Give me a comprehensive guide on Intestinal Obstruction
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
intestinal obstruction causes mechanical ileus diagram
I now have comprehensive content from multiple authoritative sources. Let me compile the full guide:
Intestinal Obstruction — Comprehensive Guide
1. Definition & Classification
Intestinal obstruction is the impairment of normal aboral progression of intestinal contents. It may affect the small bowel (most common) or large bowel, and is classified along two axes:
By Mechanism
| Type | Description |
|---|---|
| Mechanical obstruction | A physical barrier — intrinsic, extrinsic, or intraluminal — blocks the lumen |
| Functional (Paralytic) Ileus | No mechanical block; intestinal motility fails due to neurogenic, metabolic, or pharmacologic causes |
By Completeness
- Complete obstruction — total luminal occlusion; constipation/obstipation; more urgent
- Partial obstruction — some passage of gas/stool; may wax and wane; less immediately life-threatening
By Vascular Compromise
- Simple obstruction — blood supply intact
- Strangulated obstruction — blood supply compromised → ischemia, infarction, perforation (surgical emergency)
By Level
- Small bowel obstruction (SBO) — more common; narrow lumen is easily occluded
- Large bowel obstruction (LBO) — less common; usually due to cancer, volvulus, or diverticulitis
2. Epidemiology & Etiology
The small intestine is most often involved because of its relatively narrow lumen. Hernias, intestinal adhesions, intussusception, and volvulus collectively account for ~80% of mechanical obstructions. — Robbins & Kumar Basic Pathology
Causes of Mechanical Small Bowel Obstruction in Adults
Lesions Extrinsic to the Intestinal Wall
- Adhesions (postoperative) — >60% of all cases in the United States; predominance of lower abdominal procedures (gynecologic, appendectomy, colorectal resection) because bowel is more mobile in the pelvis
- Hernias — second leading cause (~10%); includes inguinal, femoral, umbilical, ventral, obturator, lumbar, and internal hernias
- Neoplastic (carcinomatosis, extrinsic tumors)
- Intraabdominal abscess
Lesions Intrinsic to the Intestinal Wall
- Congenital: malrotation, duplications
- Inflammatory: Crohn disease, tuberculosis, actinomycosis, diverticulitis
- Neoplastic: primary or metastatic tumors (~5% of SBO)
- Traumatic: hematoma
- Miscellaneous: intussusception, endometriosis, radiation stricture
Intraluminal (Obturator) Obstruction
- Gallstone ileus, bezoar, foreign body, enterolith
Malignant tumors causing SBO are mostly metastatic peritoneal implants from ovarian, pancreatic, gastric, or colon primaries; less often hematogenous spread from breast, lung, or melanoma. — Sabiston Textbook of Surgery
Common Causes of Large Bowel Obstruction
- Colorectal cancer (~60%)
- Sigmoid or cecal volvulus
- Diverticulitis with stricture
- Hirschsprung disease (neonates/children)
3. Pathophysiology
Early Phase
- Peristalsis increases proximal to the obstruction → colicky pain
- Gas and fluid accumulate proximal to the obstruction
- Intraluminal pressure rises
Progressive Phase
- Bowel distension stimulates secretion and reduces absorption
- Fluid sequestration into the bowel lumen → dehydration, electrolyte disturbances (hyponatremia, hypokalemia, metabolic alkalosis in proximal SBO; metabolic acidosis in distal)
- Bacterial overgrowth proximal to obstruction
Strangulation
- Rising intraluminal pressure exceeds venous pressure → venous congestion → arterial compromise → ischemia → mucosal barrier failure → bacterial translocation → peritonitis, sepsis, perforation
- Cecal dilation >12–14 cm is a surgical emergency due to high rupture risk — Harrison's Principles of Internal Medicine
Closed-Loop Obstruction
- Both the afferent and efferent limbs are obstructed (e.g., sigmoid volvulus, cecal volvulus, herniated loop)
- Particularly dangerous — rapid progression to strangulation with no decompressive escape
4. Clinical Features
Symptoms
| Symptom | Small Bowel | Large Bowel |
|---|---|---|
| Abdominal pain | Colicky, periumbilical, early | Colicky, lower abdominal, later |
| Vomiting | Early, copious, bilious (proximal) or feculent (distal) | Late, may be absent |
| Distension | Moderate (central) | Marked (peripheral/flanks) |
| Constipation/obstipation | Present | Prominent |
- Onset is usually insidious in malignant obstruction; acute in volvulus or strangulated hernia
- High-pitched "tinkling" bowel sounds early; absent sounds in late obstruction or ileus
- Visible peristalsis may be seen in thin patients
Signs of Strangulation (Urgent)
- Fever, tachycardia
- Localized tenderness, guarding, rigidity
- Leukocytosis
- Acidosis
5. Diagnosis
Laboratory Studies
- CBC: leukocytosis (infection/strangulation)
- BMP/electrolytes: hyponatremia, hypokalemia, elevated BUN/creatinine (dehydration)
- Lactate: elevated in mesenteric ischemia/strangulation
- ABG: metabolic alkalosis (proximal SBO with vomiting) or acidosis (ischemia)
Imaging
Plain Abdominal X-ray (Erect + Supine)
- First-line; multiple dilated loops of bowel with air-fluid levels (classic "step-ladder" pattern in SBO)
- "Colon cut-off sign" in LBO
- Absence of rectal gas
- A plain radiograph alone is insufficient but may demonstrate high or low intestinal obstruction and/or perforation — Grainger & Allison's Diagnostic Radiology

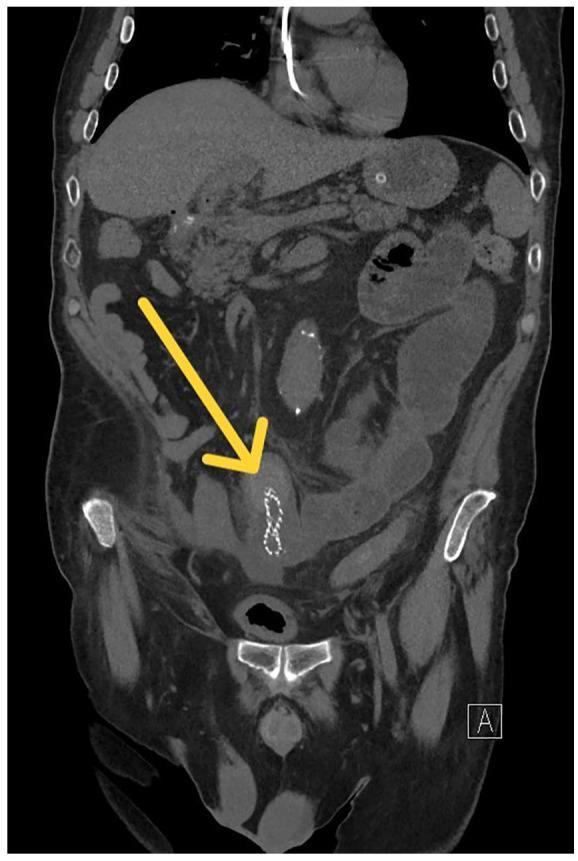
CT Abdomen/Pelvis (with IV contrast) — Gold Standard
- Defines extent, level, and nature of obstruction
- Identifies transition zone (point where bowel changes from dilated to collapsed)
- Distinguishes benign vs. malignant causes:
- Malignant: mass at obstruction site, adenopathy, abrupt irregular transition zone, irregular bowel wall thickening
- Benign: mesenteric vascular changes, large ascites, smooth transition zone, smooth bowel thickening
- Detects strangulation: bowel wall thickening, pneumatosis, portal venous gas, mesenteric edema
- CT enteroclysis for low-grade SBO: water-soluble contrast infused via naso-enteric tube followed by CT — Harrison's Principles of Internal Medicine
Water-Soluble Contrast Study (Gastrografin)
- Therapeutic and diagnostic role in adhesive SBO: if contrast reaches colon within 24 hours, likelihood of non-operative resolution is high
Ultrasound
- Useful in pregnancy; can show dilated loops and absent peristalsis
6. Special Subtypes
Intussusception
Telescoping of a proximal bowel segment into the distal. Most common cause of intestinal obstruction in children <2 years; usually no anatomic defect (often viral/reactive Peyer patch hyperplasia). In adults, usually has a lead point (tumor). Left untreated, progresses to mesenteric compression and infarction. Contrast enema is both diagnostic and therapeutic in infants; surgery required when a lead mass is present. — Robbins & Kumar Basic Pathology
Volvulus
Rotation of bowel around its mesentery. Sigmoid volvulus is most common (elderly, institutionalized, high-fiber diets); cecal volvulus occurs in younger adults. Both are closed-loop obstructions. Sigmoid volvulus may be decompressed endoscopically as a bridge to surgery; recurrence is common without resection.
Gallstone Ileus
A large gallstone erodes through the gallbladder wall into the duodenum (cholecystoenteric fistula), lodges at the terminal ileum (narrowest point). Classic triad on plain X-ray: small bowel obstruction + pneumobilia + ectopic gallstone (Rigler's triad).
Hirschsprung Disease (Congenital Aganglionic Megacolon)
- Incidence ~1:5,000 live births; more common in males
- Congenital absence of ganglion cells in the myenteric and submucosal plexuses of a distal colonic segment
- Presents in neonates with failure to pass meconium → obstructive constipation
- Risks: enterocolitis, perforation, peritonitis
- Treatment: surgical resection of aganglionic segment with anastomosis — Robbins & Kumar Basic Pathology
Paralytic (Adynamic) Ileus
No mechanical obstruction; failure of peristalsis. Diffuse distension of both small and large bowel (vs. mechanical SBO where colon is usually decompressed).
Causes:
- Pharmacologic: opioids (very common post-operative), anticholinergics, haloperidol, tricyclics
- Metabolic: hypokalemia (most common), hyponatremia, hypomagnesemia, uremia, diabetic coma
- Neurogenic: postoperative ileus, spinal cord injury, retroperitoneal irritation
- Infectious: pneumonia, peritonitis, generalized sepsis — Sabiston Textbook of Surgery
Key distinction from mechanical obstruction: diffuse distension without a transition zone; bowel sounds typically absent rather than high-pitched.
7. Management
Initial Resuscitation (All Patients)
- IV access + aggressive fluid resuscitation (isotonic crystalloid)
- Nasogastric (NG) decompression — relieves proximal distension, reduces aspiration risk, provides diagnostic information
- Electrolyte correction — particularly potassium
- Foley catheter — monitor urine output
- NPO — bowel rest
- Analgesia — do not withhold; adequate pain control
- Serial abdominal exams — monitor for deterioration
Non-Operative Management (Adhesive SBO without strangulation)
- Appropriate for partial SBO or complete SBO without signs of strangulation
- NG tube, IV fluids, electrolyte repletion, parenteral nutrition if prolonged
- Water-soluble contrast (Gastrografin) challenge: therapeutic osmotic effect may facilitate resolution; reaching the colon within 24h predicts non-operative success
-
90% of early postoperative SBO is partial and resolves spontaneously — Sabiston Textbook of Surgery
- Trial duration: typically 24–72 hours; re-evaluate if no clinical improvement
Indications for Emergency Surgery
- Complete obstruction with no improvement on conservative management
- Signs of strangulation or peritonitis (fever, tachycardia, peritoneal signs, rising lactate)
- Closed-loop obstruction
- Cecal dilation >12–14 cm
- Perforation or pneumoperitoneum
- Volvulus that cannot be decompressed endoscopically
Surgical Options
| Situation | Procedure |
|---|---|
| Adhesive SBO | Adhesiolysis (laparoscopic or open) |
| Strangulated hernia | Hernia repair ± bowel resection |
| Tumor | Resection ± primary anastomosis |
| Sigmoid volvulus (first episode) | Endoscopic decompression → elective sigmoid resection |
| Malignant LBO | Resection, diverting stoma, or self-expanding metal stent (SEMS) |
| Inoperable malignant obstruction | Venting gastrostomy, medical palliation |
Laparoscopy can diagnose and treat malignant bowel obstruction in selected cases. Self-expanding metal stents placed in the gastric outlet, duodenum, proximal jejunum, colon, or rectum may palliate obstructive symptoms without major surgery. — Harrison's Principles of Internal Medicine
Medical Management of Inoperable Malignant Obstruction
For patients not candidates for surgery, pharmacologic goals are reduction of symptoms, avoiding long-term NG suction, and enabling oral intake for comfort:
- Opioids — abdominal pain
- Antiemetics (dopamine antagonists, phenothiazines, butyrophenones) — nausea/vomiting
- Octreotide — inhibits GI secretion, reduces distension and colicky pain; may relieve obstructive symptoms
- Glucocorticoids — anti-inflammatory; may help resolve obstruction
- Metoclopramide — useful in partial or functional obstruction only; contraindicated in complete mechanical obstruction
- Anticholinergics — reduce secretions and colic
- Venting gastrostomy — decompression tube via PEG; allows oral intake "for pleasure" even as contents drain — Sleisenger & Fordtran's GI and Liver Disease; Harrison's Principles of Internal Medicine
8. Complications
| Complication | Mechanism |
|---|---|
| Dehydration & electrolyte imbalance | Fluid sequestration into obstructed bowel |
| Acute kidney injury | Prerenal from dehydration |
| Bowel ischemia/infarction | Strangulation, vascular compromise |
| Perforation | Pressure necrosis or ischemia |
| Peritonitis | Bacterial translocation or perforation |
| Septic shock | Systemic infection from translocation/perforation |
| Aspiration pneumonia | Vomiting of obstructed contents |
9. Prognosis
- Simple adhesive SBO with early treatment: excellent prognosis
- Strangulated obstruction: mortality rises significantly with delayed surgery
- Malignant obstruction: poor prognosis; median survival is 3–4 months; ~25–30% of patients with cancer and obstruction have a benign cause (adhesions, drug-induced ileus) — Harrison's Principles of Internal Medicine
- Recurrence after adhesiolysis: up to 20–30% over 10 years
10. Key Differentials
| Diagnosis | Distinguishing Features |
|---|---|
| Paralytic ileus | Uniform distension (small + large bowel); no transition zone; precipitant present |
| Pseudo-obstruction (Ogilvie syndrome) | Massive colonic dilation without mechanical block; typically in hospitalized patients |
| Mesenteric ischemia | Severe pain out of proportion to exam; elevated lactate; CT shows bowel wall changes |
| Perforated viscus | Free air on erect CXR; sudden onset; board-like rigidity |
| Intussusception | "Currant jelly" stool in children; lead-point in adults |
Key Takeaways
- Adhesions are the #1 cause of SBO; hernias are #2
- The cardinal features are colicky pain, vomiting, distension, and obstipation
- CT with contrast is the gold-standard imaging modality
- Strangulation = surgical emergency; partial adhesive SBO = trial of conservative management
- Gastrografin challenge has both diagnostic and therapeutic utility in adhesive SBO
- Medical palliation (octreotide, antiemetics, venting gastrostomy) is the cornerstone for inoperable malignant obstruction
Sources: Sabiston Textbook of Surgery (9780443124341) | Robbins & Kumar Basic Pathology (9780323790185) | Harrison's Principles of Internal Medicine 22E (9781265977061) | Sleisenger & Fordtran's GI and Liver Disease (9780323609623) | Grainger & Allison's Diagnostic Radiology (9780323760751)
This is a shared conversation. Sign in to Orris to start your own chat.