minimally invasive percutaneous plate osteosynthesis recent advances
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information to provide a thorough answer. Let me compile this into a well-structured response.
Minimally Invasive Percutaneous Plate Osteosynthesis (MIPO): Recent Advances
Concept and Biological Rationale
MIPO is a technique in which a plate is placed in the submuscular plane by sliding it through small incisions proximal or distal to a fracture, entirely avoiding exposure of the fracture site. The fundamental goal is to preserve the fracture hematoma and periosteal blood supply, allowing secondary (callus) bone healing rather than primary (cortical) healing.
Key biological advantages:
- Decreased soft tissue and biological compromise
- Better retention of medullary and periosteal perfusion
- Preservation of fracture hematoma (osteogenic environment)
- Reduced infection risk from extensive dissection
— Miller's Review of Orthopaedics, 9th Edition, p. 897
Indications Across Anatomical Sites
Humeral Shaft Fractures
MIPO was introduced as an advancement over conventional ORIF, and it challenges intramedullary nailing (IMN) by:
- Avoiding violation of the rotator cuff (vs. antegrade nailing)
- Eliminating risk of supracondylar iatrogenic fracture (vs. retrograde nailing)
- Preserving fracture hematoma (vs. ORIF)
Comparison data (An et al., Oh et al., multiple meta-analyses) show MIPO achieves:
- Lower rate of iatrogenic radial nerve palsy compared to ORIF
- Accelerated fracture union
- Comparable functional outcomes (shoulder/elbow ROM and scores)
- Reduced perioperative blood loss
— Rockwood & Green's Fractures in Adults, 10th ed. 2025, p. 1467–1475
Distal Femur
MIPO using locked condylar plates applied percutaneously through a small lateral incision has largely replaced conventional plating, preserving the lateral soft tissue envelope and reducing wound complications.
— Rockwood & Green's Fractures in Adults, 10th ed. 2025
Ankle/Fibula
MIPO for distal fibular fractures uses a 2–3 cm distal wound and 3–4 cm proximal wound. It reduces soft tissue complications in a particularly vulnerable envelope, though technically demanding. Nonunion remains a risk with poor technique.
— Rockwood & Green's Fractures in Adults, 10th ed. 2025, p. 3318
Surgical Approaches (Humerus as Model)
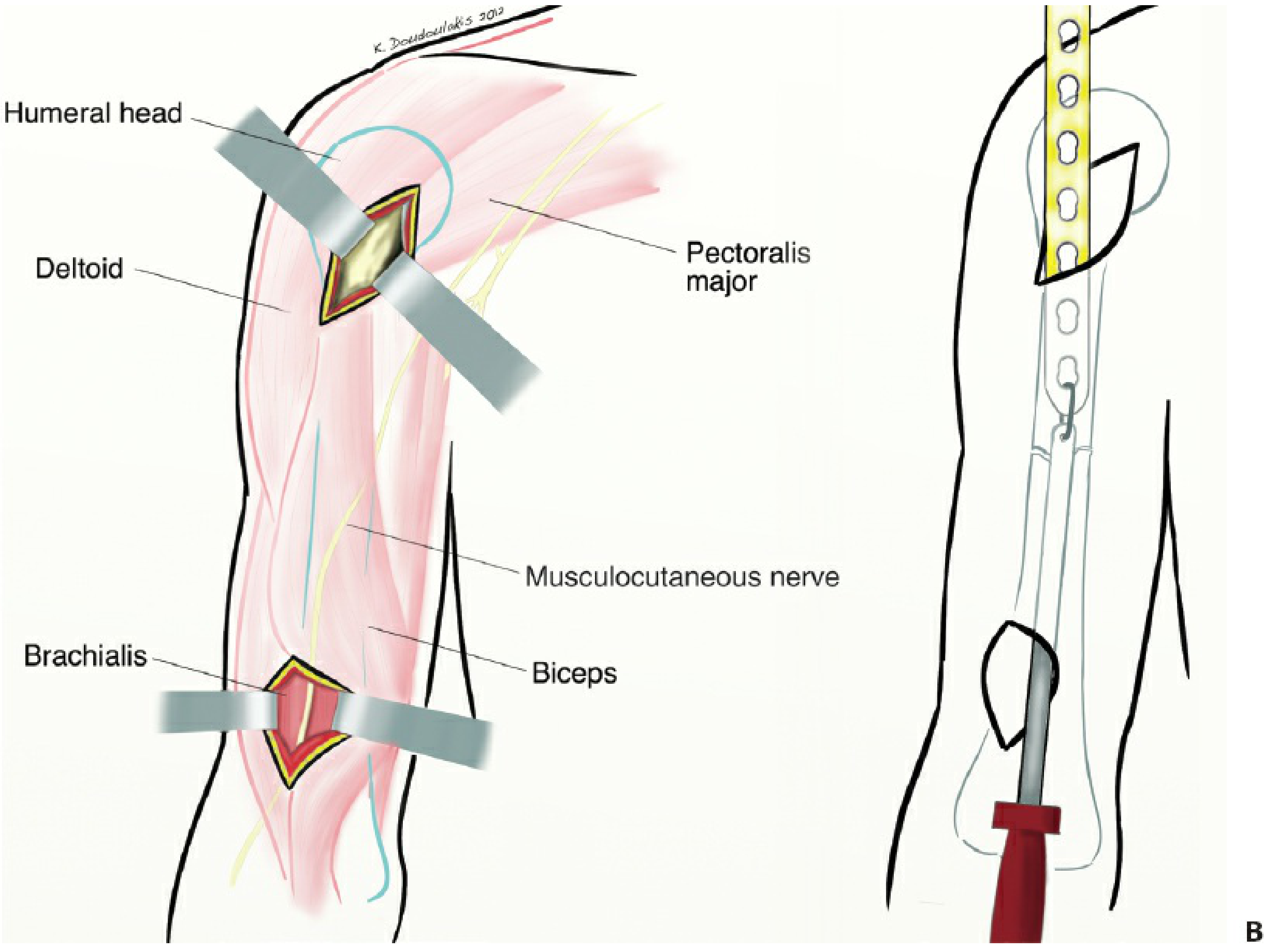
Anterior Approach (most popular)
- Two incisions: proximal (3–5 cm, between lateral biceps and medial deltoid) and distal (3–5 cm, lateral border of biceps, 5 cm proximal to elbow crease)
- Interval: biceps–brachialis; brachialis split longitudinally
- Musculocutaneous nerve protected with medial brachialis half; radial nerve with lateral half
- Full forearm supination reduces nerve proximity risk
Lateral Approach
- Proximal incision: 3 cm below acromion; distal: between brachioradialis and brachialis
- Optional middle window to guide plate passage
- Thin muscle layer left beneath plate to prevent direct radial nerve contact
Posterior Approach
- Proximal window: 5 cm, posterior border of deltoid
- Requires careful radial nerve identification and protection
— Rockwood & Green's Fractures in Adults, 10th ed. 2025, p. 1467
Integration with Locking Plate Technology
The most significant recent advance is the combination of MIPO technique with locking plate constructs:
| Feature | Conventional Plate | Locking Plate (MIPO) |
|---|---|---|
| Stability mechanism | Friction (plate–bone compression) | Fixed-angle (locked screws) |
| Failure mode | Sequential | Simultaneous (stronger construct) |
| Utility in osteoporosis | Poor | Excellent |
| Periosteal blood flow | Compromised under plate | Preserved |
Locking plates used percutaneously via MIPO are most valuable in:
- Osteoporotic bone
- Short metaphyseal segments (proximal humerus, distal femur, proximal tibia)
- Periprosthetic fractures
- Intra-articular distal femur and proximal tibia
Polyaxial locking systems (variable-angle screws) represent a further refinement, allowing screw trajectory adjustment to avoid hardware from prior surgery or anatomical variants.
— Miller's Review of Orthopaedics, 9th ed., p. 897; Rockwood & Green, 2025
Preoperative Planning Requirements
MIPO requires rigorous preoperative planning not needed for ORIF:
- Confirm fracture lines do not extend into metaphyseal zones (CT if uncertain)
- Pre-decide approach, plate length, and screw configuration
- Identify structures at risk along the planned tunnel
- Plan fluoroscopic views to confirm reduction percutaneously
- Have ORIF as a backup — experienced surgeons only
Technical Pitfalls and How to Avoid Them
| Pitfall | Prevention |
|---|---|
| Malreduction/malrotation | Use fluoroscopy (AP + lateral), check rotational landmarks (cortical thickness, matching fracture edges) |
| Nerve injury (radial, musculocutaneous) | Understand safe zones; open approach if anatomy uncertain |
| Plate malpositioning | Use tunneling instruments; confirm with intraoperative imaging |
| Radiation exposure | Optimize C-arm positioning before draping |
| Nonunion | Avoid excessive working length; ensure bridging plate spans at least 2–3 fracture widths |
Current Controversies and Future Directions
The field has matured beyond early enthusiasm, with emerging nuance:
-
MIPO vs. IMN: For humeral shaft fractures, MIPO challenges IMN by avoiding rotator cuff injury, but IMN remains preferred for certain patterns. Meta-analyses show no clear superiority of either in union rates.
-
ORIF still has a role: A well-performed open procedure is often faster and safer than a poorly executed MIPO — the technique should not be used unless the surgeon is experienced and a clear benefit exists.
-
Patient-specific selection: Emerging evidence suggests treatment choice should be driven more by fracture pattern, location, and patient factors (age, comorbidities, occupation) than surgeon preference.
-
Novel indications: MIPO has been applied to pathologic/metastatic lesions of the humerus (Chou et al.), periprosthetic fractures around ankle and shoulder arthroplasties, and high-risk soft tissue injuries where conventional open exposure would be prohibitive.
-
Implant innovation: New nail designs, anatomically pre-contoured MIPO plates, and less traumatic insertion systems continue to reduce intraoperative difficulty.
"While surgical techniques and implants are emerging and improving (locking plates, MIPO, new nail designs, and less traumatic approaches), there remains a debate among the supporters of each treatment method." — Rockwood & Green's Fractures in Adults, 10th ed. 2025, p. 1495
Summary
MIPO represents a paradigm shift from anatomy-exposing fixation to biology-preserving fixation. Its core advance — plate delivery through a submuscular tunnel without fracture site exposure — reduces infection, nonunion, and blood loss. When combined with modern locking plate technology and polyaxial screw systems, it provides mechanically sound, biologically respectful fixation especially valuable in osteoporotic bone, metaphyseal fractures, and high-risk soft tissue zones. The current frontier involves refining patient selection criteria, standardizing surgical training, and expanding indications to periprosthetic and oncological settings.
give this as exam answer 15 marks
Minimally Invasive Percutaneous Plate Osteosynthesis (MIPO) — Recent Advances
Definition and Concept
MIPO is a surgical technique in which a plate is inserted through small incisions proximal and/or distal to a fracture and tunneled in the submuscular plane, without exposing or disturbing the fracture site. It is based on the principle of biological fixation — preserving the fracture hematoma, periosteal blood supply, and soft tissue envelope to promote secondary (callus) bone healing.
Biological Rationale
The technique exploits the concept of relative stability:
- Fracture hematoma is an osteogenic environment — its preservation accelerates callus formation
- Periosteal and medullary perfusion are better retained than in conventional ORIF
- Reduced devitalization of bone fragments
- Lower rates of infection and wound breakdown due to minimal dissection
Indications
| Region | Fracture Type |
|---|---|
| Humeral shaft | Diaphyseal fractures (mid and distal third) |
| Proximal humerus | 3–4 part fractures with polyaxial locking plates |
| Distal femur | Metaphyseal and intra-articular fractures |
| Proximal tibia | Periarticular fractures |
| Ankle/Fibula | Distal fibular fractures with compromised soft tissue |
| Periprosthetic | Fractures around shoulder/ankle arthroplasty |
| Pathological | Metastatic humeral lesions |
Surgical Approaches (Humerus as the Standard Model)
1. Anterior Approach (most commonly used)
- Two incisions: proximal (3–5 cm, between lateral biceps and medial deltoid) and distal (3–5 cm, lateral border of biceps, 5 cm above elbow crease)
- Brachialis split longitudinally; musculocutaneous nerve retracted with medial half, radial nerve protected by lateral half
- Full forearm supination recommended to reduce nerve risk
2. Lateral Approach
- Proximal window below acromion; distal window between brachioradialis and brachialis
- An optional middle window facilitates plate passage
- A thin muscle layer is left beneath the plate to prevent direct radial nerve contact
3. Posterior Approach
- Used for distal third fractures
- Two windows; radial nerve must be identified and protected in the proximal window before plate passage
Preoperative Planning
- CT scan mandatory if fracture lines approach metaphysis
- Pre-decide approach, plate length, screw number, and configuration
- Identify all structures at risk along the planned submuscular tunnel
- Experienced surgeon only — ORIF should be available as backup
- Fluoroscopy positioning confirmed before draping
Recent Advances
1. Locking Plate Technology
The most significant advance — MIPO combined with locked plating transforms the construct:
| Feature | Conventional Plate | Locking Plate via MIPO |
|---|---|---|
| Stability mechanism | Friction (plate–bone) | Fixed-angle locked screws |
| Failure mode | Sequential | Simultaneous (stronger) |
| Osteoporotic bone | Poor grip | Excellent stability |
| Periosteal blood supply | Compressed under plate | Fully preserved |
Most useful in: osteoporotic bone, short metaphyseal segments, periprosthetic fractures, intra-articular distal femur and proximal tibia.
2. Polyaxial (Variable-Angle) Locking Systems
- Screws can be directed at varying trajectories, not fixed angles
- Allows screw placement around prior hardware, implants, or anatomical variants
- Permits better bone purchase in comminuted or osteoporotic fragments
3. Anatomically Pre-Contoured Plates
- Site-specific plates (proximal humerus, distal femur, lateral tibial plateau) designed to slide and seat without intraoperative contouring
- Reduces operative time and improves plate–bone apposition percutaneously
4. Robotic and Computer-Assisted Navigation
- Emerging use of fluoroscopy-based navigation to confirm reduction without open exposure
- Reduces radiation exposure and improves alignment accuracy in MIPO procedures
5. Expanded Indications
- Pathological/metastatic fractures: MIPO plating applied to metastatic humeral lesions avoids large incisions in immunocompromised patients
- Periprosthetic fractures: MIPO used around shoulder and ankle arthroplasty stems where soft tissue is scarred
- Geriatric fractures: Growing use in elderly osteoporotic patients with distal femur and proximal tibia fractures where conventional ORIF carries high wound complication risk
Pitfalls and How to Avoid Them
| Pitfall | Prevention |
|---|---|
| Malreduction / malrotation | Intraoperative fluoroscopy; assess cortical thickness and rotational landmarks |
| Nerve injury (radial, musculocutaneous) | Know safe zones; open approach if anatomy is uncertain |
| Plate malpositioning | Use dedicated tunneling instruments; confirm with biplanar imaging |
| Nonunion | Adequate working length; bridge plate must span 2–3× fracture zone width |
| Increased radiation exposure | Optimize C-arm setup before draping; use navigation where available |
MIPO vs. ORIF vs. IMN — Current Evidence
- MIPO vs. ORIF (humeral shaft): MIPO shows lower iatrogenic radial nerve palsy, faster union, similar functional outcomes
- MIPO vs. IMN: MIPO avoids rotator cuff injury (vs. antegrade nail) and supracondylar iatrogenic fracture (vs. retrograde nail); union rates comparable
- Current consensus: No technique is universally superior — selection should be driven by fracture pattern, location, bone quality, and patient factors (age, comorbidities, occupation) rather than surgeon preference alone
Controversies and Future Directions
- Lack of consensus on screw number, working length, and hybrid (locking + non-locking) screw configurations
- Role of MIPO in segmental and highly comminuted fractures still debated
- Trend is toward early mobilization and enhanced recovery protocols — MIPO aligns well with this philosophy
- A well-performed ORIF remains preferable to a poorly executed MIPO — technique should not be applied without adequate surgical experience
"Trauma surgeons are moving away from MIPO procedures when they do not offer a clear benefit. Sometimes, a well-performed open procedure is quicker and much safer than percutaneous or minimally invasive procedures." — Rockwood & Green's Fractures in Adults, 10th ed. 2025
Conclusion
MIPO represents a fundamental shift from anatomy-exposing to biology-preserving fixation. Its combination with locking plates, polyaxial screw systems, and pre-contoured implants has made it the preferred technique for periarticular fractures, osteoporotic bone, and compromised soft tissue zones. The ongoing advances in implant design, navigation, and patient-specific planning continue to expand its applications while refining its indications.
This is a shared conversation. Sign in to Orris to start your own chat.