Ctev
Reading File
Finding Sources
Finding Sources
Searching PubMed
"clubfoot" AND "Ponseti" AND treatment
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have all the information needed for a comprehensive answer.
CTEV - Congenital Talipes Equinovarus (Clubfoot)
Definition
CTEV is a congenital deformity of the foot characterized by a combination of four components, remembered by the mnemonic CAVE:
| Component | Description |
|---|---|
| C - Cavus | High arch (plantar flexion of forefoot on hindfoot) |
| A - Adductus | Adduction of the forefoot |
| V - Varus | Varus of the hindfoot |
| E - Equinus | Plantar flexion at the ankle |
Epidemiology
- Boys affected twice as often as girls
- 50% of cases are bilateral
- Incidence: ~1-2 per 1,000 live births
Etiology
- Majority idiopathic - genetic cause strongly suggested
- Key genetic pathway: PITX1-TBX4 transcriptional pathway
- Associated conditions:
- Arthrogryposis
- Myelomeningocele
- Diastrophic dwarfism
- Prune-belly syndrome
- Tibial hemimelia
- Streeter dysplasia (hand anomalies)
- Other neuromuscular/syndromic conditions
Pathoanatomy
- Talar neck deformity - medial and plantar deviation of the talar neck
- Medial rotation of calcaneus
- Medial displacement of navicular and cuboid
- Shortening/contracture of:
- Intrinsic foot muscles
- Achilles tendon
- Tibialis posterior
- Flexor hallucis longus (FHL)
- Flexor digitorum longus (FDL)
- Joint capsules, ligaments, and fascia
- Associated with absence or diminutive anterior tibial artery
Radiographic Findings
Radiographs are of limited use in infants due to minimal ossification. When used:
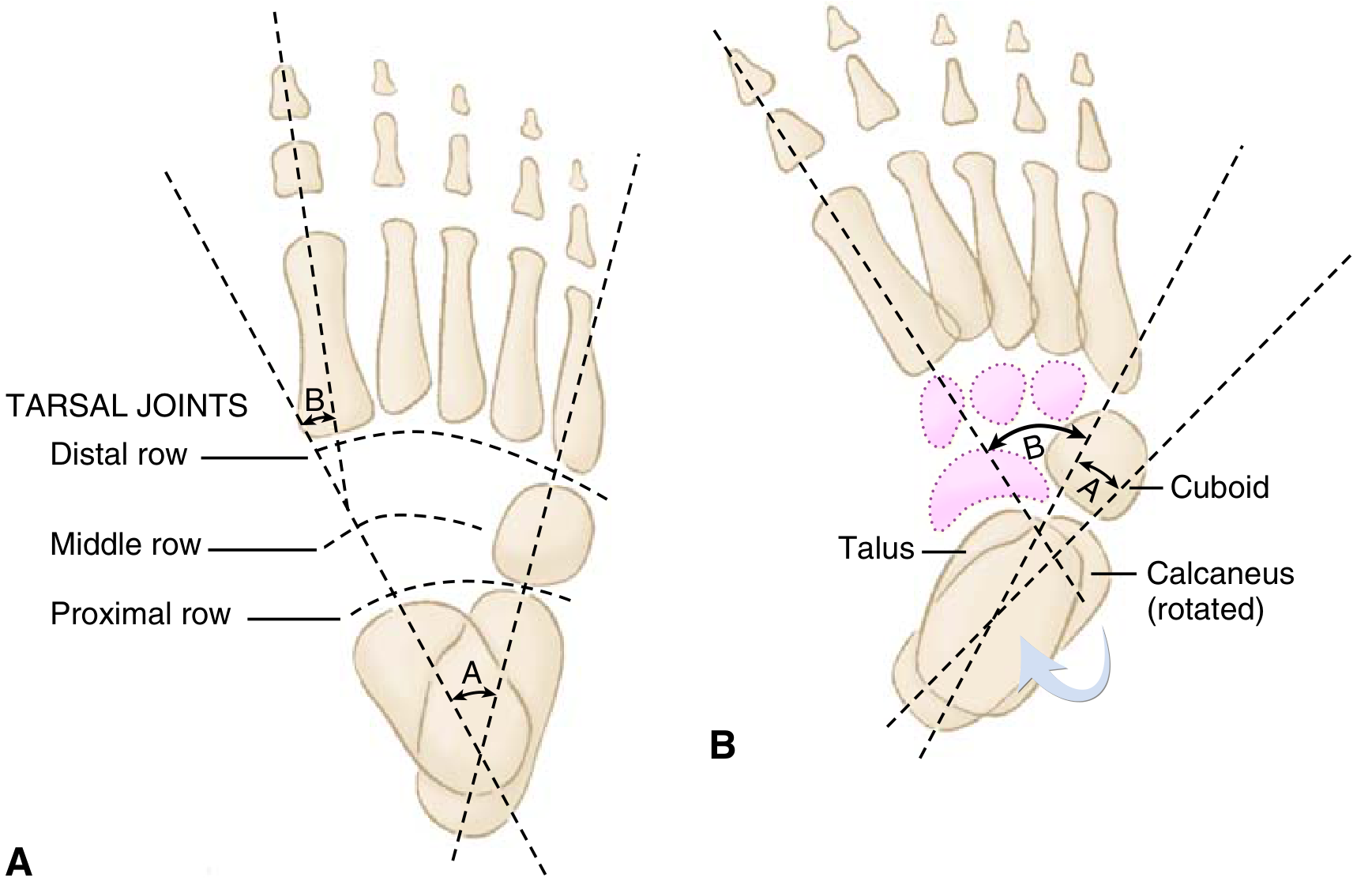
Fig. 3.20 - (A) Normal foot. (B) Clubfoot showing "parallelism" of talus and calcaneus.
| Measurement | Normal | Clubfoot |
|---|---|---|
| Talocalcaneal angle (AP/Kite angle) | 20-40° | < 20° (parallelism) |
| Talocalcaneal angle (lateral/Turco - dorsiflexion view) | ~35° | < 35° |
| Talus-1st metatarsal angle (AP) | 0-20° | Negative |
The key X-ray finding is parallelism of the talus and calcaneus (normally they diverge).
Treatment
1. Ponseti Method (Gold Standard - First Line)
Serial weekly manipulation and casting using long-leg plaster casts.
Order of correction follows CAVE (same mnemonic, but correction sequence):
- Cavus - corrected first by supinating the forefoot and dorsiflexing the first ray
- Adductus - corrected using lateral pressure on distal talar head as a fulcrum
- Varus - corrected simultaneously with adductus
- Equinus - addressed last (after varus is fully corrected to avoid rocker-bottom deformity)
Key steps:
- ~90% of patients require percutaneous Achilles tendon lengthening (tenotomy) to address hindfoot equinus
- Last cast placed in 70° of abduction
- Treatment typically complete in 1-5 months
2. Foot Abduction Brace (FAB) - Mandatory Post-Casting
- Full-time wear for 3 months post-casting
- Then during naps and nighttime for 3 years
- Brace non-compliance is the #1 cause of recurrence
- No impairment in athletic ability after successful treatment
Complications of Treatment
| Complication | Cause |
|---|---|
| Recurrence / undercorrection | Most common; strongly associated with brace non-compliance |
| Rocker-bottom deformity | Attempting to dorsiflex hindfoot before varus is corrected |
| Flat-top talus | Aggressive dorsiflexion causing flattening of the talar dome |
| Dorsal bunion | After clubfoot surgery; tibialis anterior + FHB/abductor hallucis |
Operative Treatment
Reserved for only ~5% of idiopathic clubfeet (resistant/refractory cases):
-
Posteromedial soft tissue release (PMSTR): tendon lengthening + subtalar, tibiotalar, and talonavicular release
- Must protect posterior tibial artery (dorsalis pedis often insufficient)
- Used in severe disease or when treatment initiated after 9 months of age
-
Older children (3-10 years): medial opening-wedge or lateral column-shortening osteotomy, or cuboidal decancellation for persistent adductus
-
Late presentation: Triple arthrodesis
- Contraindicated in insensate feet (risk of ulceration from rigidity)
Recent Evidence (2024-2026)
Recent systematic reviews confirm the Ponseti method as the standard of care:
- A 2024 systematic review (PMID 39365806) found Ponseti method is also effective for myelodysplastic (non-idiopathic) clubfoot.
- A 2026 meta-analysis (PMID 40888800) compared Plaster of Paris vs. semirigid fiberglass casting - POP remains the reference standard.
- A 2024 systematic review (PMID 39134994) examined anterior tibial tendon transfer fixation techniques for dynamic supination relapse.
Sources: Miller's Review of Orthopaedics, 9th Ed., p. 282; Schwartz's Principles of Surgery, 11th Ed., p. 1946
This is a shared conversation. Sign in to Orris to start your own chat.