Botox in Ophthalmology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I have enough information to compile a comprehensive answer. Let me synthesize all the retrieved content.
Botulinum Toxin (Botox) in Ophthalmology
Mechanism of Action
Botulinum toxin type A (BoNT-A) blocks acetylcholine release at the neuromuscular junction by cleaving SNAP-25, a protein essential for vesicle fusion. This causes temporary, dose-dependent paralysis of locally injected muscles. The effect is reversible — axonal sprouting and re-innervation restore function over weeks to months.
Several BoNT-A preparations are marketed:
- OnabotulinumtoxinA (Botox®)
- AbobotulinumtoxinA (Dysport®)
- PrabotulinumtoxinA (Jeuveau®)
- IncobotulinumtoxinA (Xeomin®)
Botox was the first FDA-approved clinical application of botulinum toxin — specifically for strabismus and blepharospasm — before its widely-known cosmetic uses.
— Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 1487
Ophthalmic Indications
1. Strabismus (Squint)
BoNT-A injection into an overacting extraocular muscle weakens it, allowing the antagonist to re-establish alignment. It is used:
- As primary treatment for small-to-moderate angle deviations
- As an adjunct or alternative to surgery, particularly in:
- Acute acquired comitant esotropia
- Sixth nerve (abducens) palsy — injection into the medial rectus prevents contracture while waiting for neurological recovery
- Post-surgical over- or under-correction
- Consecutive exotropia
- Under EMG guidance to confirm needle placement in the target muscle
The therapeutic benefit may outlast the pharmacological paralysis due to re-establishment of sensory fusion during the period of alignment.
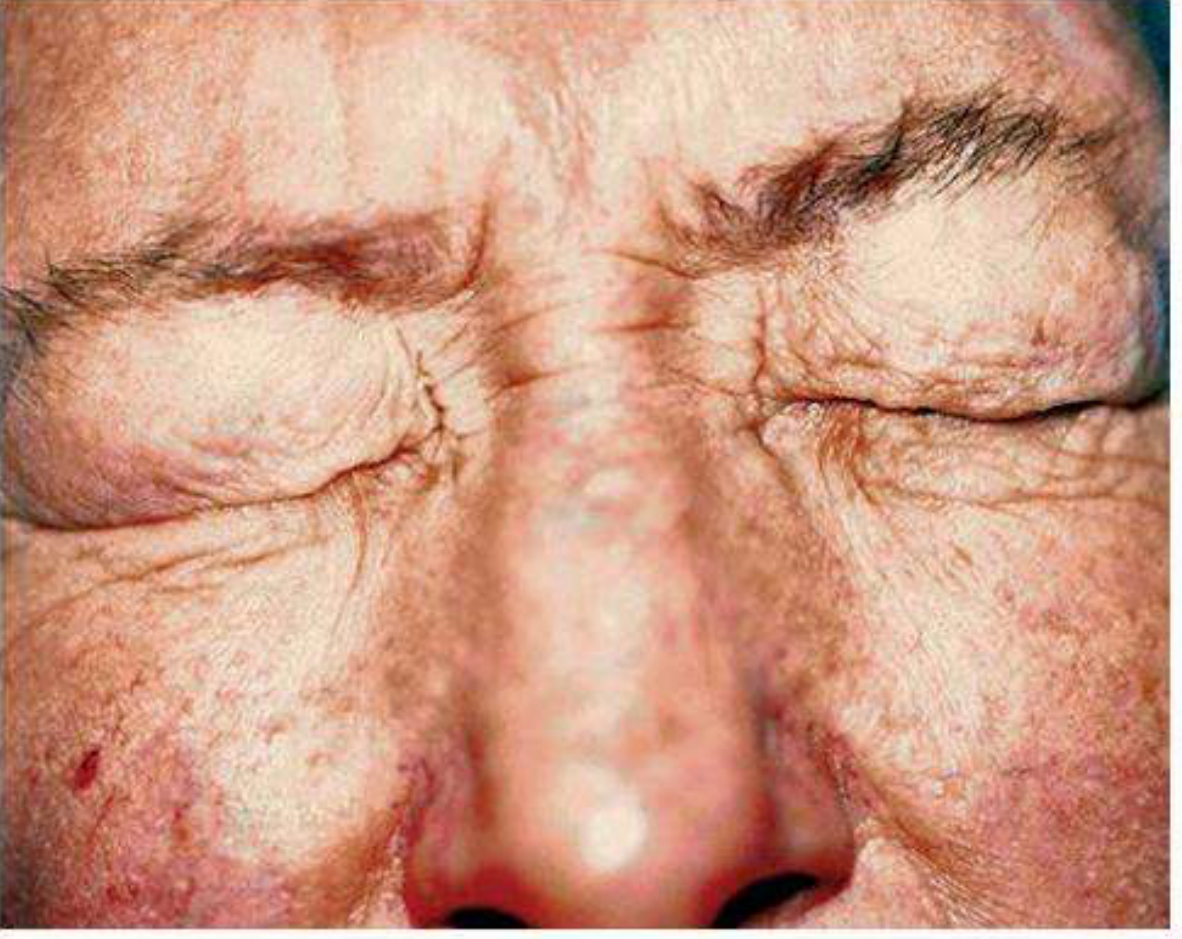
2. Essential Blepharospasm
Essential blepharospasm is a bilateral involuntary spasm of orbicularis oculi and upper facial muscles, presenting in the 6th decade with female predominance. It can cause functional blindness in severe cases, triggered by stress and bright light.
Botulinum toxin is the treatment of choice:
- 2.5–5 units injected subcutaneously at 3–4 periocular sites per side
- Achieves relief in ~95% of patients
- Repeat injections needed every ~3 months
- Surgery (orbicularis myectomy) reserved for non-responders
3. Hemifacial Spasm
A unilateral condition with initial orbicularis spasm that spreads along the facial nerve distribution, typically idiopathic but may indicate CN VII compression. Treatment is the same as for blepharospasm — periocular BoNT-A injections every 3 months.
4. Meige / Brueghel Syndrome
Blepharospasm combined with oromandibular dystonia. BoNT-A injection is the cornerstone of management here as well.
5. Other Ophthalmic / Periocular Uses
| Indication | Rationale |
|---|---|
| Thyroid eye disease (restrictive myopathy) | Temporary alignment correction or relief of diplopia while awaiting orbital decompression |
| Nystagmus | Retrobulbar injection to dampen oscillations (limited use) |
| Ptosis repair adjunct | Temporary lid elevation to protect the cornea post-lower lid surgery |
| Facial wrinkles / periocular aesthetics | Glabellar lines, crow's feet (cosmetic, widely used) |
| Lacrimal hypersecretion | Injection into lacrimal gland to reduce tearing in crocodile tears syndrome |
| Corneal exposure | Inducing temporary ptosis to protect a compromised cornea |
Injection Technique (Blepharospasm)
- Sites: Subcutaneous injection at the pre-tarsal orbicularis (upper and lower lids) and the lateral canthal area; typically 3–4 sites per eye
- Dose: 2.5–5 units onabotulinumtoxinA per site; total ~15–25 units per eye
- Strabismus: Injection under EMG guidance directly into the extraocular muscle (e.g., medial rectus for esotropia)
- Onset: 2–4 days; peak effect: 1–2 weeks; duration: 2–4 months
Adverse Effects
| Effect | Notes |
|---|---|
| Ptosis | Most common; from toxin diffusion to levator palpebrae |
| Lagophthalmos | Incomplete lid closure → dry eye, exposure keratopathy |
| Diplopia | Toxin spread to adjacent extraocular muscles |
| Dry eye | Reduced blink + lagophthalmos |
| Ecchymosis / bruising | At injection sites |
| Distant toxin spread | Rare but potentially life-threatening; dysphagia, respiratory compromise |
Ptosis from inadvertent BoNT-A injection can mimic ocular myasthenia gravis on the ice test — an important pitfall in clinical diagnosis.
— Localization in Clinical Neurology, 8e
Key Points
- Botulinum toxin was originally developed for ophthalmic indications — strabismus and blepharospasm were the first approved uses (FDA approved 1989)
- Effect is temporary and reversible — repeat injections every 3 months are standard
- For blepharospasm: success rate ~95%; myectomy is rarely needed
- For strabismus: most effective for small angles and acute palsies; less reliable for large-angle congenital deviations
- Resistance (antibody formation) can develop with frequent, high-dose injections — newer preparations (incobotulinumtoxinA) are complexing-protein-free to reduce this risk
— Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.