Short comparison between permanent access,temporary,and emergency in dialysis patients, also illustrates preference of choice, indication and complications and their management. Creat in poster form
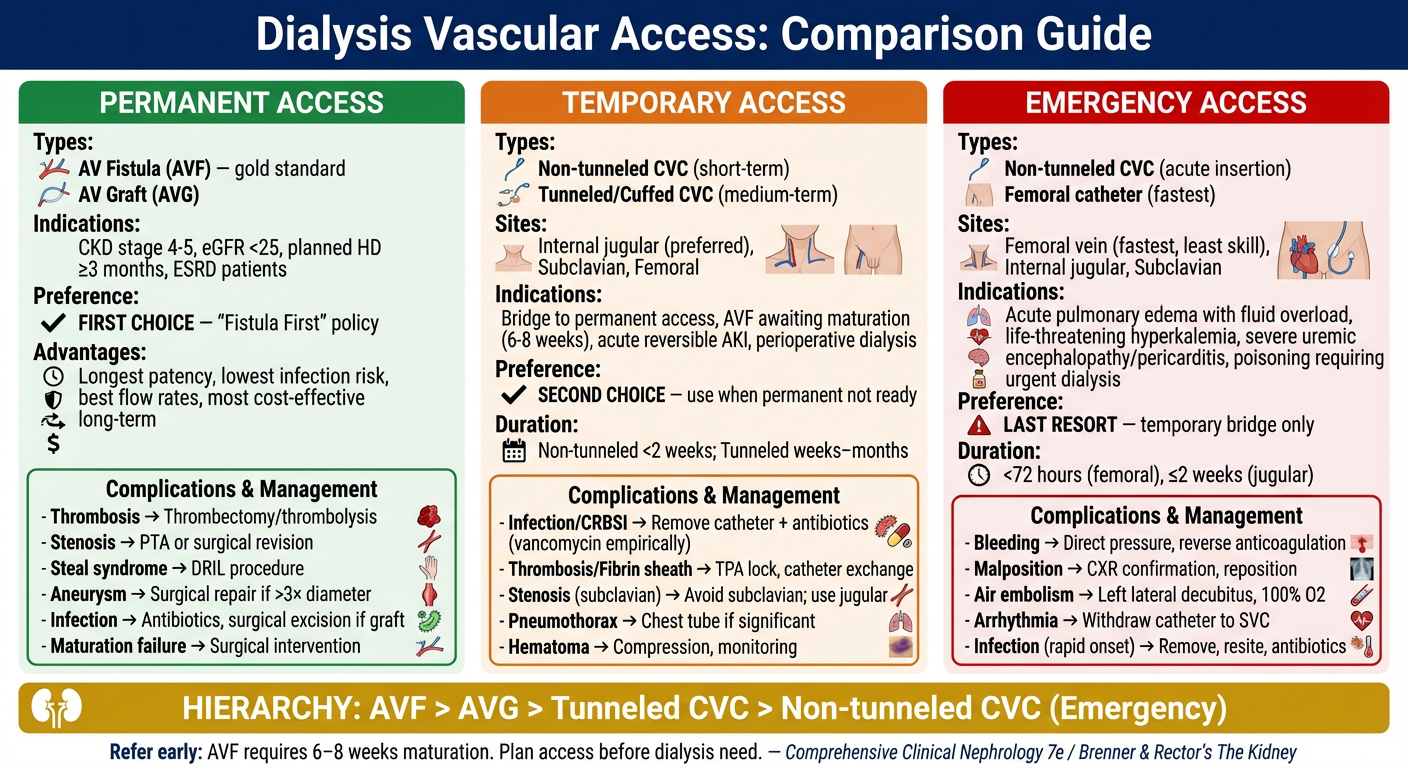
Medical educational poster titled "Dialysis Vascular Access: Comparison Guide" with three main columns for Permanent Access, Temporary Access, and Emergency Access. Layout: dark navy blue header with white title text. Three color-coded columns below (green for Permanent, orange for Temporary, red for Emergency). PERMANENT ACCESS column (green header): Types: AV Fistula (AVF) — gold standard, AV Graft (AVG) Indications: CKD stage 4-5, eGFR <25, planned HD ≥3 months, ESRD patients Preference: FIRST CHOICE — "Fistula First" policy Advantages: Longest patency, lowest infection risk, best flow rates, most cost-effective long-term Complications & Management box: - Thrombosis → Thrombectomy/thrombolysis - Stenosis → PTA or surgical revision - Steal syndrome → DRIL procedure - Aneurysm → Surgical repair if >3× diameter - Infection → Antibiotics, surgical excision if graft - Maturation failure → Surgical intervention TEMPORARY ACCESS column (orange header): Types: Non-tunneled CVC (short-term), Tunneled/Cuffed CVC (medium-term) Sites: Internal jugular (preferred), Subclavian, Femoral Indications: Bridge to permanent access, AVF awaiting maturation (6-8 weeks), acute reversible AKI, perioperative dialysis Preference: SECOND CHOICE — use when permanent not ready Duration: Non-tunneled <2 weeks; Tunneled weeks–months Complications & Management box: - Infection/CRBSI → Remove catheter + antibiotics (vancomycin empirically) - Thrombosis/Fibrin sheath → TPA lock, catheter exchange - Stenosis (subclavian) → Avoid subclavian; use jugular - Pneumothorax → Chest tube if significant - Hematoma → Compression, monitoring EMERGENCY ACCESS column (red header): Types: Non-tunneled CVC (acute insertion), Femoral catheter (fastest) Sites: Femoral vein (fastest, least skill), Internal jugular, Subclavian Indications: Acute pulmonary edema with fluid overload, life-threatening hyperkalemia, severe uremic encephalopathy/pericarditis, poisoning requiring urgent dialysis Preference: LAST RESORT — temporary bridge only Duration: <72 hours (femoral), ≤2 weeks (jugular) Complications & Management box: - Bleeding → Direct pressure, reverse anticoagulation - Malposition → CXR confirmation, reposition - Air embolism → Left lateral decubitus, 100% O2 - Arrhythmia → Withdraw catheter to SVC - Infection (rapid onset) → Remove, resite, antibiotics Bottom row: HIERARCHY banner in gold: "AVF > AVG > Tunneled CVC > Non-tunneled CVC (Emergency)" with kidney icon Footer note: "Refer early: AVF requires 6–8 weeks maturation. Plan access before dialysis need." — Comprehensive Clinical Nephrology 7e / Brenner & Rector's The Kidney Clean infographic style, professional medical poster, clear readable fonts, icons for each complication type, white background for columns with colored headers, well-spaced layout.
Dialysis Vascular Access — Quick Reference
Access Hierarchy (Preference Order)
🟢 Permanent Access — FIRST CHOICE
| Feature | AV Fistula (AVF) | AV Graft (AVG) |
|---|---|---|
| Preferred site | Radiocephalic > Brachiocephalic | Brachioaxillary (PTFE) |
| Indication | CKD stage 4–5, eGFR <25, planned HD | Failed AVF attempts, inadequate veins |
| Maturation | 6–8 weeks | 2–3 weeks |
| Patency | Best (years) | Moderate |
🟠 Temporary Access — SECOND CHOICE
- Types: Non-tunneled CVC (<2 weeks) | Tunneled/Cuffed CVC (weeks–months)
- Preferred site: Internal jugular (avoid subclavian — stenosis risk)
- Indication: Bridge to AVF maturation, reversible AKI, perioperative HD
🔴 Emergency Access — LAST RESORT
- Types: Non-tunneled CVC, femoral vein catheter (fastest insertion)
- Duration: Femoral <72 h | Jugular ≤2 weeks
- Indications: Acute life-threatening hyperkalemia, severe uremic complications (encephalopathy, pericarditis), refractory pulmonary edema, intoxication
Key principle: Refer early. An AVF must be created months before dialysis is needed. The "Fistula First, Catheter Last" initiative exists because catheters carry significantly higher mortality, infection, and hospitalization rates compared to native fistulas. — Comprehensive Clinical Nephrology 7e; Brenner & Rector's The Kidney
Summary State
Dialysis Vascular Access — Summary
Core Concept
Three Access Types at a Glance
| Permanent | Temporary | Emergency | |
|---|---|---|---|
| Types | AVF, AVG | Tunneled / Non-tunneled CVC | Non-tunneled CVC, Femoral catheter |
| Preference | 1st choice | 2nd choice | Last resort |
| Duration | Years | Weeks–months | Hours–days |
| Infection risk | Lowest | Moderate | Highest |
| Best site | Forearm/arm vessels | Internal jugular | Femoral / jugular |
Indications Summary
- Permanent → Planned chronic HD, CKD stage 4–5 (eGFR <25), referred early
- Temporary → Bridging while AVF matures, reversible AKI, perioperative HD
- Emergency → Life-threatening hyperkalemia, uremic emergency, refractory pulmonary edema
Top Complications & Management
| Complication | Access Type | Management |
|---|---|---|
| Thrombosis | AVF/AVG | PTA or thrombectomy |
| Steal syndrome | AVF/AVG | DRIL procedure |
| CRBSI | CVC (all) | Remove catheter + vancomycin |
| Fibrin sheath | Tunneled CVC | tPA lock or catheter exchange |
| Subclavian stenosis | Non-tunneled CVC | Avoid subclavian; use jugular |
| Air embolism | Emergency CVC | Left lateral decubitus + 100% O₂ |
Golden Rules
- Fistula First, Catheter Last — AVF has the best survival outcomes
- Plan ahead — AVF needs 6–8 weeks to mature before use
- Avoid subclavian for temporary access — risks future central vein stenosis
- Femoral catheters must be removed within 72 hours due to high infection and thrombosis risk
- Every catheter day = increased mortality risk; transition to permanent access as soon as possible