divided by a vertical ridge into a larger lateral facet and smaller medial facet
4. TIBIA
The weight-bearing bone of the leg; medial and larger.
Proximal End
| Feature | Details |
|---|
| Medial condyle | Large medial articular surface for the medial femoral condyle |
| Lateral condyle | Lateral articular surface; fibula head articulates on its posteroinferior aspect |
| Intercondylar area | Between the articular surfaces; anterior and posterior intercondylar areas for attachment of menisci and cruciate ligaments |
| Intercondylar eminence | Raised bony ridges between the articular surfaces; medial and lateral tubercles |
| Tibial tuberosity | Anterior prominence on the proximal shaft; insertion of the patellar ligament (quadriceps mechanism); site of Osgood-Schlatter disease |
| Gerdy's tubercle | Anterolateral surface of the lateral condyle; insertion of the iliotibial tract |
| Soleal line | Oblique line on the posterior surface of the proximal shaft; attachment for soleus |
Shaft
- Anterior border (shin) - subcutaneous and palpable throughout
- Medial surface - subcutaneous; overlies the medial compartment
- Interosseous border - lateral sharp border; attachment of interosseous membrane
Distal End
| Feature | Details |
|---|
| Medial malleolus | Medial projection; articulates with the medial surface of the talus |
| Inferior articular surface | Articulates with the superior surface of the talus (ankle/talocrural joint) |
| Fibular notch | Lateral; articulates with the fibula at the distal tibiofibular syndesmosis |
5. FIBULA
Slender lateral bone; non-weight-bearing; provides muscle attachment and forms the lateral part of the ankle mortise.
Proximal End
- Head - articulates with the lateral condyle of the tibia (proximal tibiofibular joint; synovial plane joint)
- Neck - just distal to the head; where the common fibular nerve winds around; most common site of fibular fracture
Shaft
- Interosseous border - medial sharp ridge; attachment of interosseous membrane
- Multiple compartments of muscles attach to the fibular shaft
Distal End
- Lateral malleolus - projects more distally than the medial malleolus; articulates with the lateral surface of the talus
- Key attachment point for the lateral collateral ligaments (anterior and posterior talofibular, calcaneofibular)
6. TARSAL BONES (7 bones)
| Bone | Key Features |
|---|
| Talus | No muscle attachments; articulates superiorly with tibia (talocrural joint), inferiorly with calcaneus (subtalar joint), anteriorly with navicular; has head, neck, and body |
| Calcaneus | Largest tarsal; forms the heel; bears the sustentaculum tali (medial shelf supporting the talus; flexor hallucis longus runs beneath it); calcaneal tuberosity posteriorly (attachment of Achilles tendon = calcaneal tendon); most commonly fractured tarsal (axial loading); peroneal trochlea (lateral) separates peroneus longus from brevis |
| Navicular | Medial side; articulates with the talus posteriorly and three cuneiforms anteriorly; navicular tuberosity (medial side, insertion of tibialis posterior) |
| Medial cuneiform | Articulates with navicular posteriorly and 1st metatarsal anteriorly |
| Intermediate cuneiform | Smallest of the three; articulates with navicular and 2nd metatarsal |
| Lateral cuneiform | Articulates with navicular, cuboid, and 3rd metatarsal |
| Cuboid | Lateral side; articulates with calcaneus posteriorly and 4th/5th metatarsals anteriorly; has a groove for peroneus longus tendon on its plantar surface |
Tarsal Tunnel
The tarsal tunnel lies posterior and inferior to the medial malleolus, between the medial malleolus and calcaneus, roofed by the flexor retinaculum (laciniate ligament). Contents (medial to lateral - "Tom Dick And Very Nervous Harry"):
- Tibialis posterior
- Digitorum flexor (FDL)
- Artery (posterior tibial)
- Vein (posterior tibial)
- Nerve (tibial nerve)
- Hallucis longus flexor (FHL)
Compression here causes tarsal tunnel syndrome (medial plantar heel and arch pain).
7. METATARSALS AND PHALANGES
Metatarsals
Five bones; each has a base (proximal), shaft, and head (distal).
- 1st metatarsal: shortest and most robust; articulates with the medial cuneiform; two sesamoid bones (medial and lateral) lie under its head
- 5th metatarsal: has a prominent styloid process (tuberosity) at the base on the lateral side; insertion of peroneus brevis; commonly avulsed in inversion injuries ("pseudo-Jones fracture")
- Jones fracture = true stress fracture at the diaphyseal-metaphyseal junction of the 5th metatarsal (zone 2)
- 2nd metatarsal base is recessed between the cuneiforms ("keystone"); most rigid; stress fractures common here in marching (march fracture)
Phalanges
- Great toe (hallux) has 2 phalanges (proximal and distal)
- Toes 2-5 have 3 phalanges each (proximal, middle, distal)
- Each phalanx has a base, shaft, and head
8. SPECIAL REGIONS AND SPACES
Femoral Triangle
A wedge-shaped depression in the upper anterior thigh.
| Boundary | Structure |
|---|
| Base (superior) | Inguinal ligament |
| Lateral border | Medial border of sartorius |
| Medial border | Medial border of adductor longus |
| Floor | Iliopsoas (laterally) + pectineus + adductor longus (medially) |
| Roof | Fascia lata + cribriform fascia (over saphenous opening) |
Contents (lateral to medial - mnemonic: "NAVEL"):
- Nerve (femoral) - lateral to the sheath, NOT in the femoral sheath
- Artery (femoral)
- Vein (femoral)
- Empty space (femoral canal - lymphatics)
- Lymphatics / lacunar ligament (medial wall)
The femoral sheath (funnel of fascia) surrounds the artery, vein, and the femoral canal (lymphatics) - but NOT the femoral nerve. The most medial compartment (femoral canal) is the site of femoral hernias.
The femoral artery can be palpated just inferior to the inguinal ligament at the midpoint between the ASIS and pubic symphysis (the mid-inguinal point).
Adductor Canal (Subsartorial / Hunter's Canal)
- Continuation of the femoral triangle inferiorly
- Bounded anterolaterally by the vastus medialis, posteriorly by adductor longus and adductor magnus, and covered by sartorius
- Contents: femoral artery, femoral vein, saphenous nerve (branch of femoral nerve), nerve to vastus medialis
- The femoral artery passes through the adductor hiatus at the distal end of adductor magnus to enter the popliteal fossa as the popliteal artery
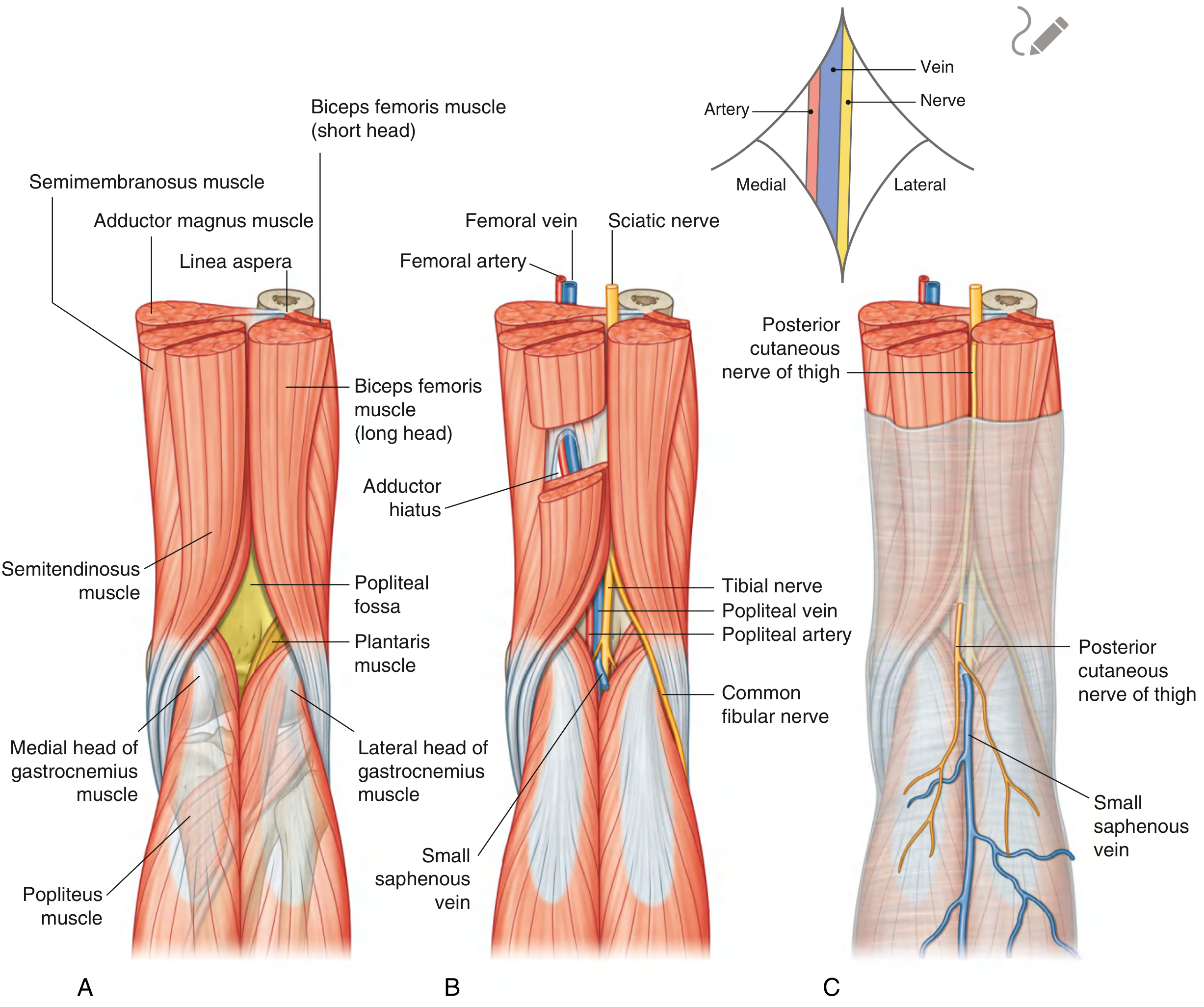
Popliteal Fossa
A diamond-shaped space posterior to the knee joint; the major transition zone between the thigh and the leg.
| Boundary | Structure |
|---|
| Upper medial | Semitendinosus + semimembranosus |
| Upper lateral | Biceps femoris |
| Lower medial | Medial head of gastrocnemius |
| Lower lateral | Lateral head of gastrocnemius + plantaris |
| Floor (deep) | Popliteal surface of femur, capsule of knee joint, popliteus muscle |
| Roof | Deep fascia (popliteal fascia); small saphenous vein + posterior cutaneous nerve of thigh are in the roof |
Contents (superficial to deep):
- Tibial nerve - most superficial; descends vertically through the fossa
- Common fibular nerve - follows biceps femoris to the fibular neck
- Popliteal vein - between nerve and artery
- Popliteal artery - deepest; lies on the floor; continuation of femoral artery through the adductor hiatus
The popliteal artery divides at the lower border of popliteus into the anterior tibial artery (passes through a gap in the interosseous membrane) and posterior tibial artery.
Clinical: The popliteal artery is vulnerable in distal femur fractures (supracondylar). Popliteal artery aneurysm may present as a pulsatile mass; associated with aneurysms elsewhere.
Gluteal Region - Key Structures
The gluteal region communicates with the thigh and leg via the greater sciatic foramen. The piriformis divides the greater sciatic foramen into:
- Above piriformis: superior gluteal nerve and vessels
- Below piriformis: inferior gluteal nerve, sciatic nerve, posterior cutaneous nerve of thigh, pudendal nerve, nerve to obturator internus, nerve to quadratus femoris
Sciatic nerve (L4-S3) is the largest nerve in the body; exits below piriformis and descends posterior to the thigh. It divides into tibial and common fibular nerves, usually in the popliteal fossa (sometimes higher).
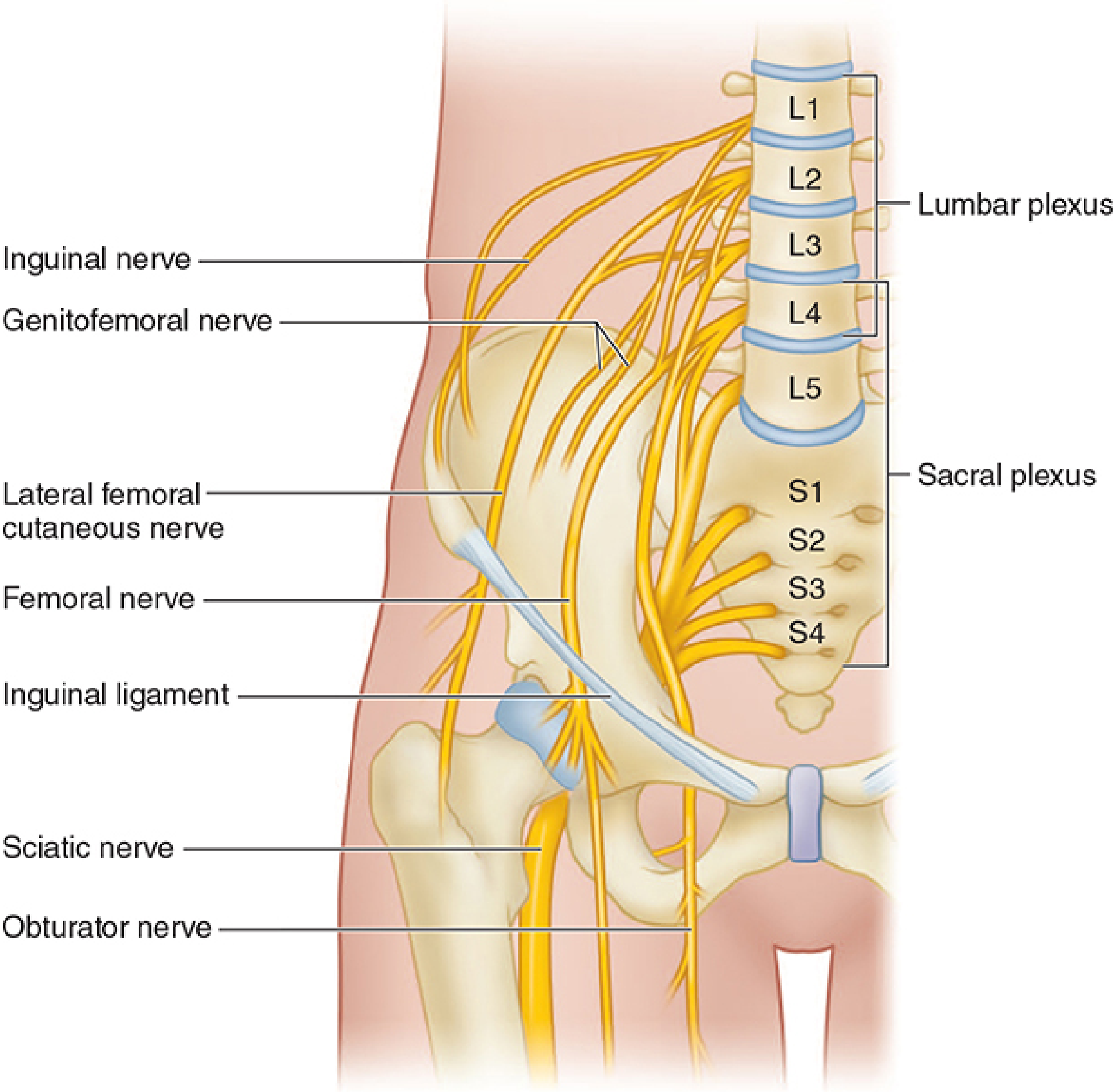
9. NERVE PLEXUSES OF THE LOWER LIMB
Lumbar Plexus (L1-L4, with contribution from T12)
Formed within the psoas major muscle.
| Nerve | Root | Motor | Sensory |
|---|
| Iliohypogastric | L1 | Internal oblique, transversus abdominis | Skin of the lateral hip and inguinal region |
| Ilioinguinal | L1 | Internal oblique | Skin of medial thigh + scrotum/labia majora |
| Genitofemoral | L1-L2 | Cremaster (genital branch) | Anterior scrotum/labia + small patch of anterior thigh (femoral branch) |
| Lateral femoral cutaneous | L2-L3 | None (pure sensory) | Lateral thigh; meralgia paresthetica when compressed under inguinal ligament near ASIS |
| Femoral nerve | L2-L4 | Iliopsoas, quadriceps, sartorius, pectineus | Anterior thigh + medial leg/foot (saphenous nerve) |
| Obturator nerve | L2-L4 | Adductors (longus, brevis, magnus-adductor part), gracilis, obturator externus | Medial thigh |
Sacral Plexus (L4-S4)
Formed on the posterior pelvic wall (anterior to piriformis).
| Nerve | Root | Motor | Sensory |
|---|
| Superior gluteal | L4-S1 | Gluteus medius, minimus, tensor fasciae latae | None |
| Inferior gluteal | L5-S2 | Gluteus maximus | None |
| Sciatic (tibial + common fibular) | L4-S3 | Hamstrings, all leg and foot muscles | Posterior thigh (via posterior femoral cutaneous), leg, and foot |
| Posterior femoral cutaneous | S1-S3 | None | Posterior thigh, upper leg |
| Pudendal | S2-S4 | Perineal muscles, external sphincters | Perineum, genitalia |
10. MUSCLE SUMMARY BY COMPARTMENT
Gluteal Region
| Muscle | Origin | Insertion | Action | Nerve |
|---|
| Gluteus maximus | Posterior ilium, sacrum, coccyx, sacrotuberous lig. | Gluteal tuberosity + iliotibial tract | Extension + lateral rotation of hip | Inferior gluteal (L5-S2) |
| Gluteus medius | Between anterior and posterior gluteal lines | Greater trochanter (lateral surface) | Abduction; anterior fibers medially rotate | Superior gluteal (L4-S1) |
| Gluteus minimus | Between anterior and inferior gluteal lines | Greater trochanter (anterior surface) | Abduction + medial rotation | Superior gluteal |
| Piriformis | Anterior sacrum | Greater trochanter (apex) | Lateral rotation | Nerve to piriformis (S1-S2) |
| Obturator internus | Internal surface of obturator membrane + surrounding bone | Greater trochanter (medial surface via trochanteric fossa) | Lateral rotation | Nerve to obturator internus (L5-S1) |
| Gemellus superior | Ischial spine | Trochanteric fossa | Lateral rotation | Nerve to obturator internus |
| Gemellus inferior | Ischial tuberosity | Trochanteric fossa | Lateral rotation | Nerve to quadratus femoris (L4-S1) |
| Quadratus femoris | Ischial tuberosity (lateral border) | Quadrate tubercle of intertrochanteric crest | Lateral rotation | Nerve to quadratus femoris |
| Tensor fasciae latae (TFL) | ASIS + iliac crest | Iliotibial (IT) tract | Abduction + medial rotation; stabilizes extended knee via IT tract | Superior gluteal |
Thigh - Anterior Compartment
| Muscle | Origin | Insertion | Action | Nerve |
|---|
| Iliopsoas (iliacus + psoas major) | Iliac fossa (iliacus); T12-L5 vertebral bodies/transverse processes (psoas) | Lesser trochanter | Flexion of hip; psoas also flexes lumbar spine | Femoral (iliacus) + direct branches L1-L3 (psoas) |
| Sartorius | ASIS | Medial surface of proximal tibia (pes anserinus) | Hip flexion, abduction, lateral rotation; knee flexion + medial rotation | Femoral |
| Rectus femoris | AIIS (straight head); acetabular rim (reflected head) | Patella + patellar ligament to tibial tuberosity | Knee extension + hip flexion | Femoral |
| Vastus lateralis | Greater trochanter + lateral lip of linea aspera | Patella (lateral retinaculum + patellar ligament) | Knee extension | Femoral |
| Vastus medialis | Medial lip of linea aspera | Patella (medial retinaculum + patellar ligament) | Knee extension; distal fibers (VMO) prevent patellar lateralization | Femoral |
| Vastus intermedius | Anterior shaft of femur | Patella | Knee extension | Femoral |
Thigh - Medial Compartment (Adductors)
| Muscle | Origin | Insertion | Action | Nerve |
|---|
| Pectineus | Pecten pubis | Pectineal line of femur | Adduction + flexion | Femoral (+ obturator) |
| Adductor longus | Pubic body (front) | Middle third of linea aspera (medial lip) | Adduction | Obturator |
| Adductor brevis | Inferior pubic ramus | Upper third of linea aspera | Adduction | Obturator |
| Adductor magnus | Inferior pubic ramus + ischial ramus (adductor part) + ischial tuberosity (hamstring part) | Linea aspera + adductor tubercle | Adduction; hamstring part extends hip | Obturator (adductor part) + tibial (hamstring part) |
| Gracilis | Inferior pubic ramus | Medial surface proximal tibia (pes anserinus) | Adduction + knee flexion + medial rotation of knee | Obturator |
| Obturator externus | External surface of obturator membrane | Trochanteric fossa | Lateral rotation | Obturator |
Thigh - Posterior Compartment (Hamstrings)
All arise from the ischial tuberosity (except short head of biceps femoris) and are innervated by the tibial division of the sciatic nerve (except short head of biceps = common fibular division).
| Muscle | Origin | Insertion | Action |
|---|
| Biceps femoris (long head) | Ischial tuberosity | Head of fibula | Hip extension + knee flexion + lateral rotation of knee |
| Biceps femoris (short head) | Lateral lip of linea aspera | Head of fibula | Knee flexion + lateral rotation of knee |
| Semitendinosus | Ischial tuberosity | Medial surface proximal tibia (pes anserinus) | Hip extension + knee flexion + medial rotation of knee |
| Semimembranosus | Ischial tuberosity | Medial condyle of tibia (posterior) | Hip extension + knee flexion + medial rotation of knee |
Pes anserinus ("goose foot") = common insertion of sartorius, gracilis, and semitendinosus on the medial proximal tibia; contains the pes anserine bursa.
Leg - Anterior Compartment
Innervated by the deep fibular (peroneal) nerve; anterior tibial artery.
| Muscle | Origin | Insertion | Action |
|---|
| Tibialis anterior | Lateral condyle + upper 2/3 of tibia | Medial cuneiform + base of 1st metatarsal | Dorsiflexion + inversion |
| Extensor hallucis longus | Middle fibula + interosseous membrane | Base of distal phalanx of great toe | Extension of great toe + dorsiflexion |
| Extensor digitorum longus | Lateral condyle of tibia + fibula | Dorsal aponeurosis of toes 2-5 | Toe extension + dorsiflexion |
| Fibularis (peroneus) tertius | Lower fibula | Base of 5th metatarsal | Dorsiflexion + eversion |
Leg - Lateral Compartment
Innervated by the superficial fibular (peroneal) nerve.
| Muscle | Origin | Insertion | Action |
|---|
| Fibularis (peroneus) longus | Upper 2/3 of fibula | Medial cuneiform + base of 1st metatarsal (crosses sole diagonally) | Eversion + plantarflexion; supports the lateral arch |
| Fibularis (peroneus) brevis | Lower 2/3 of fibula | Tuberosity of 5th metatarsal (styloid process) | Eversion + plantarflexion |
Leg - Posterior Compartment
Superficial group (innervated by tibial nerve):
| Muscle | Origin | Insertion | Action |
|---|
| Gastrocnemius (medial head) | Medial epicondyle of femur | Calcaneus via calcaneal (Achilles) tendon | Plantarflexion + knee flexion |
| Gastrocnemius (lateral head) | Lateral epicondyle of femur | Calcaneus via Achilles tendon | Plantarflexion + knee flexion |
| Soleus | Posterior head of fibula + soleal line of tibia | Calcaneus via Achilles tendon | Plantarflexion (main); "peripheral heart" pumping venous blood |
| Plantaris | Lateral supracondylar ridge | Calcaneus | Weak plantarflexion; used for tendon grafts |
Deep group (innervated by tibial nerve):
| Muscle | Origin | Insertion | Action |
|---|
| Popliteus | Lateral condyle of femur | Posterior proximal tibia | "Unlocks" the knee (medially rotates tibia when going from extension to flexion) |
| Flexor digitorum longus (FDL) | Posterior tibia | Bases of distal phalanges of toes 2-5 | Toe flexion + plantarflexion |
| Flexor hallucis longus (FHL) | Posterior fibula | Base of distal phalanx of great toe | Great toe flexion + plantarflexion; passes beneath sustentaculum tali |
| Tibialis posterior | Posterior tibia + fibula + interosseous membrane | Navicular tuberosity + all other tarsals except talus | Inversion + plantarflexion; maintains medial longitudinal arch |
11. CLINICAL CORRELATES - HIGH-YIELD FOR MS1
| Injury/Site | Nerve at Risk | Deficit |
|---|
| Posterior hip dislocation | Sciatic nerve | Foot drop + hamstring weakness + sensory loss posterior leg/foot |
| Fibular neck fracture | Common fibular nerve | Foot drop (loss of dorsiflexion + eversion); sensory loss dorsum of foot + lateral leg |
| Knee dislocation | Popliteal artery (and tibial nerve) | Limb ischemia; posterior tibial pulse loss |
| Medial knee injury (valgus stress) | Saphenous nerve (femoral) | Medial knee/leg pain; associated with MCL + medial meniscus damage ("unhappy triad") |
| ASIS avulsion | ASIS apophysis | Pain + weakness of hip flexion/abduction |
| Hip fracture (femoral neck) | Medial circumflex femoral artery (blood supply to femoral head) | Avascular necrosis of femoral head |
| Inversion sprain (ankle) | Anterior talofibular ligament most common | Lateral ankle instability; 5th metatarsal avulsion by peroneus brevis |
| Lumbar disc herniation L4-L5 | L5 root | Weakness of dorsiflexion + great toe extension; sensory loss dorsum of foot |
| Lumbar disc herniation L5-S1 | S1 root | Weakness of plantarflexion + eversion; diminished ankle reflex; sensory loss lateral foot |
| Meralgia paresthetica | Lateral femoral cutaneous nerve (L2-L3) | Numbness/burning lateral thigh; compressed under inguinal ligament at ASIS; no motor deficit |
| Compartment syndrome (leg) | Anterior compartment most common | Pain with passive toe extension; tight anterior compartment; risk to deep fibular nerve and anterior tibial artery |
Gray's Anatomy for Students, Blocks 3 & 4; Morgan & Mikhail's Clinical Anesthesiology 7e (Lumbar & Sacral Plexus); Campbell's Operative Orthopaedics 15e