High bp complications
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Here is a well-organized clinical overview:
Complications of High Blood Pressure (Hypertension)
Hypertension (HTN) causes damage through two broad mechanisms:
- Chronic target organ damage (TOD) — from sustained elevated pressure over years
- Acute hypertensive emergencies — from abrupt, severe BP rises (≥180/110 mmHg) that overwhelm autoregulatory mechanisms
1. Cardiovascular Complications
Coronary Artery Disease & Acute Coronary Syndrome
HTN accelerates atherosclerosis. It is the primary population-attributable risk factor for chronic cardiac dysfunction. Over 50% of ED patients with acute heart failure have elevated BP at presentation.
Left Ventricular Hypertrophy (LVH)
Sustained pressure overload causes concentric hypertrophy, detectable on ECG or chest X-ray. LVH precedes more serious end-organ damage.
Heart Failure
Both with reduced (HFrEF) and preserved (HFpEF) ejection fraction. Patients with acute heart failure and HTN respond well to vasodilatory agents and afterload reduction.
- Acute heart failure: 14–37% of hypertensive emergencies
- Acute coronary syndrome: 11–12% of hypertensive emergencies
Aortic Dissection
An acute HTN-driven emergency. Antihypertensive therapy is a key component of management.
- Incidence: 1–2% of hypertensive emergencies
2. Cerebrovascular Complications
Ischemic Stroke
HTN is the single most important modifiable risk factor for stroke.
- Acute ischemic stroke: 6–25% of hypertensive emergencies
Intracranial Hemorrhage (ICH)
The BP elevation in ICH may be compensatory, but long-standing HTN is often causal.
- Spontaneous ICH: 5–23% of hypertensive emergencies
Hypertensive Encephalopathy
The classic hypertensive emergency. Caused by failure of cerebral autoregulation → vasogenic cerebral edema → diffuse ischemia and punctate hemorrhages.
Features:
- Severe headache, vomiting, altered consciousness
- May progress to seizures or coma
- Papilledema and hypertensive retinopathy
- Focal neurological deficits that don't follow a single anatomic pattern
- Incidence: 8–16% of hypertensive emergencies
Fully reversible with early BP reduction (30–40% decrease). In-hospital mortality <1%.
Posterior Reversible Encephalopathy Syndrome (PRES)
HTN is the most common associated condition. Presents with visual changes, headache, altered mental status, and seizures. Diagnosed by white matter edema in posterior parietal-temporal-occipital regions on MRI. Reversible with treatment.
3. Renal Complications
Hypertensive Nephrosclerosis / Glomerulosclerosis
Chronic pressure damage to glomerular arterioles leads to:
- Reduced GFR (progressive CKD)
- Arteriolo- and glomerulosclerosis
- Tubular atrophy
Acute Kidney Injury (AKI)
In hypertensive emergencies:
- Acute renal risk: 15% of cases
- Acute kidney injury: 8% of cases
AKI may be a consequence of associated cardiac failure or direct renal vascular injury.
4. Ophthalmologic Complications
Hypertensive Retinopathy
- The earliest sign on physical examination in most hypertensive individuals
- Findings: focal intraretinal periarterio-lar transudates, retinal hemorrhages, papilledema
- Strongly associated with enhanced stroke risk
- Severe cases → blurred vision progressing to complete blindness
5. Peripheral Vascular Disease
Chronic HTN accelerates atherosclerosis in the peripheral arteries, leading to claudication and limb ischemia.
6. Complications in Special Populations
Pregnancy (Preeclampsia/Eclampsia)
- Chronic HTN → risk of superimposed preeclampsia, placental abruption, fetal growth restriction, preterm birth
- Eclampsia accounts for ~2% of hypertensive emergencies
Summary Table: Hypertensive Emergency — Target Organ Incidence
| Organ System | Complication | Approximate Incidence |
|---|---|---|
| Heart (cumulative) | — | 27–49% |
| Acute heart failure | 14–37% | |
| Acute coronary syndrome | 11–12% | |
| Brain (cumulative) | — | 37–45% |
| Acute ischemic stroke | 6–25% | |
| Spontaneous ICH | 5–23% | |
| Hypertensive encephalopathy | 8–16% | |
| Kidney | Acute renal risk | 15% |
| Acute kidney injury | 8% | |
| Vascular | Aortic dissection | 1–2% |
| Other | Eclampsia | 2% |
| Acute hypertensive retinopathy | 1% |
— Rosen's Emergency Medicine, 10e
Key Pathophysiology (Acute Emergencies)
An abrupt BP rise overwhelms autoregulation → endothelial injury → ↓ nitric oxide, ↑ endothelin → further ↑ SVR → terminal arteriole dilation and rupture → fibrinoid necrosis → diffuse ischemia, microangiopathic hemolytic anemia, and tissue edema across multiple organ beds.
Sources: Rosen's Emergency Medicine; Goldman-Cecil Medicine, 2e; Fuster & Hurst's The Heart, 15e; Swanson's Family Medicine Review
Asthma management according to gina guidelines
Asthma management according to gina guidelines in paediatric patients
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full response:
Asthma Management in Paediatric Patients — GINA Guidelines
1. Diagnosis & Initial Assessment
Diagnosis in children, especially under 5 years, is challenging as no reliable objective tests exist in this age group — it relies entirely on clinical presentation. Key features include:
- Recurrent wheeze, cough, breathlessness, chest tightness
- Symptoms worse at night or with exercise/viral infections
- Response to bronchodilator therapy
Asthma Predictive Index (API) — used in children <3 years:
- 3+ episodes of wheezing in the first 3 years PLUS
- ≥1 major risk factor: parental history of asthma OR physician-diagnosed atopic dermatitis; OR
- ≥2 minor risk factors: wheezing apart from colds, peripheral eosinophilia >4%, food sensitisation
2. Classifying Asthma Severity in Children
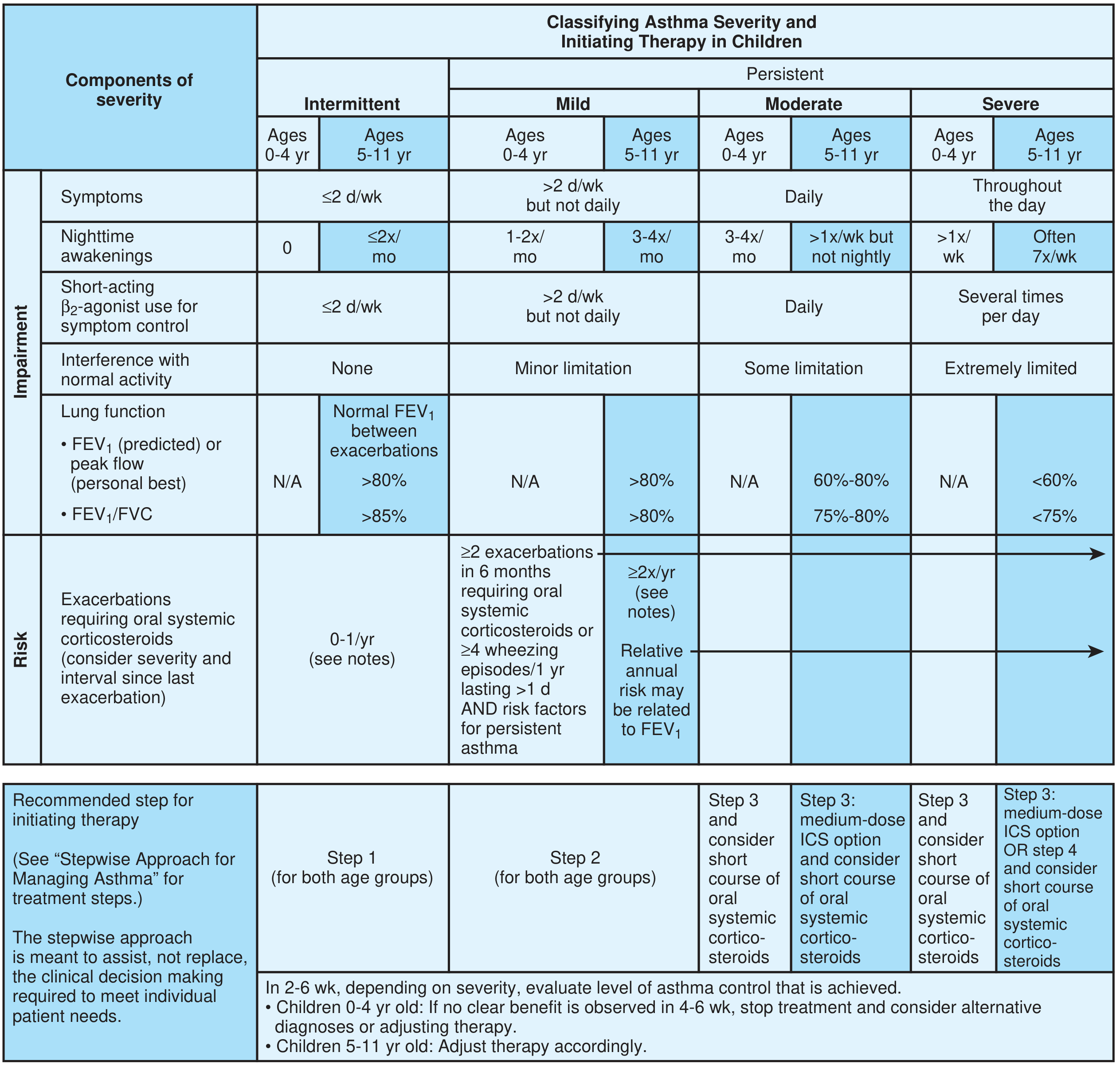
— Textbook of Family Medicine 9e (based on NAEPP EPR-3 / GINA framework)
| Severity | Symptoms | Nighttime Awakenings | SABA Use | Lung Function |
|---|---|---|---|---|
| Intermittent | ≤2 d/wk | 0 (0–4 yr) / ≤2×/mo (5–11 yr) | ≤2 d/wk | Normal FEV₁ between attacks |
| Mild Persistent | >2 d/wk but not daily | 1–2×/mo (0–4 yr) / 3–4×/mo (5–11 yr) | >2 d/wk | FEV₁ >80% |
| Moderate Persistent | Daily | 3–4×/mo (0–4 yr) / >1×/wk (5–11 yr) | Daily | FEV₁ 60–80% |
| Severe Persistent | Throughout the day | >1×/wk (0–4 yr) / Often nightly (5–11 yr) | Several times/day | FEV₁ <60% |
GINA defines severity by the amount of treatment required to control asthma (retrospectively, after several months on therapy):
- Mild: controlled at Step 1–2
- Moderate: controlled at Step 3
- Severe: requires Step 4–5 or remains uncontrolled despite it
3. Assessing Asthma Control (GINA)
Control is assessed over the past 4 weeks:
| Question | Yes | No |
|---|---|---|
| Daytime symptoms >2×/wk? | ||
| Any night waking due to asthma? | ||
| Reliever needed for symptoms >2×/wk? | ||
| Any activity limitation due to asthma? |
- 0 "Yes" → Well controlled
- 1–2 "Yes" → Partly controlled
- 3–4 "Yes" → Uncontrolled
Risk Factors for Poor Outcomes
- Uncontrolled symptoms
- Frequent SABA use, poor inhaler technique, non-adherence
- Obesity, chronic rhinosinusitis, GERD
- Smoking exposure, allergen exposure, air pollution
- Low FEV₁ (<60% predicted)
- Prior severe exacerbation
- Psychosocial or socioeconomic factors
4. GINA Stepwise Management (Adults/Adolescents >11 yr — for context)
| Step | Preferred Controller | Other Controller Options | Preferred Reliever |
|---|---|---|---|
| Step 1 | As-needed low-dose ICS-formoterol | Low-dose ICS taken whenever SABA used | As-needed low-dose ICS-formoterol |
| Step 2 | Low-dose ICS, or as-needed ICS-formoterol | LTRA, or low-dose ICS whenever SABA used | As-needed low-dose ICS-formoterol |
| Step 3 | Low-dose ICS-LABA | Medium-dose ICS, or low-dose ICS+LTRA | As-needed low-dose ICS-formoterol |
| Step 4 | Medium-dose ICS-LABA | High-dose ICS, add-on tiotropium, or LTRA | As-needed low-dose ICS-formoterol |
| Step 5 | High-dose ICS-LABA + refer for phenotyping ± biologics | Add low-dose oral corticosteroids (with caution) | As-needed low-dose ICS-formoterol |
— Murray & Nadel's Textbook of Respiratory Medicine
Key GINA shift: ICS-formoterol (not SABA alone) is now the preferred reliever at all steps, including Step 1 (intermittent asthma), because even mild asthma carries exacerbation risk.
5. Stepwise Approach Specific to Children
Children 0–4 Years
- Step 1: Intermittent SABA (as needed); no daily controller required
- Step 2: Daily low-dose ICS (preferred); LTRA as alternative
- Step 3: Medium-dose ICS; consider short course of oral corticosteroids for exacerbations
- Step 4: Medium-dose ICS + LABA (or montelukast); specialist referral recommended
If no clear benefit in 4–6 weeks at any step in 0–4 year olds → stop treatment and reconsider the diagnosis
Children 5–11 Years
- Step 1: SABA as needed (≤2 episodes/wk)
- Step 2: Low-dose ICS (preferred); LTRA or cromones as alternatives
- Step 3: Medium-dose ICS or low-dose ICS + LABA; refer if not controlled
- Step 4: Medium-dose ICS + LABA ± LAMA; specialist referral
- Step 5: High-dose ICS + LABA; consider add-on biologics (e.g., omalizumab ≥6 yrs, mepolizumab ≥6 yrs EU)
Initiating Therapy Based on Severity
| Severity at Diagnosis | Recommended Starting Step |
|---|---|
| Intermittent | Step 1 |
| Mild Persistent | Step 2 |
| Moderate Persistent | Step 3 (both age groups); consider short-course OCS |
| Severe Persistent | Step 3–4 + consider short-course OCS |
Evaluate level of control in 2–6 weeks; adjust therapy accordingly.
6. Step-Up / Step-Down Principles
| Control Level | Action |
|---|---|
| Well controlled (≥3 months) | Step down — reduce to lowest effective step |
| Not well controlled | Step up one step; follow up in 2–6 weeks |
| Very poorly controlled | Step up 1–2 steps; consider short course oral corticosteroids; follow up in 2 weeks |
Before stepping up, always check: adherence, inhaler technique, trigger avoidance, and comorbidities.
7. Inhaler Device Considerations in Children
- MDI + spacer is as effective as or better than a nebulizer in children with acute asthma exacerbations (Level of Evidence: A)
- Younger children (<4 yrs) require a spacer with facemask
- Children 4–6 years can transition to spacer with mouthpiece
- Dry powder inhalers (DPI) generally suitable for children ≥6 years who can generate sufficient inspiratory flow
8. Management of Exacerbations in Children
Exacerbations feature progressive worsening of breathlessness, wheeze, cough, or chest tightness.
| Severity | FEV₁/PEF | Management |
|---|---|---|
| Moderate | 40–69% predicted | Inhaled SABA q20min × 3, systemic corticosteroids, O₂ if needed |
| Severe | <40% predicted | Continuous SABA nebulisation, IV/IM corticosteroids, O₂, consider IV magnesium |
| Impending respiratory arrest | <25% or unable to measure | ICU, possible intubation |
9. Non-Pharmacological Management
- Trigger identification and avoidance: house dust mite, animal dander, tobacco smoke, exercise, viral URTIs, cold air
- Written asthma action plan for every child and caregiver
- Allergen immunotherapy (SCIT/SLIT): considered in children with allergic asthma where allergens cannot be avoided
- Regular follow-up: every 1–6 months (well-controlled) or 2–6 weeks (after step changes)
- Patient/caregiver education: inhaler technique, recognising worsening, when to seek emergency care
Key Sources: Murray & Nadel's Textbook of Respiratory Medicine; Textbook of Family Medicine 9e; The Washington Manual of Medical Therapeutics; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.