causes of heart attack
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of the causes of a heart attack (myocardial infarction), drawn from authoritative medical textbooks.
Causes of a Heart Attack (Myocardial Infarction)
A myocardial infarction (MI) is necrosis of heart muscle resulting from ischemia — an inadequate blood and oxygen supply to the myocardium.
The Dominant Cause: Atherosclerotic Coronary Artery Disease
The vast majority (~90%) of MIs are caused by acute thrombosis within a coronary artery. The sequence is:
- Atherosclerosis — lipid-rich plaques accumulate in the coronary artery wall over years, progressively narrowing the lumen.
- Plaque disruption — a vulnerable plaque ruptures or erodes (triggered by inflammation, mechanical stress, hypertension, or vasoconstriction).
- Thrombus formation — platelet aggregation and clotting at the rupture site creates an occlusive thrombus, completely blocking blood flow.
- Myocardial necrosis — the territory supplied by that artery is starved of oxygen and dies.
The diagram below illustrates this progression:
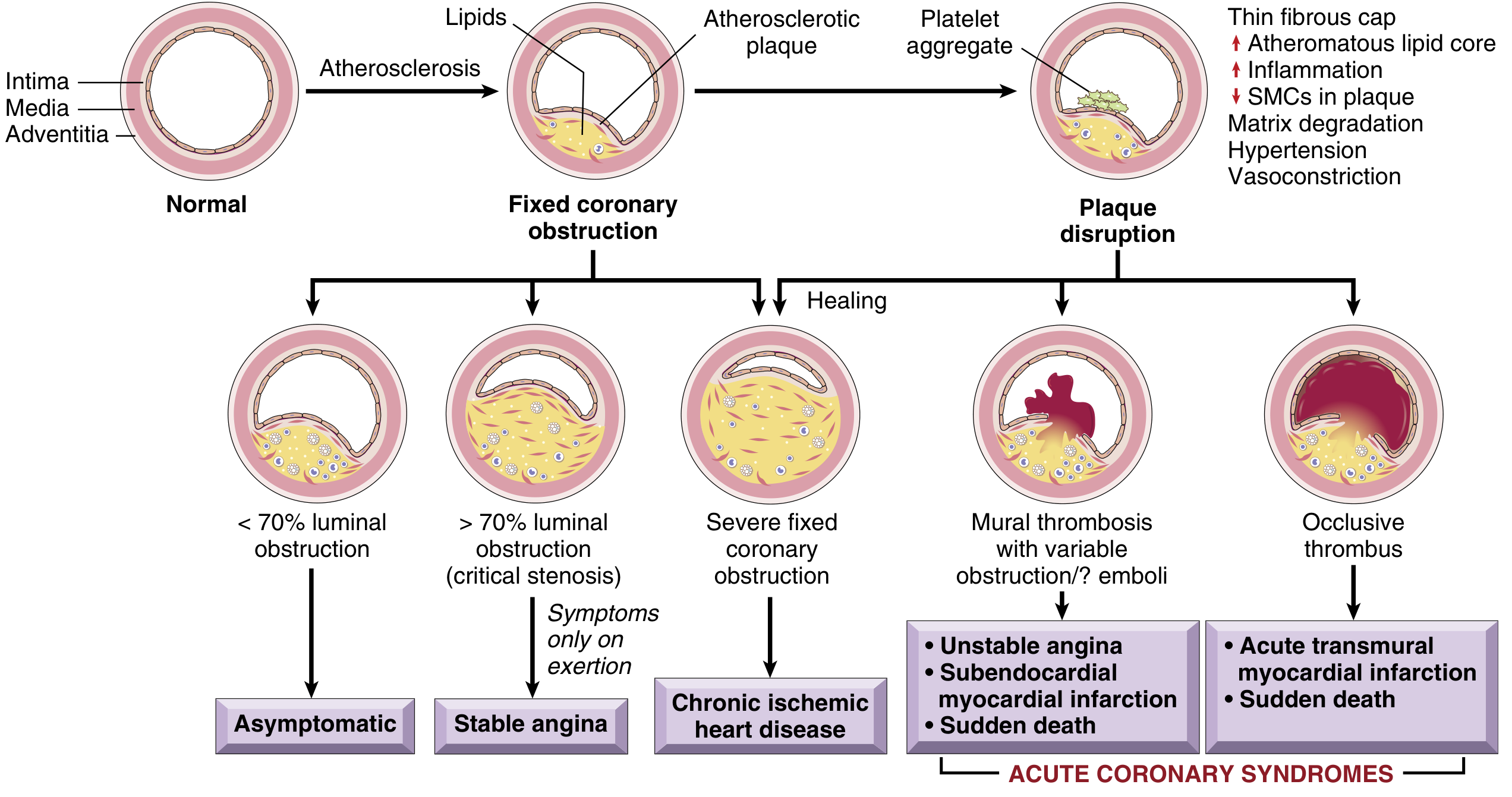
— Robbins & Kumar Basic Pathology
Risk Factors That Drive Atherosclerosis
These accelerate plaque buildup:
- Dyslipidemia (high LDL, low HDL)
- Hypertension
- Diabetes mellitus
- Cigarette smoking
- Obesity and physical inactivity
- Family history / genetics
- Age (risk rises progressively; men affected earlier than women)
- Male sex (women are relatively protected until menopause, after which risk equalizes)
Non-Atherosclerotic Causes (~10% of MIs)
When coronary arteries are structurally normal or minimally diseased, MI can still occur via:
| Mechanism | Examples |
|---|---|
| Coronary vasospasm | Prinzmetal (variant) angina; cocaine or amphetamine use |
| Coronary embolism | From mural thrombus (e.g., atrial fibrillation), infective endocarditis, prosthetic valve |
| Spontaneous coronary artery dissection (SCAD) | Especially in young women, often peripartum |
| Coronary vasculitis | Kawasaki disease, polyarteritis nodosa, SLE |
| Supply-demand mismatch (Type II MI) | Severe tachycardia, hypotension, severe anemia, respiratory failure — ischemia without occlusion |
| Takotsubo (stress) cardiomyopathy | Catecholamine surge from emotional/physical stress mimicking MI |
| Hypercoagulable states | Antiphospholipid syndrome, thrombophilias |
| Severe fixed stenosis without rupture | Progressive narrowing from in-stent restenosis |
| Cocaine/stimulant use | Causes intense vasospasm and accelerates atherosclerosis |
The "Universal Definition" Framework
The Fourth Universal Definition of MI classifies causes into two main types:
- Type I MI — Atherosclerotic plaque rupture/erosion → platelet-rich thrombus → acute reduction in coronary supply. This is the classic "heart attack."
- Type II MI — Supply-demand imbalance without plaque rupture (e.g., severe anemia, tachyarrhythmia, hypotension, coronary vasospasm, embolism, SCAD).
— Fuster and Hurst's The Heart, 15th Edition; Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E
Key Modulating Factors
Even in the presence of atherosclerosis, these factors influence whether an MI actually occurs:
- Degree of collateral circulation
- Platelet reactivity and thrombotic tendency
- Level of fibrinolytic activity
- Catecholamine surges (stress, smoking, cocaine)
- Blood viscosity
- Heart rate and blood pressure at the time of plaque disruption
— Fuster and Hurst's The Heart, 15th Edition
Bottom line: The overwhelming cause is rupture of an atherosclerotic plaque in a coronary artery, triggering a clot that blocks blood flow. Modifiable risk factors (smoking, hypertension, diabetes, high cholesterol, obesity) account for the majority of preventable MIs.
This is a shared conversation. Sign in to Orris to start your own chat.