How to diagnose acral melanoma in early stages?
Reading File
search_medical_text
acral melanoma early diagnosis clinical features dermoscopy
search_medical_image
acral melanoma dermoscopy early stage
GradeResponse
GradeResponse
Early Diagnosis of Acral Melanoma
Acral melanoma (specifically acral lentiginous melanoma, ALM) arises on the palms, soles, and subungual regions. It is the most common melanoma subtype in darker-skinned populations and is frequently diagnosed late due to its hidden location and subtle early presentation. Early detection requires a combination of clinical examination, dermoscopy, and histopathology.
1. Clinical Features in Early Stages
| Feature | Early Stage Finding |
|---|---|
| Location | Sole (most common), palm, subungual (nail unit) |
| Lesion size | Often ≤ 6 mm initially, but can be smaller |
| Color | Uniform tan or light brown macule |
| Border | May appear relatively regular early on |
| Surface | Flat macule; no ulceration or nodularity |
Apply the standard ABCDE criteria with important modifications for acral sites:
- Asymmetry — often subtle at first
- Border — irregular or poorly defined margins as lesion progresses
- Color — initially uniform brown; variegation (dark brown, black, even white regression areas) suggests progression
- Diameter — > 6 mm is a classic warning sign, but early lesions may be smaller
- Evolution — any change in a palmoplantar pigmented lesion warrants evaluation
2. Dermoscopy — The Key Diagnostic Tool
Dermoscopy is the most important non-invasive tool for early acral melanoma diagnosis (Diagnosis and Management of Melanoma, p. 338).
Parallel Ridge Pattern (PRP) — Hallmark of Early ALM
The single most important dermoscopic criterion:
- Pigmentation is deposited along the ridges (elevated dermatoglyphic lines) rather than the furrows
- This is in contrast to benign acral nevi, which show the parallel furrow pattern (PFP) — pigment in the sulci (grooves)
The image below demonstrates 24-month progression of ALM in situ — note the development of the classic PRP by 24 months, along with asymmetry and multicolor variegation:
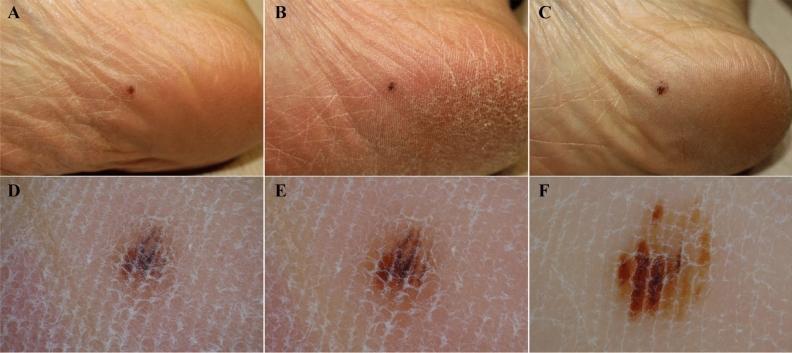
At initial visit: small, symmetric brown macule with non-typical pigmentation. At 24 months: clear PRP, multicolor variegation (light/dark brown, black), and asymmetry — diagnostic of ALM (pmc_clinical_VQA dataset).
Dermoscopic Pattern Summary
| Pattern | Lesion Type | Interpretation |
|---|---|---|
| Parallel furrow pattern | Benign acral nevus | Pigment in furrows (sulci) |
| Parallel ridge pattern (PRP) | Acral melanoma | Pigment on ridges — HIGH specificity |
| Fibrillar pattern | Benign (pressure site) | Diagonal crossing of ridges/furrows |
| Lattice-like pattern | Benign acral nevus | Combined furrow + cross lines |
| Irregular diffuse pigmentation | Suspicious/melanoma | Loss of organized pattern |
Sensitivity of PRP for ALM: ~86% | Specificity: ~99% (Saida et al.)
Additional Dermoscopic Red Flags
- Multicomponent pattern — multiple structures in one lesion
- Irregular blotches — structureless dark areas
- Regression structures — white scar-like areas or blue-gray peppering
- Vascular patterns — dotted or irregular vessels
3. Subungual Melanoma (Nail Unit)
Early subungual melanoma presents as melanonychia striata (longitudinal pigmented band in the nail):
Hutchinson's sign — periungual pigmentation extending to the proximal or lateral nail fold — is a key clinical indicator of subungual melanoma.
Dermoscopy of nail (onychoscopy):
- Irregular lines in the band (varied color, spacing, parallelism) → suspicious
- Regular parallel brown lines → more likely benign nevus or ethnic melanonychia
- Any band appearing in a patient > 50 years old, single digit, thumb/great toe, rapid change, or width > 3 mm warrants biopsy
4. Biopsy and Histopathology
Clinical + dermoscopic suspicion should always be confirmed by excisional or incisional biopsy:
- Preferred: Excisional biopsy with 1–2 mm margins (if feasible at the site)
- For large lesions on the sole: punch biopsy of the most atypical area
- Histopathologic features of early ALM:
- Atypical melanocytes along the dermoepidermal junction (lentiginous proliferation)
- Single-cell pagetoid spread within the epidermis
- Acral lentiginous growth pattern (in situ or early invasive)
- Breslow thickness < 1 mm in early-stage disease
5. Reflectance Confocal Microscopy (RCM)
An emerging non-invasive technique that provides near-histologic resolution:
- Identifies atypical melanocytes at the DEJ and epidermis
- Can help guide biopsy site selection in large or anatomically challenging lesions
- Not yet widely available but increasingly used in specialist centers
6. Practical Early Detection Algorithm
Pigmented lesion on palm / sole / nail
│
▼
Clinical exam (ABCDE + Hutchinson's sign for nail)
│
▼
Dermoscopy
├── Parallel furrow / lattice → Benign → Monitor
├── Parallel ridge pattern → HIGHLY suspicious → Biopsy
└── Irregular / multicomponent → Suspicious → Biopsy
│
▼
Excisional / punch biopsy + histopathology
│
▼
Confirm ALM → Stage → Treat
7. High-Risk Populations and Screening Tips
- Acral melanoma is not UV-related, so standard sun-exposure risk factors are less relevant
- Higher incidence in East Asian, African, and Hispanic populations — screen these groups carefully
- Regular self-examination of soles and nails is recommended, especially after age 40
- Trauma to the foot is often mistaken as the cause of pigmentation — any non-resolving pigmented lesion post-trauma must be biopsied
Early diagnosis of acral melanoma hinges on recognizing the parallel ridge pattern on dermoscopy and maintaining a low threshold for biopsy on any atypical acral or subungual pigmented lesion. Given its aggressive behavior when diagnosed late, prompt evaluation is critical.
This is a shared conversation. Sign in to Orris to start your own chat.