hypoxia , types and explainations • chyne stokes breathing(physiology basis, pattern of breathing and conditions) -biots breathing(physiological basis, pattern and conditions) Sometimes chyne stokes and biots are togetherly asked as periodic breathing
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
I have all the information I need. Let me now compile a thorough, well-organized answer.
HYPOXIA - Types and Explanations
Definition
Hypoxia is a state in which oxygen delivery to tissues is inadequate for their metabolic needs, or tissues are unable to use available oxygen.
Classification of Hypoxia
There are two major classification frameworks used in physiology and clinical medicine.
Framework 1: Ganong / Classic 4-Type Classification
(Ganong's Review of Medical Physiology)
| Type | Also Called | Core Problem |
|---|---|---|
| Hypoxic hypoxia | Hypoxemia | Low arterial PO2 |
| Anemic hypoxia | - | Normal PO2 but reduced O2-carrying capacity |
| Ischemic/Stagnant hypoxia | - | Low blood flow to tissues |
| Histotoxic hypoxia | - | Tissues cannot use O2 despite adequate delivery |
Framework 2: Guyton's Descriptive Classification
(Guyton and Hall Textbook of Medical Physiology)
1. Inadequate oxygenation of blood in the lungs - Extrinsic causes
- Deficiency of O2 in the atmosphere (e.g., high altitude)
- Hypoventilation due to neuromuscular disorders
2. Pulmonary disease
- Hypoventilation from increased airway resistance or decreased compliance (e.g., asthma, COPD)
- Abnormal ventilation-perfusion (V/Q) ratio - including increased physiological dead space or physiological shunt
- Diminished respiratory membrane diffusion (e.g., pulmonary fibrosis, pulmonary edema)
3. Venous-to-arterial shunts - right-to-left cardiac shunts (congenital heart disease)
4. Inadequate O2 transport by blood
- Anemia or abnormal hemoglobin (e.g., CO poisoning, methemoglobinemia)
- General circulatory deficiency (e.g., heart failure, shock)
- Localized circulatory deficiency (peripheral vascular disease, stroke, MI)
- Tissue edema (increases diffusion distance from capillary to cell)
5. Inadequate tissue capability to use O2 (Histotoxic)
- Poisoning of cellular oxidation enzymes (classic example: cyanide poisoning - blocks cytochrome oxidase)
- Deficiencies of oxidative enzymes (e.g., beriberi - vitamin B1 deficiency disrupts tissue O2 utilization and CO2 production)
The 4 Classic Types - Detailed
1. Hypoxic Hypoxia (Hypoxemia)
- Mechanism: Insufficient O2 reaches the blood. Both arterial O2 content AND tension (PaO2) are low.
- Causes: High altitude, V/Q mismatch, diffusion impairment, hypoventilation, right-to-left shunts, low FiO2
- Response: Cerebral blood flow increases to compensate. If CBF cannot increase sufficiently (~2x normal), cerebral metabolic rate of O2 (CMRO2) falls and symptoms emerge.
- O2 therapy: Highly effective (corrects the low alveolar PO2 directly)
2. Anemic Hypoxia
- Mechanism: Arterial PO2 is normal, but O2-carrying capacity of blood is reduced - less hemoglobin available or Hb is non-functional.
- Causes: Iron deficiency anemia, pernicious anemia, CO poisoning (forms carboxyhemoglobin), methemoglobinemia, sickle cell disease
- O2 therapy: Partially useful - dissolved O2 in plasma increases (7-30% extra transport), which can sometimes be life-saving, but the Hb-bound transport is barely altered.
3. Ischemic (Stagnant) Hypoxia
- Mechanism: Blood flow to a tissue is so low that adequate O2 is not delivered, despite normal PaO2 and normal Hb concentration.
- Causes: Heart failure, cardiogenic shock, arterial occlusion, severe hypotension, localized ischemia (e.g., limb ischemia, cerebral ischemia)
- O2 therapy: Limited benefit - the problem is delivery failure, not content failure. Some extra dissolved O2 may help marginally.
4. Histotoxic Hypoxia
- Mechanism: O2 is delivered adequately to tissues but cells cannot use it - the cellular machinery for O2 utilization is poisoned or impaired.
- Key feature: Normal arterial AND venous O2 levels (venous blood remains oxygenated because tissues cannot extract O2)
- Causes:
- Cyanide poisoning - directly blocks cytochrome oxidase (complex IV of the electron transport chain)
- Carbon monoxide (high-dose) - also impairs intracellular cytochrome function
- Beriberi (Vitamin B1/thiamine deficiency) - disrupts key steps in tissue oxidation and CO2 formation
- Certain mitochondrial toxins
- O2 therapy: Of little to no value (tissues cannot use the O2 regardless of how much is delivered)
Effects of Hypoxia
- Mild/moderate: Increased cerebral blood flow, compensatory hyperventilation, release of HIFs (hypoxia-inducible factors) which upregulate erythropoietin, angiogenic factors
- Moderate-severe: Depressed mental activity, impaired muscle work capacity
- Severe: Cell death throughout the body; cerebral hypoxia leads to coma and death
PERIODIC BREATHING
Periodic breathing is the umbrella term for abnormal rhythmic variations in breathing depth and rate, which cycle repeatedly. The two main types are Cheyne-Stokes breathing and Biot's breathing.
Cheyne-Stokes Breathing
Pattern
A gradually waxing (crescendo) then waning (decrescendo) pattern of breathing, classically cycling every 40-60 seconds, with periods of central apnea at the nadir. The apnea phase is followed by the next crescendo.
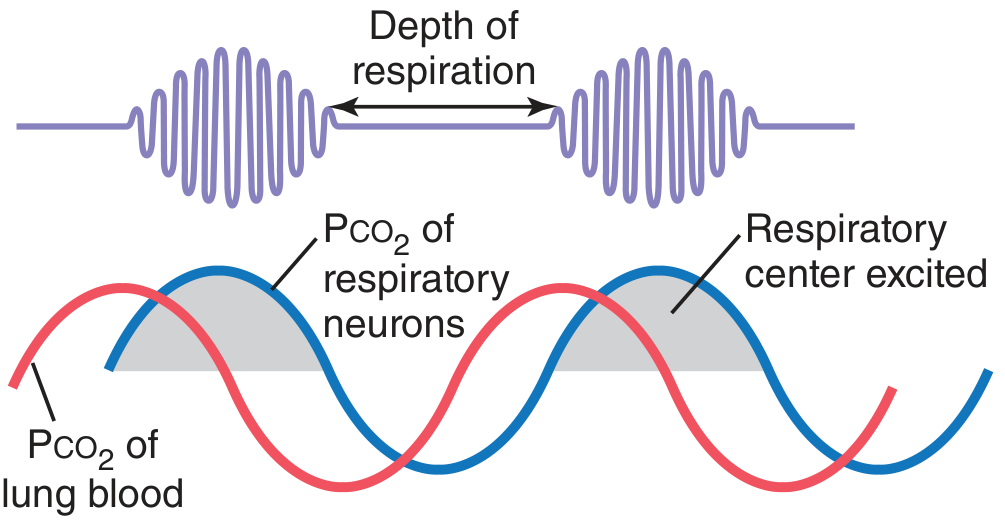
Fig 42.12 from Guyton and Hall: The red line = PCO2 in lung blood; the blue line = PCO2 reaching respiratory center neurons. Note the phase lag - this delay drives the oscillation.
Physiological Basis
(Guyton and Hall)
The mechanism arises from a feedback control loop with excessive delay or excessive gain:
Step-by-step cycle:
- The person overbreathes (hyperventilates) - blowing off CO2 and raising O2 in pulmonary blood.
- It takes several seconds for this altered blood to travel from the lungs to the brainstem respiratory center.
- During this transit delay, the person continues to overbreathe.
- When the low-CO2, high-O2 blood finally reaches the respiratory center, it suppresses ventilation excessively - causing apnea or very shallow breathing.
- During apnea, CO2 builds up and O2 falls in the alveoli again.
- Again, there is a delay before this new blood (now high CO2, low O2) reaches the brain.
- When it does, the respiratory center is stimulated excessively - causing hyperventilation.
- The cycle repeats.
Why doesn't this happen in normal people?
The large "buffer" of dissolved and chemically-bound CO2/O2 in blood and tissues normally damps these oscillations. It takes an amplifying condition to override this damping.
Two Conditions That Produce Cheyne-Stokes Breathing
Condition 1 - Prolonged circulation time (lung-to-brain delay):
- The blood takes longer than normal to travel from lungs to brain.
- By the time altered blood reaches the brain, the alveolar gas changes have become extreme.
- Classic cause: severe cardiac failure (low cardiac output = slow blood flow)
- Can persist on and off for months in chronic heart failure.
Condition 2 - Increased feedback gain in respiratory control centers:
- A small rise in PCO2 triggers a disproportionately large ventilatory response (e.g., 10-20x increase instead of the normal 2-3x).
- Even without a circulatory delay, the system oscillates.
- Classic cause: brain damage to respiratory centers (often turns off breathing completely then restimulates it forcefully)
- Also seen at high altitude (hypoxia increases chemoreceptor sensitivity).
Neurological Localization
- Cheyne-Stokes respiration localizes to bilateral hemispheric or diencephalic dysfunction, or bilateral damage anywhere along the descending pathway from forebrain to upper pons.
- A continuous Cheyne-Stokes pattern is relatively a good prognostic sign (permanent brainstem damage has not occurred).
- Emergence of Cheyne-Stokes in a patient with a unilateral mass lesion is an early warning of transtentorial herniation.
- Patients are more alert during the hyperpneic (waxing) phase and less alert during the apneic phase.
Clinical Conditions Associated with Cheyne-Stokes
| Category | Examples |
|---|---|
| Cardiac | Congestive heart failure (most common), atrial fibrillation |
| Neurological | Bilateral hemispheric damage, diencephalic lesions, post-stroke, herniation |
| Metabolic/Toxic | Uremia, morphine/opioid use |
| High altitude | Periodic breathing during sleep at altitude |
| Sleep | Central sleep apnea with Cheyne-Stokes (classified in ICSD) |
Risk factors for Cheyne-Stokes in heart failure: Male sex, advanced age, low baseline PaCO2, atrial fibrillation.
Biot's Breathing
Historical Note
First described in 1876 by Camille Biot in patients with severe meningitis.
Pattern
- Breaths of nearly equal volume separated by periods of apnea (unpredictable, variable length apneas).
- The breathing is irregular (ataxic) - each breath may vary in rate and depth.
- No orderly crescendo-decrescendo; abrupt onset and cessation of breathing clusters.
- Apnea length is often greater than the ventilatory phase.
Physiological Basis
- Biot's breathing results from damage to the dorsomedial medulla - the part of the medullary reticular formation that generates and coordinates the respiratory rhythm.
- When the medullary respiratory rhythm generator is disrupted, breathing becomes chaotic, irregular, and unpredictable rather than the smooth oscillations of Cheyne-Stokes.
- This is a fundamentally different mechanism from Cheyne-Stokes: it is not a feedback loop problem - it is structural damage to the rhythm-generating apparatus itself.
Neurological Localization
- Medullary dysfunction (dorsomedial reticular formation)
- Indicates a lesion at the level of the medulla oblongata
Clinical Conditions
| Category | Examples |
|---|---|
| CNS infections | Bacterial meningitis (Biot's original description), encephalitis |
| Raised ICP | Severe raised intracranial pressure, herniation at medullary level |
| Structural | Medullary tumors, hemorrhage into medulla, medullary infarction |
| Late herniation | Terminal brainstem herniation (ominous sign) |
| Drugs | Opioid overdose (can cause ataxic breathing) |
Cheyne-Stokes vs Biot's - Comparison Table (Periodic Breathing)
| Feature | Cheyne-Stokes | Biot's (Ataxic) |
|---|---|---|
| Pattern | Crescendo-decrescendo (smooth waxing/waning) | Irregular, equal-amplitude breaths with unpredictable apneas |
| Apnea | Regular, at the nadir of the cycle | Irregular, may be longer than breathing phase |
| Cycle length | ~40-60 seconds | No fixed cycle |
| Mechanism | Feedback loop: delayed chemoreceptor response + prolonged circulation time or increased gain | Direct structural damage to medullary rhythm generator |
| Lesion site | Bilateral forebrain/diencephalon to upper pons | Dorsomedial medulla |
| Classic conditions | Cardiac failure, bilateral hemisphere damage, high altitude | Meningitis, raised ICP, medullary lesions |
| Prognosis | Relatively better (brainstem intact) | Ominous - indicates severe medullary compromise |
| O2/CO2 role | Central to the mechanism | Not the primary driver |
Neurological Respiratory Pattern Localization Chart
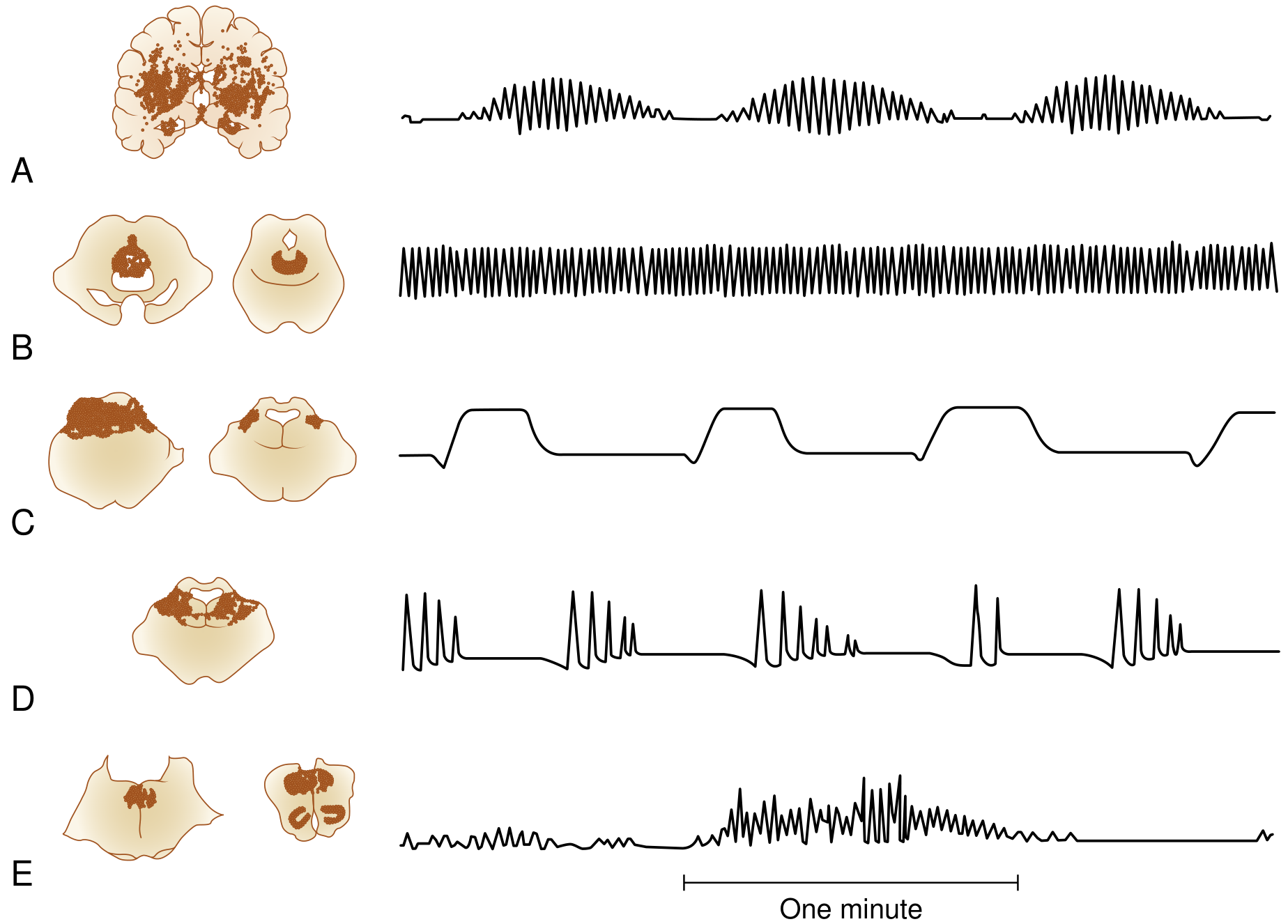
Fig 5.1 from Bradley and Daroff's Neurology: Lesion sites (shaded) with corresponding breathing tracings. Row A = Cheyne-Stokes, Row E = Ataxic/Biot's breathing.
Important Exam Note: Terminology Confusion
A common source of confusion: the pattern sometimes called "Biot's breathing" in clinical settings (short bursts of 7-10 rapid breaths then apnea, without waxing/waning) has been incorrectly labeled. What Biot actually described was ataxic breathing - truly irregular, variable amplitude. The misapplied term refers more accurately to cluster breathing (lower pontine lesion). Both Cheyne-Stokes and Biot's are grouped under "periodic breathing" when asked together in exams.
Sources:
- Guyton and Hall Textbook of Medical Physiology (respiratory center control, Cheyne-Stokes mechanism, hypoxia classification)
- Ganong's Review of Medical Physiology (4-type hypoxia classification)
- Bradley and Daroff's Neurology in Clinical Practice (neurological localization of breathing patterns)
- Medical Physiology (Boron and Boulpaep) (Biot's breathing, breathing pattern diagram)
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma (hypoxia types, neuropathological correlates)
This is a shared conversation. Sign in to Orris to start your own chat.