Give me Diabtes melitus
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have very rich content on Diabetes Mellitus. Let me compile a comprehensive answer.
Diabetes Mellitus (DM)
Definition
Diabetes mellitus is a group of metabolic diseases characterized by chronic hyperglycemia resulting from defects in insulin secretion, insulin action, or both. It is a major cardiovascular risk equivalent — nearly 80% of people with diabetes die of cardiovascular disease (CVD).
Epidemiology
- ~25.8 million people in the US have DM; 79 million have prediabetes
- 1 in 3 people with DM is undiagnosed
- 90–95% of adults have Type 2 DM
- WHO projected >350 million people with DM worldwide by 2025
- Type 2 DM is now increasingly seen in adolescents and young adults due to rising obesity
Classification
| Type | Description |
|---|---|
| Type 1 DM | Autoimmune destruction of pancreatic β-cells → absolute insulin deficiency |
| Type 2 DM | Insulin resistance + progressive β-cell failure; most common (90–95%) |
| Gestational DM | Glucose intolerance first recognized during pregnancy |
| Other specific types | Monogenic (MODY), secondary to pancreatic disease, drugs, endocrinopathies |
Diagnostic Criteria (ADA)
| Test | Diabetes | Prediabetes |
|---|---|---|
| Fasting plasma glucose (FPG) | ≥ 126 mg/dL | 100–125 mg/dL (IFG) |
| 2-hour OGTT | ≥ 200 mg/dL | 140–199 mg/dL (IGT) |
| HbA1c | ≥ 6.5% | 5.7–6.4% |
| Random glucose + symptoms | ≥ 200 mg/dL | — |
In the absence of unequivocal hyperglycemia with symptoms, diagnosis requires two abnormal test results.
Pathophysiology
Type 1 DM
- Autoimmune T-cell–mediated destruction of islet β-cells
- Results in absolute insulin deficiency
- Prone to diabetic ketoacidosis (DKA)
Type 2 DM
- Insulin resistance in peripheral tissues (skeletal muscle, liver, adipose)
- Compensatory hyperinsulinemia → eventual β-cell exhaustion
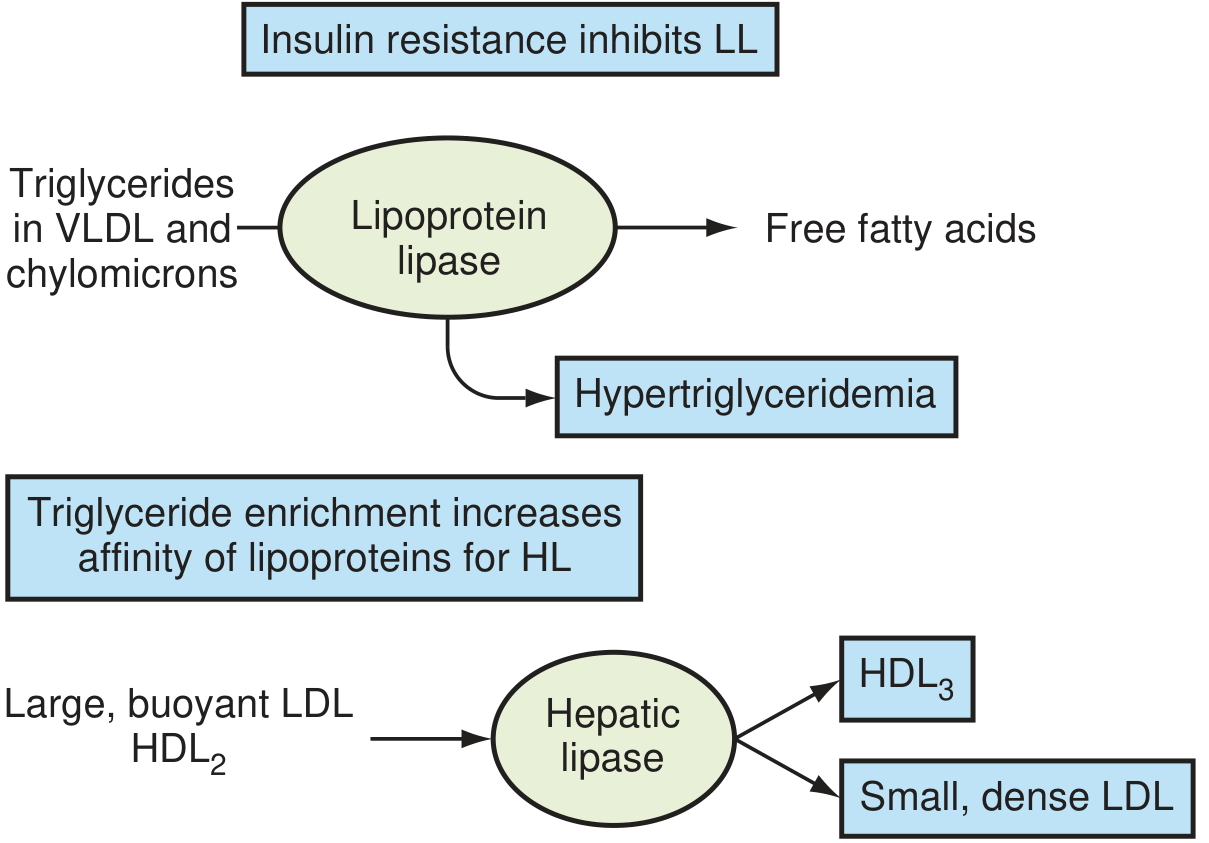
- Key pathophysiologic cascade:
- ↓ Lipoprotein lipase activity → ↑ triglycerides, ↑ VLDL, small dense LDL, ↓ HDL
- Advanced glycation end products (AGEs) damage the vasculature
- Endothelial dysfunction → accelerated atherosclerosis
Clinical Features
Symptoms of Hyperglycemia
- Polyuria, polydipsia, polyphagia
- Weight loss (especially Type 1)
- Fatigue, blurred vision, recurrent infections
Acute Complications
| Complication | Type | Key Features |
|---|---|---|
| DKA | Type 1 (mainly) | Ketones, anion gap acidosis, Kussmaul breathing |
| HHS (Hyperosmolar Hyperglycemic State) | Type 2 | Extreme hyperglycemia, no/minimal ketones, high mortality |
| Hypoglycemia | Both | Sweating, tremor, confusion; from insulin/sulfonylurea excess |
Chronic Complications
Microvascular
| Complication | Notes |
|---|---|
| Diabetic Nephropathy | Leading cause of ESRD; screen with urine microalbumin; treat with ACE inhibitors/ARBs (SOR: A) |
| Diabetic Retinopathy | Leading cause of adult-onset blindness; screen with annual dilated eye exam |
| Diabetic Neuropathy | Peripheral (glove-and-stocking), autonomic (gastroparesis, orthostatic hypotension) |
Macrovascular
| Complication | Notes |
|---|---|
| Coronary artery disease (CAD) | DM is a CAD risk equivalent — risk of MI equivalent to prior MI in non-diabetics |
| Stroke | 2–4× increased risk |
| Peripheral artery disease | Risk of lower extremity amputation |
Management
Glycemic Targets (ADA)
- HbA1c < 7% for most patients
- Tighter targets (< 6.5%) for select young, healthy patients
- Less stringent (< 8%) for elderly, high hypoglycemia risk, limited life expectancy
Lifestyle Modifications
- Weight loss (even 5–10% reduces insulin resistance significantly)
- Aerobic exercise ≥150 min/week
- Mediterranean or low-glycemic diet
- Smoking cessation
Pharmacotherapy
Oral Agents
| Drug Class | Mechanism | Notes |
|---|---|---|
| Metformin | ↓ Hepatic glucose production | First-line; weight-neutral; avoid in severe renal failure |
| Sulfonylureas (glipizide, glyburide) | Stimulate insulin secretion | Risk of hypoglycemia and weight gain |
| Thiazolidinediones (pioglitazone) | PPAR-γ agonist → ↑ insulin sensitivity | Risk of fluid retention, HF |
| DPP-4 inhibitors (sitagliptin) | Increase incretin activity | Weight-neutral, well tolerated |
| SGLT-2 inhibitors (empagliflozin, dapagliflozin) | ↑ Urinary glucose excretion | Cardio- and renoprotective benefits; preferred in HF/CKD |
| GLP-1 agonists (liraglutide, semaglutide) | Enhance insulin, suppress glucagon | Weight loss, CV benefit; injectable or oral |
| Alpha-glucosidase inhibitors (acarbose) | Delay carbohydrate absorption | GI side effects |
| Orlistat | Lipase inhibitor → ↓ fat absorption | Weight management adjunct |
Insulin
- Required in Type 1; used in advanced Type 2
- Types: basal (glargine, detemir), prandial (lispro, aspart), premixed
- Initiate basal insulin when oral agents fail to achieve HbA1c targets
Comorbidity Management (Aggressive Risk Reduction)
| Target | Goal | Treatment |
|---|---|---|
| Blood pressure | < 130/80 mmHg | ACE inhibitor or ARB preferred (especially with nephropathy) |
| LDL cholesterol | < 70 mg/dL (high-risk) | High-intensity statin (e.g., atorvastatin) — CARDS trial |
| Triglycerides | < 150 mg/dL | Fibrates, omega-3 fatty acids |
| Nephropathy | Microalbuminuria screening | ACE inhibitor/ARB; reduces progression to ESRD |
| Retinopathy | Annual dilated fundus exam | Laser photocoagulation if proliferative |
| Foot care | Annual monofilament exam | Podiatry referral, offloading, wound care |
| Cardiovascular | Aspirin 81 mg/day | For primary prevention in high-risk patients |
Monitoring
| Parameter | Frequency |
|---|---|
| HbA1c | Every 3 months (uncontrolled), every 6 months (controlled) |
| Fasting lipid panel | Annually |
| Urine microalbumin / creatinine ratio | Annually |
| Dilated eye exam | Annually |
| Foot exam | Every visit |
| Blood pressure | Every visit |
| Serum creatinine / GFR | Annually |
Key Takeaways
- DM is a CAD risk equivalent — treat all cardiovascular risk factors aggressively
-
75% of people with DM die from macrovascular complications
- Tight glycemic, BP, and lipid control to ADA targets is the cornerstone of management
- Nephropathy must be screened for and treated with ACE inhibitors or ARBs
- SGLT-2 inhibitors and GLP-1 agonists have proven cardiovascular and renal benefits beyond glucose lowering
- Bariatric surgery in morbidly obese patients can achieve near-remission of Type 2 DM
Sources: Textbook of Family Medicine 9e (pp. 667–680); Brenner and Rector's The Kidney; ADA Standards of Medical Care in Diabetes
This is a shared conversation. Sign in to Orris to start your own chat.