Give me a comprehensive guide on Hernias
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed. Here is the comprehensive guide.
Hernias: A Comprehensive Clinical Guide
1. Definition
A hernia is the protrusion of an organ, tissue, or structure through the wall of the cavity in which it normally resides. The essential components are: a defect (weakness in the abdominal wall or a natural opening), a sac (peritoneal lining), and contents (omentum, bowel, or other viscera).
2. Classification
By Reducibility
| Term | Meaning |
|---|---|
| Reducible | Contents can be manually or spontaneously returned to the abdominal cavity |
| Incarcerated | Contents are trapped and irreducible, but blood supply is intact |
| Strangulated | Ischemia or obstruction results from compression of bowel within the hernia neck — surgical emergency |
| Obstructed | Bowel lumen is obstructed within the hernia, with or without strangulation |
"Incarceration alone does not imply a surgical emergency. A wide-necked hernia may contain several non-reducible loops of bowel with no compromise of luminal diameter or blood supply and no symptoms other than a bulge. Strangulation occurs when any degree of ischemia or obstruction results from compression of a loop of bowel within the neck of a hernia." — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
By Origin
- Congenital: Present from birth (e.g., indirect inguinal hernia due to patent processus vaginalis, congenital diaphragmatic hernia)
- Acquired: Develop over time due to connective tissue weakness, prior surgery, or increased intra-abdominal pressure
By Location
- Groin hernias: Inguinal (direct/indirect), femoral
- Ventral/abdominal wall hernias: Umbilical, epigastric, incisional, Spigelian
- Internal hernias: Paraduodenal, foramen of Winslow, mesenteric, obturator
- Special hernias: Hiatal, parastomal, perineal, sciatic, Richter, Littre
3. Epidemiology & Risk Factors
- Hernias of all types are second only to adhesions as the most frequent cause of bowel obstruction in Western countries.
- Inguinal hernias are the most common type, occurring far more frequently in males (M:F ratio ~10:1 for inguinal).
- Femoral hernias are more common in women and are relatively uncommon in children.
Risk Factors
- Family history: Up to 8× increased risk for inguinal hernia
- Connective tissue disorders: Osteogenesis imperfecta, Marfan syndrome, Ehlers-Danlos syndrome
- Collagen imbalance: Decreased type I:III collagen ratio found in fascial/skin specimens
- Smoking: Elevated serum elastolytic activity and MMP dysregulation ("metastatic emphysema")
- Obesity: Increased intra-abdominal pressure
- Prior abdominal surgery: Incisional hernia occurs in ~1 in 5 patients post-laparotomy, more if wound infection occurred
- MMPs (matrix metalloproteinases): MMP overexpression disrupts extracellular matrix integrity in abdominal wall
"A decreased ratio of type I to type III collagens can be detected in fascial and skin specimens obtained from patients with hernias." — Mulholland and Greenfield's Surgery
4. Types of Hernia: Anatomy & Clinical Features
4.1 Indirect Inguinal Hernia
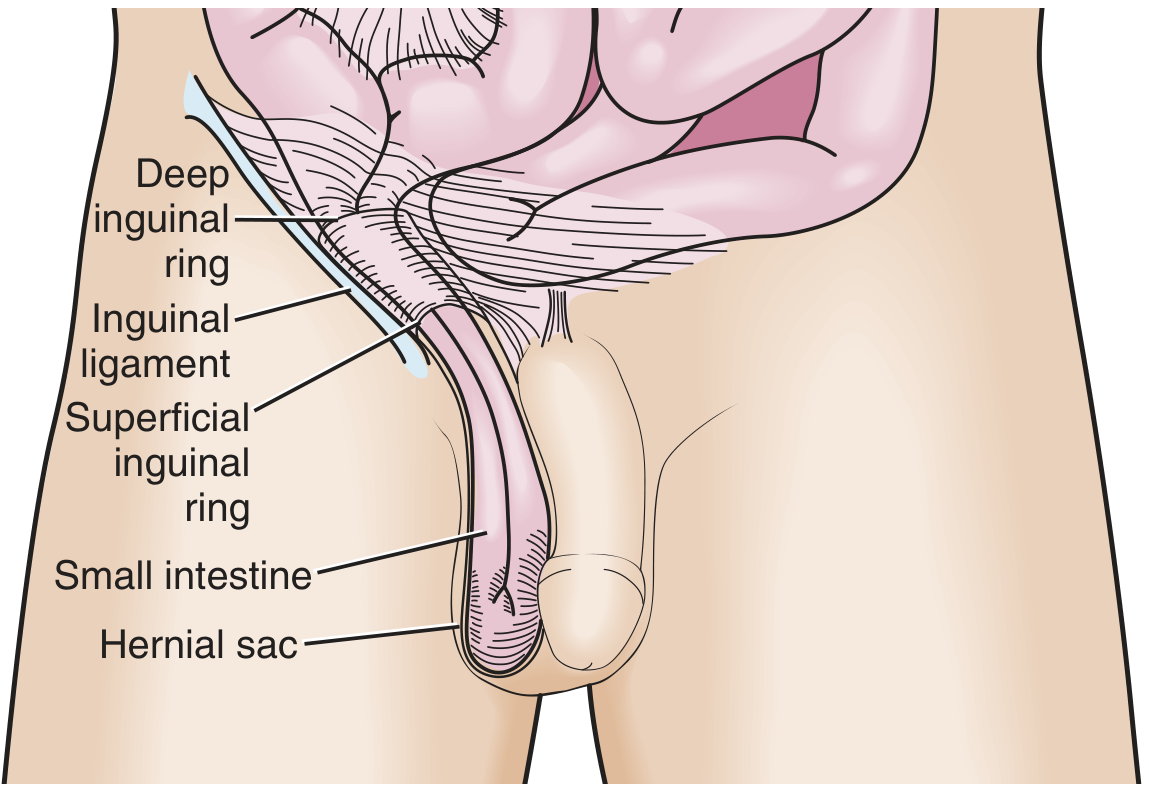
- Pathology: Protrudes through the deep (internal) inguinal ring, lateral to the inferior epigastric vessels, traveling down the inguinal canal — may descend into the scrotum.
- Origin: Failure of closure of the processus vaginalis; therefore, all congenital inguinal hernias in children are indirect.
- Demographics: Most common hernia overall; more common on the right side (later testicular descent); predominates in males.
- In children: High incarceration risk due to narrow inguinal ring. The operation is called herniotomy (high ligation of the sac without floor reconstruction).
4.2 Direct Inguinal Hernia
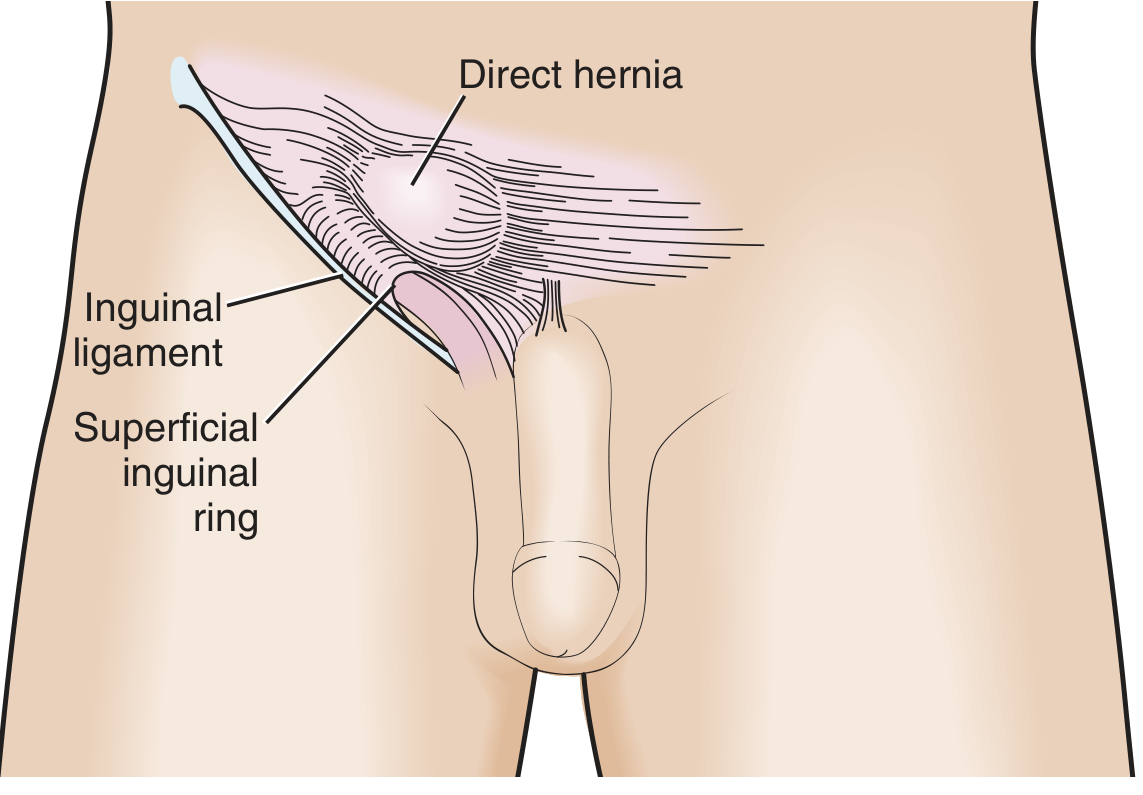
- Pathology: Protrudes medial to the inferior epigastric vessels through a weakness in the posterior inguinal wall (Hesselbach's triangle — bounded by inguinal ligament inferiorly, inferior epigastric vessels laterally, lateral edge of rectus abdominis medially).
- Origin: Acquired, not congenital — results from weakness/attenuation of the transversalis fascia.
- Lower incarceration risk than indirect hernias due to wider neck.
4.3 Pantaloon Hernia
- A combination of both direct and indirect components straddling the inferior epigastric vessels.
- Difficult to diagnose in the ED and to achieve sustained manual reduction; often discovered during surgical exploration.
4.4 Femoral Hernia
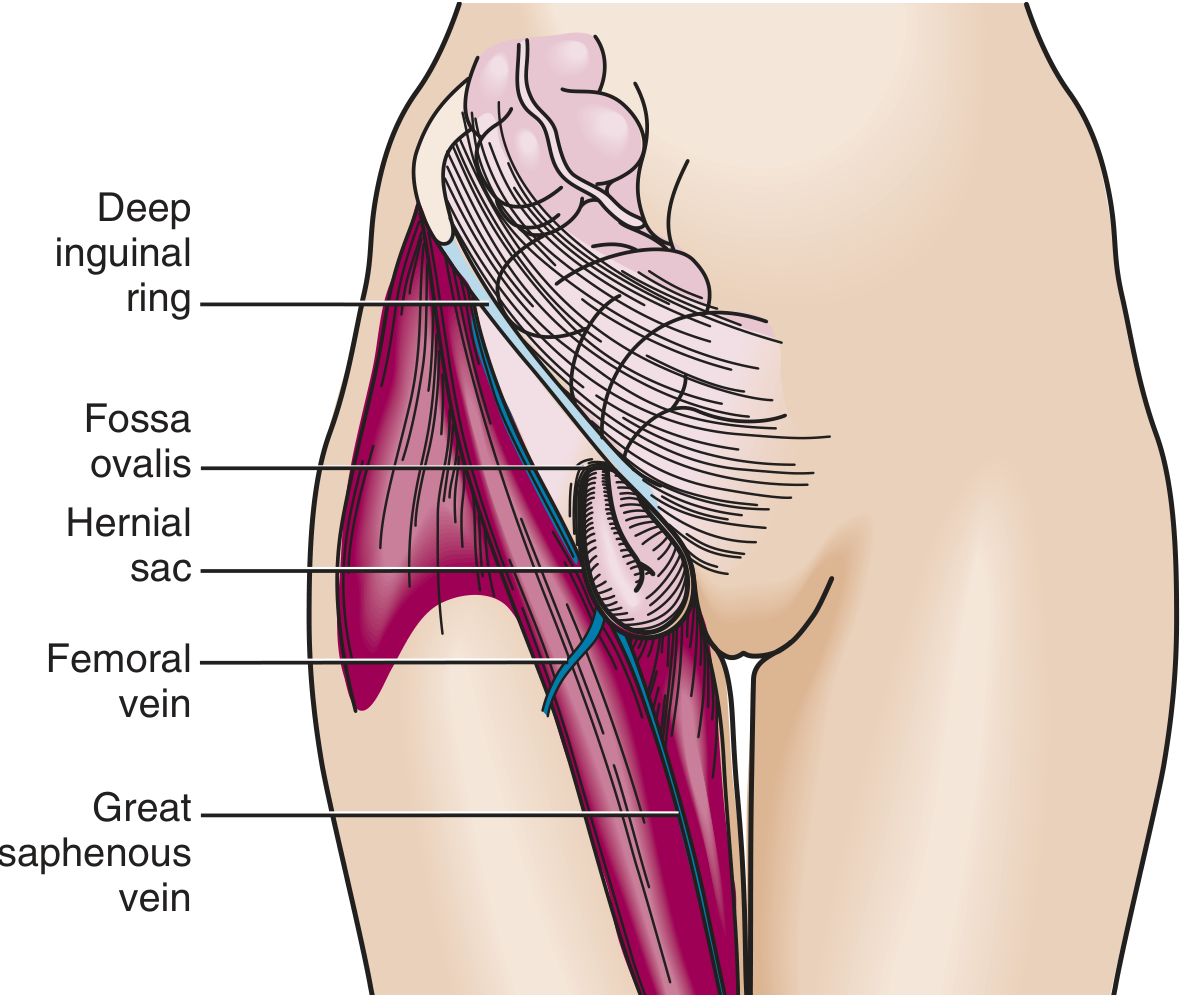
- Anatomy: Protrudes inferior to the inguinal ligament through a defect in the transversalis fascia, into the femoral canal (medial to femoral vein, lateral to lacunar ligament). Presents as a medial thigh mass, below and lateral to the pubic tubercle.
- Demographics: More common in women; uncommon in children.
- Key clinical point: Small fascial defect → incarceration in up to 45% of cases; strangulation at presentation in up to 40%.
- McVay repair specifically addresses femoral hernia by approximating transversus abdominis/transversalis fascia to Cooper's ligament.
4.5 Umbilical Hernia
- Traverses the fibromuscular umbilical ring.
- Occurs in infants (usually closes spontaneously by age 3–4) and adults.
- Adult umbilical hernias are acquired and carry significant strangulation risk — account for ~15% of emergency hernia surgery, with up to 60% showing strangulation at the time of surgery.
- Associated with obesity, pregnancy, ascites, chronic cough.
4.6 Epigastric Hernia
- Protrudes through a defect in the linea alba above the umbilicus.
- Usually small and may contain only preperitoneal fat.
- Often presents as a small painful midline mass.
4.7 Incisional Hernia
- Develops through a prior surgical wound — occurs in up to 20% of patients after abdominal surgery.
- Poor wound healing (e.g., wound infection) markedly increases risk.
- Recurrence rate after repair: 20–50% without mesh; lower with mesh.
- Larger defects paradoxically have a lower incarceration risk than small, tight-necked hernias.
4.8 Spigelian Hernia
- First described by anatomist Adriaan van der Spiegel — protrudes through the semilunar line, just lateral to the rectus sheath, usually below the arcuate line.
- Usually interparietal (rarely penetrates the external oblique fascia) → difficult to palpate clinically.
- Rare: only ~744 cases in the historical literature.
- Diagnosis often requires CT or ultrasound.
4.9 Parastomal Hernia
- Hernia adjacent to an intestinal stoma; a form of incisional hernia.
- Risk of strangulation is only 2% (vs. much higher for femoral/umbilical) due to wide neck.
- Prophylactic mesh placement at stoma creation reduces incidence from ~52% to ~15% in trials.
4.10 Hiatal Hernia
- Sliding hiatal hernia (Type I): Gastro-oesophageal junction migrates above the diaphragm; most common type; associated with GORD.
- Paraesophageal hernia (Type II–IV): Gastric fundus or other viscera herniate beside the oesophagus with GEJ remaining in normal position; risk of volvulus and strangulation — generally repaired electively.
4.11 Obturator Hernia
- Protrudes through the obturator canal.
- Rare; occurs predominantly in elderly, thin women.
- Classic sign: Howship-Romberg sign — medial thigh/knee pain due to obturator nerve compression.
- High risk of strangulation; often diagnosed at laparotomy for SBO.
4.12 Sciatic Hernia
- Protrusion through the greater or lesser sciatic foramen — the rarest of abdominal wall hernias.
- Presents as a buttock swelling; sciatic nerve may be involved.
- Can cause ureteral obstruction if ureter is included.
- Treatment is surgical (transperitoneal and/or transgluteal approach + mesh).
4.13 Richter Hernia
- Only a portion of the bowel wall (not the full circumference) is incarcerated in the hernia neck.
- Ischemia and strangulation can occur without complete bowel obstruction — a diagnostic trap.
- Complete obstruction only if >50% of bowel circumference is incarcerated.
- Most frequently associated with femoral or inguinal hernias.
4.14 Littre Hernia
- Hernia containing a Meckel's diverticulum as the hernial content.
4.15 Internal Hernias
- Herniation through a natural or iatrogenic defect within the peritoneal cavity (paraduodenal, foramen of Winslow, mesenteric).
- Most common type today is iatrogenic following Roux-en-Y gastric bypass, colectomy, or Whipple procedure.
- Often only diagnosed at laparotomy or laparoscopy for presumed adhesive SBO.
5. Pathophysiology
Abdominal Wall Weakness
The transversalis fascia and musculo-aponeurotic layers of the abdominal wall provide structural integrity. Disruption from any cause — congenital (patent processus vaginalis), acquired (connective tissue degradation, surgery), or mechanical (raised intra-abdominal pressure) — creates a defect through which peritoneal contents can herniate.
Collagen Dysregulation
- Decreased type I:III collagen ratio (type I = tensile strength; type III = weaker remodeling matrix)
- MMP overexpression (specifically MMP-1, MMP-2, others): degrades extracellular matrix
- Smoking increases circulating elastolytic activity and MMP levels
- TGF-β1 overexpression, decreased tropoelastin and lysyl oxidase-like 1 synthesis also implicated
- Drug classes under investigation for MMP suppression: tetracyclines (doxycycline), aspirin, statins, thiazolidinediones
Strangulation
Once incarcerated, the hernia neck compresses mesenteric vessels → venous congestion → arterial compromise → ischemia → necrosis → perforation. The narrower the neck (e.g., femoral, umbilical in adults), the faster this cascade.
6. Clinical Presentation
| Feature | Details |
|---|---|
| Classic symptom | Groin or abdominal bulge, worse on standing/straining/coughing |
| Pain | Dull aching; sharp if incarcerated |
| Reducibility | Disappears on lying flat (reducible) or persists (incarcerated) |
| SBO symptoms | Colicky pain, vomiting, abdominal distension, obstipation |
| Strangulation | Severe constant pain, tender erythematous/discoloured mass, systemic toxicity, fever |
Examination pitfall: Incarcerated inguinal hernia can present primarily with bowel obstruction; hernia may only be found on careful groin examination (obese patients especially).
7. Diagnosis
- Clinical examination is usually sufficient for groin and ventral hernias.
- Ultrasound: First-line imaging in equivocal cases; dynamic cough test.
- CT scan: Required for obese patients, suspected internal hernia, or when SBO etiology is unclear. Shows hernia orifice, herniated contents, and signs of ischemia.
- Differentiating incarcerated hernia from hydrocele: You can get fingers above a hydrocele; you cannot get above a hernia (it communicates with the abdominal cavity). Hydroceles transilluminate; hernias do not.
8. Complications
Incarceration
- Irreducible hernia; not necessarily an emergency if no vascular compromise.
- Differentiate from chronically incarcerated hernias (adhesions to sac, no tension).
- Acutely incarcerated: attempt manual reduction (taxis) unless strangulation suspected.
Strangulation
- Ischemic compromise of hernial contents.
- Absolute contraindication to manual reduction: signs of strangulation (severe tenderness, skin erythema, systemic sepsis, suspected bowel necrosis).
- Among SBO patients undergoing surgery, incarcerated hernia is associated with intestinal ischemia in up to 75% and necrosis in >25%.
Richter hernia risk
- Can strangulate and become gangrenous without producing classic SBO signs — must always be considered.
"Reduction en masse"
- The hernia together with its sac and constricting ring is reduced as a unit — persistent obstruction continues despite apparent reduction. Requires operative correction.
9. Management
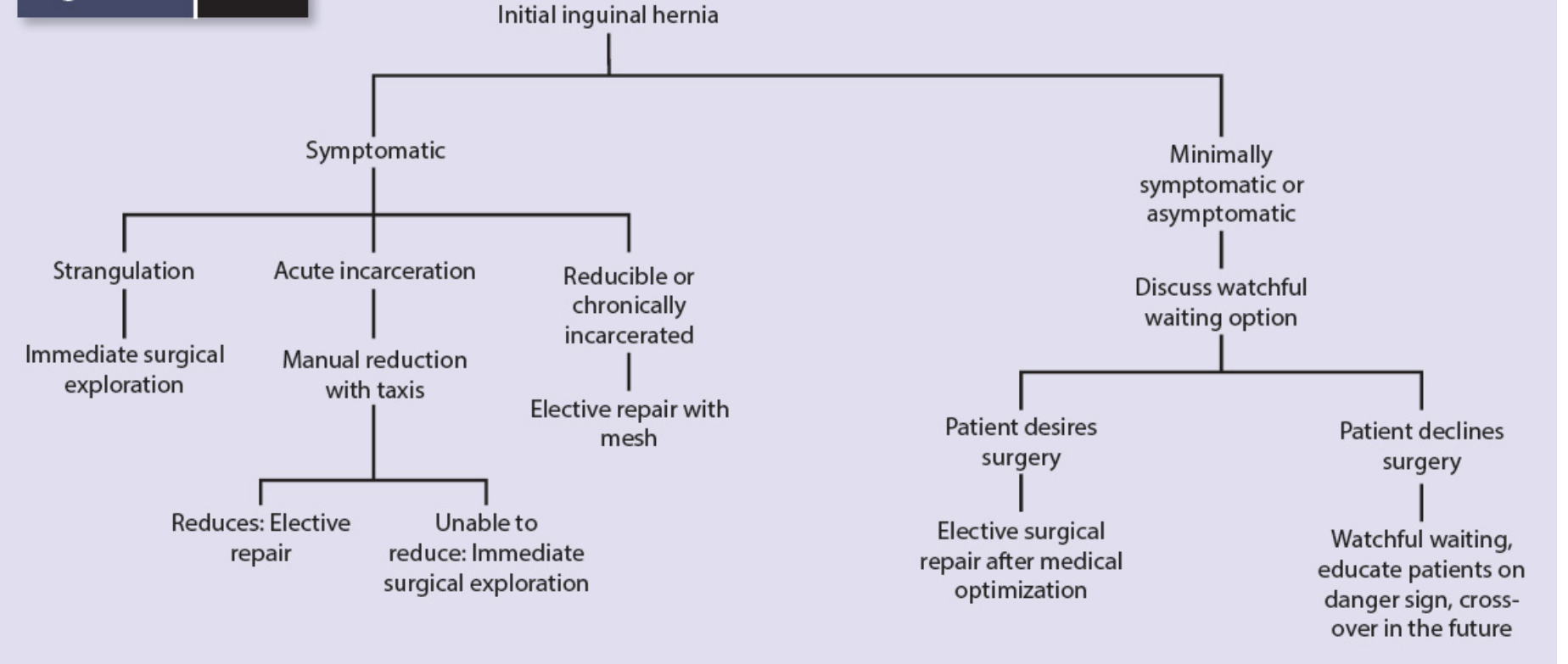
9.1 Watchful Waiting
Randomized controlled trials have shown that watchful waiting is safe for men with asymptomatic or minimally symptomatic inguinal hernias:
- The risk of acute hernia accident (strangulation) is approximately 0.3–0.5%/year.
- However, most patients eventually develop symptoms and cross over to surgery.
- Watchful waiting is not appropriate for femoral hernias (high strangulation risk) or symptomatic hernias.
Management Algorithm for Initial Inguinal Hernia:
9.2 Emergency Management of Incarceration / Strangulation
- IV resuscitation, antibiotics, NPO, urinary catheter
- Taxis (manual reduction): patient sedated, Trendelenburg position; grasp neck of hernia with one hand to elongate it, apply intermittent pressure distally with the other. Avoid excessive force. 1–2 attempts only.
- If taxis fails, or if strangulation is suspected → immediate surgical exploration
- At surgery: reduce hernia, assess bowel viability, resect if nonviable, then repair hernia defect
- Contraindication to taxis: signs of strangulation, gangrenous bowel suspected (skin changes, severe tenderness, systemic sepsis)
9.3 Elective Surgical Repair
Principles of Open Repair
The essential steps (Bassini's principles) for open inguinal hernia repair:
- Complete division of the external oblique aponeurosis and transversalis fascia
- Differentiation between indirect and direct defects
- Isolation of the spermatic cord or round ligament
- High ligation of the hernia sac at the deep inguinal ring
- Reconstruction of the inguinal canal
Tissue Repairs (No Mesh)
- Bassini repair: Transversus abdominis aponeurosis + transversalis fascia sutured to shelving edge of inguinal ligament with nonabsorbable sutures.
- Shouldice repair: Transversalis fascia is divided and repaired with four rows of running sutures — best tissue repair outcomes (~1% recurrence at Shouldice Clinic, though hard to replicate elsewhere).
- McVay (Cooper's ligament) repair: Approximates transversus abdominis/transversalis fascia to Cooper's ligament — the only tissue repair that addresses the femoral canal.
- Tissue repairs carry higher recurrence rates (~10–20%) vs. mesh repairs; increasingly reserved for patients wishing to avoid mesh.
Tension-Free Repair (TFR) — Mesh
- Lichtenstein repair (gold standard for open anterior): Polypropylene mesh placed in the inguinal floor without tension — recurrence rates <2% in experienced hands.
- Mesh is the gold standard for ventral and incisional hernia repair due to its tension-free properties; recurrence rates dramatically lower than primary suture repair.
Laparoscopic / Minimally Invasive Repair
- TEP (Total Extraperitoneal Repair): Mesh placed in preperitoneal space without entering the peritoneal cavity.
- TAPP (Transabdominal Preperitoneal Repair): Mesh placed via transperitoneal approach in preperitoneal space.
- Advantages: reduced chronic groin pain, faster return to activity, lower SSI rates, superior visualization for bilateral hernias.
- Recommended for: recurrent hernias after anterior repair, bilateral inguinal hernias, female groin hernias (to exclude femoral component).
- Laparoscopic repair after a failed anterior (open) repair; anterior repair after a failed posterior (laparoscopic) repair.
- Robotic-assisted repair: Emerging platform especially useful for complex ventral/incisional repairs and retromuscular sublay techniques.
Mesh in Emergency Repairs
- In obstruction without ischemia or gangrene: mesh use appears safe.
- When bowel resection has been performed or significant contamination: mesh is generally avoided initially; two-stage approach preferred.
Antibiotic Prophylaxis
- Not recommended in average-risk clean elective hernia repair.
- Used when contamination risk is elevated (emergency, bowel resection, immunosuppressed).
10. Specific Repair Techniques by Hernia Type
| Hernia Type | Preferred Approach |
|---|---|
| Indirect inguinal (adult) | Tension-free Lichtenstein or TEP/TAPP laparoscopic |
| Direct inguinal | Same as above |
| Femoral | McVay (open) or laparoscopic TAPP/TEP; timely repair due to high strangulation risk |
| Umbilical (adult) | Open mesh repair (Mayo repair for small; mesh for large) |
| Incisional / ventral | Open or laparoscopic mesh repair; retromuscular (sublay) position preferred for large defects |
| Spigelian | Laparoscopic or open mesh repair after CT confirmation |
| Parastomal | Sugarbaker technique (intraperitoneal mesh); laparoscopic/robotic preferred |
| Obturator | Open via transperitoneal approach; laparoscopy if no hemodynamic instability |
| Hiatal paraesophageal | Laparoscopic with or without mesh cruroplasty |
| Sciatic | Transperitoneal + transgluteal; prosthetic mesh |
| Interparietal | Dependent on anatomy; mesh often required |
11. Complications of Hernia Repair
Urinary Retention
- Most common predisposing factor: general or regional anesthesia.
- Additional risk factors: overhydration, opioid use, older age, prostatism, prolonged operative time.
- Treatment: intermittent catheterization; alpha-blockers (tamsulosin, prazosin) show benefit.
Recurrence
- Lowest with tension-free mesh repairs (<2% from specialty centers).
- Higher with tissue-only repairs, emergency repairs, and repairs for recurrent hernias.
- Laparoscopic repairs have now achieved equivalent recurrence rates to open mesh repairs.
- Risk factors for recurrence: first-month complications, suture-only repairs, redo surgery.
Chronic Groin Pain
- A significant long-term issue: reported in 10–12% of patients after inguinal hernia repair.
- Occurs with both open and laparoscopic approaches.
- Mechanisms: nerve entrapment (ilioinguinal, iliohypogastric, genitofemoral), mesh fibrosis, neuroma formation.
- Prevention: careful nerve identification and preservation; laparoscopic approaches may reduce incidence.
Surgical Site Infection (SSI)
- Risk <1% for laparoscopic; <5% for open mesh repair in clean cases.
- Higher with contamination, obesity, smoking, COPD, diabetes, immunosuppression.
- Intraperitoneal mesh infection typically requires mesh removal; extraperitoneal large-pore monofilament mesh often amenable to salvage.
Mesh-Related Complications
- Mesh infection/periprosthetic infection, exposed mesh, extrusion, enterocutaneous fistula.
- Risk varies significantly by mesh type and anatomic location.
- Large-pore, monofilament polypropylene: lower infection rate, high salvageability.
- Microporous, multifilament, or laminar mesh: requires complete removal if infected.
Seroma
- Common after laparoscopic ventral hernia repair; usually managed expectantly.
- Drains reduce surgical site occurrences (SSOs) but do not reduce SSI rates.
Testicular/Cord Complications
- Orchitis, hydrocele, testicular atrophy — from cord vessel injury during extensive dissection.
- Minimizing spermatic cord trauma reduces orchialgia.
Ileus
- More common with laparoscopic procedures than conventional open repair; self-limiting.
12. Special Populations
Pediatric Inguinal Hernia
- All are indirect (patent processus vaginalis); repair is herniotomy (sac ligation only — no floor reconstruction).
- Spontaneous resolution does not occur; all diagnosed hernias are repaired.
- Premature infants have the highest risk of incarceration.
- Incarcerated hernias in infants: attempt manual reduction (with or without light sedation); herniotomy within 24 hours to prevent recurrence.
Women
- Higher proportion of femoral hernias in women — laparoendoscopic technique is recommended (better visualization of femoral ring).
- Timely repair is emphasized given the high strangulation risk of femoral hernias.
Post-Bariatric Surgery
- Internal hernias through mesenteric defects (Peterson's space, transverse mesocolon window, jejunojejunostomy mesentery) are a major cause of SBO post-RYGB.
- Presentation differs from typical SBO and surgery is required >50% of the time.
- Laparoscopic exploration is first-line when hemodynamically stable.
13. Summary Table: Key Hernia Comparisons
| Hernia | Location | Sex predilection | Incarceration risk | Key features |
|---|---|---|---|---|
| Indirect inguinal | Through deep ring → inguinal canal | M >> F | Moderate (higher in infants) | Most common overall; congenital origin |
| Direct inguinal | Through Hesselbach's triangle | M > F | Low | Acquired; wide neck |
| Femoral | Below inguinal ligament, femoral canal | F > M | Very high (45%) | Often strangulated at presentation |
| Umbilical | Umbilical ring | F > M (adults) | High in adults (60% strangulated at surgery) | Ascites, obesity predispose |
| Incisional | Prior surgical scar | Equal | Low (larger defects = lower risk) | 1 in 5 post-laparotomy |
| Spigelian | Semilunar line, below arcuate line | Equal | Moderate | Interparietal; hard to palpate |
| Richter | Any ring, partial wall only | — | High (strangulate without full SBO) | Diagnostic trap |
| Obturator | Obturator canal | Elderly thin women | High | Howship-Romberg sign |
Sources:
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e — Chapter 72 (Hernia) and Chapter 49 (Obstruction)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease — Chapter 123 (Small Bowel Obstruction)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine — Chapter 44 (Hernia Reduction)
- Schwartz's Principles of Surgery, 11e — Chapter 39 (Pediatric Inguinal Hernia) and Chapter 72
Give me comprehensive guide on intestinal obstruction
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple authoritative sources. Let me compile the full guide.
Intestinal Obstruction: A Comprehensive Clinical Guide
1. Definition & Classification
Intestinal obstruction is any condition that impairs the normal aboral transit of intestinal contents through the gut. It is classified along several axes:
By Mechanism
| Type | Description |
|---|---|
| Mechanical obstruction | A physical barrier obstructs the bowel lumen — the most surgically important type |
| Functional obstruction (Ileus) | No physical barrier; absence of normal peristaltic activity (paralytic ileus) |
| Pseudo-obstruction | Massive bowel dilation without mechanical cause; divided into acute (Ogilvie syndrome) and chronic (CIPO) |
By Completeness
- Complete: No gas or fluid passes beyond the obstruction; higher risk of ischemia
- Partial: Some passage of gas/fluid remains; slower progression, lower ischemia risk
By Vascular Compromise
- Simple: Bowel lumen is obstructed but blood supply is intact
- Strangulated: Both luminal obstruction and vascular compromise — a surgical emergency
- Closed-loop: A segment obstructed at both ends (e.g., volvulus, incarcerated hernia with two obstructed points); rapid escalation to ischemia and perforation
By Location
- Small bowel obstruction (SBO): Most common; adhesions account for ~75% of cases
- Large bowel obstruction (LBO): 4–5 times less common than SBO; most often from colorectal cancer, volvulus, or diverticular stricture
By Anatomical Relationship to the Bowel Wall
- Intraluminal (within the lumen): Bezoars, gallstones, foreign bodies, feces, polypoid neoplasms, meconium
- Intramural (within the wall): Carcinoma, IBD (Crohn/UC), anastomotic stricture, intussusception, ischemic injury, radiation injury, diverticulitis
- Extrinsic (from outside): Adhesions, hernias, carcinomatosis, volvulus, endometriosis, congenital bands, abscess
2. The Four Major Mechanical Causes (Robbins)
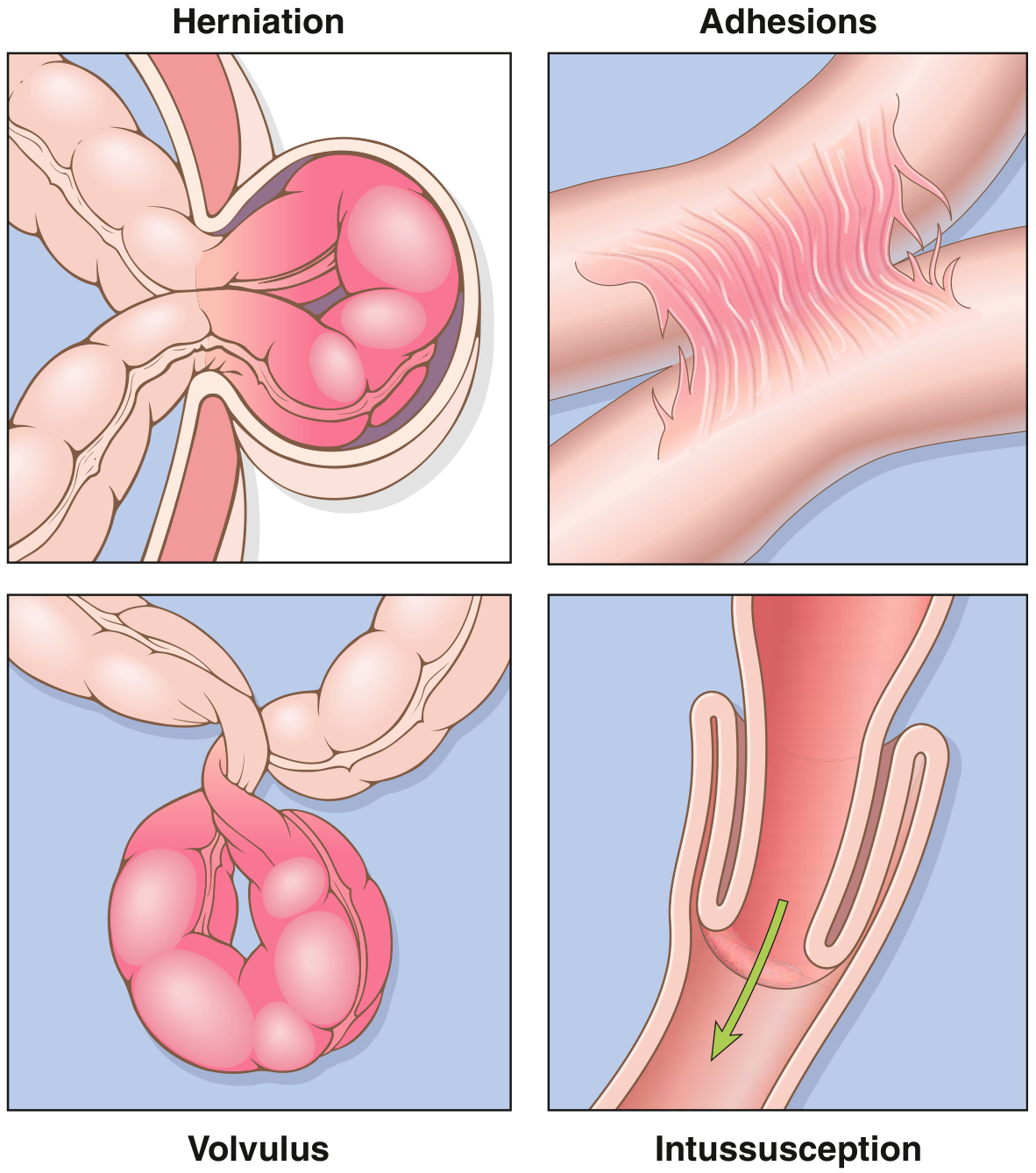
"Collectively, hernias, intestinal adhesions, intussusception, and volvulus account for 80% of mechanical obstructions, while tumors and infarction account for most of the remainder." — Robbins & Kumar Basic Pathology
3. Epidemiology
- SBO accounts for 224,000–344,000 hospital admissions in the USA annually with a stable incidence over the past 25 years.
- Accounts for approximately 2% of all patients presenting to the ED with abdominal pain.
- Adhesiolysis for SBO is the 4th most commonly performed emergency general surgery procedure in the USA.
- Of all admitted SBO patients, approximately 25% require surgery during the index admission.
- Overall mortality for operative SBO management: ~5% in recent series.
- LBO is 4–5 times less common than SBO and affects an older population.
4. Etiology by Type
Small Bowel Obstruction — Common Causes
| Cause | Approximate Proportion |
|---|---|
| Adhesions (post-surgical) | ~75% of cases |
| Hernias (external and internal) | Second most common |
| Crohn disease | Common in IBD populations |
| Malignancy (extrinsic or metastatic) | 5–10% of SBO |
| Volvulus | Less common in Western countries |
| Intussusception | Most common in children <2 years |
| Gallstone ileus, bezoars, foreign body | Rare |
| Radiation stricture, post-ischemic stricture | Iatrogenic |
| Congenital abnormalities (malrotation, atresia, webs) | Usually pediatric; occasionally adult |
Large Bowel Obstruction — Common Causes
- Colorectal adenocarcinoma: Most common cause in the West; ~30% of colorectal cancers present with obstruction
- Colonic volvulus: 5–10% of LBO in the USA (sigmoid 75%, cecal 22% of volvulus cases)
- Diverticular disease: Fibrotic intramural stricture
- Less common: IBD stricture, anastomotic stricture, ischemic colitis, adhesions, pelvic abscess, incarcerated hernia
"In the Western world, LBO is 4 to 5 times less common than SBO and affects an older population. The most common causes are adenocarcinoma of the colon and rectum, colonic volvulus, and benign stricture from diverticular disease; these 3 conditions accounting for about 90% of cases." — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
5. Pathophysiology
Proximal vs. Distal SBO
- Proximal SBO (duodenum/proximal jejunum): Symptoms of gastric outlet obstruction predominate — intractable vomiting, rapid loss of Na⁺, K⁺, Cl⁻ → metabolic alkalosis with hypokalemia; fluid resuscitation alone is sufficient to prevent early death.
- Distal SBO: Fluid/electrolyte replacement alone is insufficient. Progressive intestinal distention leads to venous congestion, impaired mucosal integrity, bacterial translocation, and ischemic necrosis.
Gas and Fluid Accumulation
- Gas accumulates proximal to the obstruction; most originates from swallowed air (Wangenstein demonstrated this with cervical esophagostomy experiments).
- Fluid accumulates from swallowed liquids + GI secretions; obstruction itself stimulates intestinal epithelial water secretion, worsening the accumulation.
- Progressive luminal pressure → increased intramural pressure → impaired microvascular perfusion → ischemia.
Bacterial Translocation
- Epithelial injury begins within 4–6 hours of obstruction; focal epithelial necrosis within 8–12 hours.
- TNF-α, IFN-γ, superoxide anion disrupt epithelial tight junctions.
- Bacterial overgrowth in the obstructed lumen + impaired mucosal barrier → translocation to mesenteric lymph nodes (E. coli found in mesenteric lymph nodes of ~60% of patients undergoing laparotomy for SBO vs. 4% for other laparotomy).
Ischemia Cascade
- Progressive distention → increased wall tension → decreased venous outflow → capillary arterial flow impairment → ischemia → necrosis → perforation.
- Closed-loop obstruction (e.g., volvulus) accelerates this cascade dramatically, as neither proximal nor distal decompression is possible.
Large Bowel Obstruction — Ileocecal Valve Competence
- Competent ICV (75% of patients): Prevents colonic contents decompressing into small intestine → closed-loop obstruction → faster progression to cecal ischemia/perforation.
- Cecal diameter 10–13 cm: Significant perforation risk. Duration and rapidity of distention are more important than exact diameter alone.
- Per the Law of Laplace: Wall tension = intraluminal pressure × radius. The cecum (thinnest wall, largest radius) is most vulnerable.
- Incompetent ICV: Contents back up through the entire small intestine → massive distention, feculent emesis over weeks.
Acute Colonic Pseudo-Obstruction (Ogilvie Syndrome)
- Imbalance in autonomic innervation: sympathetic stimulation or parasympathetic suppression → functional obstruction without mechanical cause.
- Normal parasympathetic supply: vagus nerve (ascending colon to splenic flexure) + sacral cord S2–4 (distal colon).
- Sympathetic nervous system tonically inhibits colonic motility via α2-adrenergic receptors; excessive sympathetic tone → colonic distention.
6. Clinical Presentation
Small Bowel Obstruction
| Feature | Details |
|---|---|
| Pain | Colicky, periumbilical or diffuse; crampy waves (4–5 min cycles) |
| Vomiting | Prominent, especially in proximal SBO; may become feculent in established distal SBO (indicates bacterial overgrowth) |
| Distension | Most pronounced with distal ileal obstruction; absent with proximal obstruction |
| Obstipation | Passage of flatus/stool beyond 6–12 hours suggests partial, not complete obstruction |
| Bowel sounds | Initially hyperactive with high-pitched rushes; diminish/absent in late stages |
| Lab findings | Hemoconcentration, electrolyte abnormalities, mild leukocytosis |
Features Suggesting Strangulation (Surgical Emergency)
- Abdominal pain disproportionate to abdominal findings — visceral ischemia is characteristically more painful
- Tachycardia, fever
- Localized tenderness (peritoneal signs)
- Marked leukocytosis (WBC >15,000)
- Metabolic acidosis
Large Bowel Obstruction
- Patients seek care on average 5 days after onset (better tolerated than SBO)
- Abdominal pain, distension, constipation; vomiting is a late finding
- Malignancy: insidious onset, melena, anemia, weight loss, fatigue
- Rectal mass: tenesmus, pelvic pain, bright-red bleeding
- Sigmoid volvulus: average symptom duration ~38 hours before presentation; 6th–8th decade; often chronically constipated
- Cecal volvulus: bean-shaped dilation in left upper quadrant on X-ray
Ileus vs. Mechanical Obstruction
| Feature | Ileus | Mechanical SBO |
|---|---|---|
| Bowel sounds | Diminished/absent | Hyperactive (early); absent (late) |
| Pain | Mild, diffuse | Colicky |
| Distension | Diffuse, uniform | Asymmetric, proximal to obstruction |
| Radiograph | Diffuse gas throughout bowel + colon | Dilated proximal bowel, no gas in colon |
| Vomiting | Variable | Prominent |
| History | Recent surgery, sepsis, electrolyte disorder, drugs | Prior surgery, hernia, malignancy |
7. Diagnosis
History
- Prior abdominal surgery → adhesions
- IBD, malignancy, radiation → specific etiologies
- Hernia history; always examine groins, umbilicus, and old surgical scars
Physical Examination
- Expose patient completely from "nipples to knees" — old scars fade and previous hernias may be subtle
- Full hernia survey (inguinal, femoral, umbilical, incisional)
- Abdominal distention, tenderness, peritoneal signs
- Bowel sounds character
Imaging
Plain Abdominal X-Ray (AXR)
- First-line; identifies gas pattern
- SBO: dilated loops of small bowel with air-fluid levels (step-ladder pattern); no gas in colon
- LBO: colonic dilation proximal to obstruction
- Free air under diaphragm: perforation
- Sensitivity for SBO: ~70%; limited for distinguishing complete from partial, and for identifying cause or strangulation
CT Scan (Gold Standard)
- Preferred initial imaging in most clinical settings; sensitivity >90% for SBO.
- Identifies: site and cause of obstruction, closed-loop, strangulation signs, transition zone.
- Can be performed without oral contrast in the acute setting.
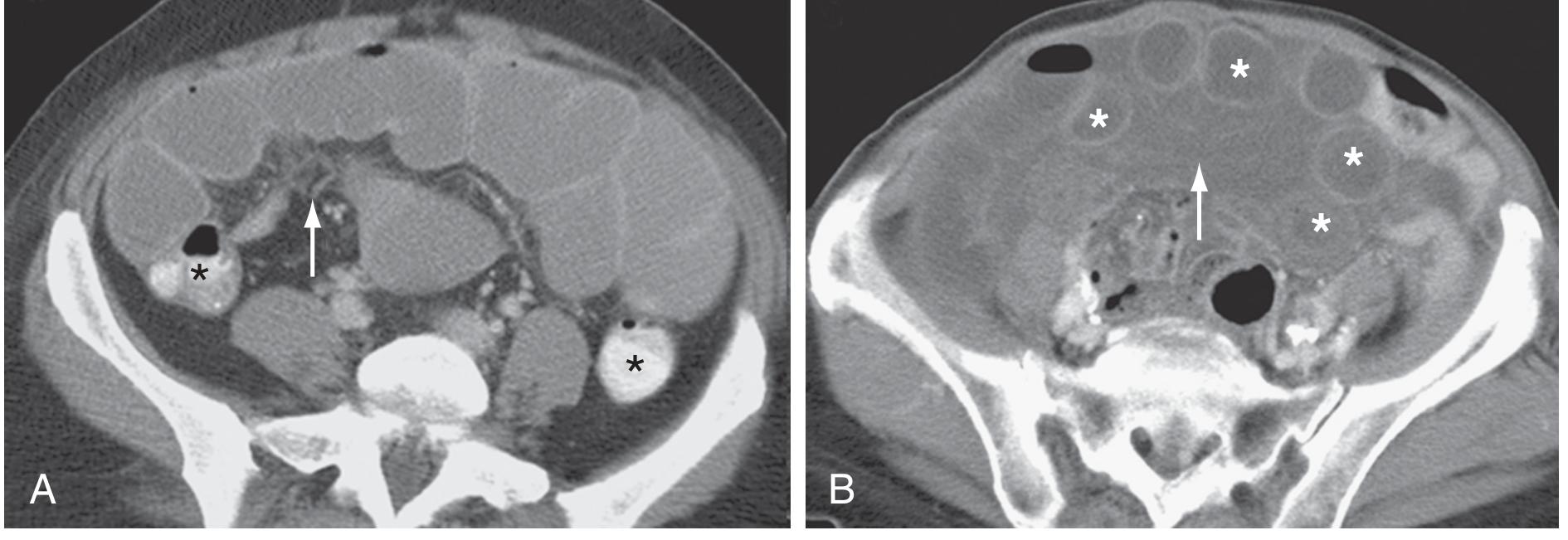
Key CT findings by obstruction type:
| Pattern | CT Findings |
|---|---|
| Simple complete SBO | Dilated proximal bowel; discrete transition zone; collapsed distal bowel; small bowel feces sign |
| Closed-loop | U-shaped fluid-filled loop; whirl sign (tightly twisted mesentery); beak sign (fusiform tapering at obstruction); two adjacent collapsed loops at obstruction |
| Strangulated bowel | Bowel wall thickening with increased attenuation; target/halo sign; pneumatosis intestinalis; poor/absent wall enhancement with IV contrast; mesenteric congestion/hemorrhage; high-density ascites |
CT images: Simple SBO (A) and Closed-loop SBO (B)
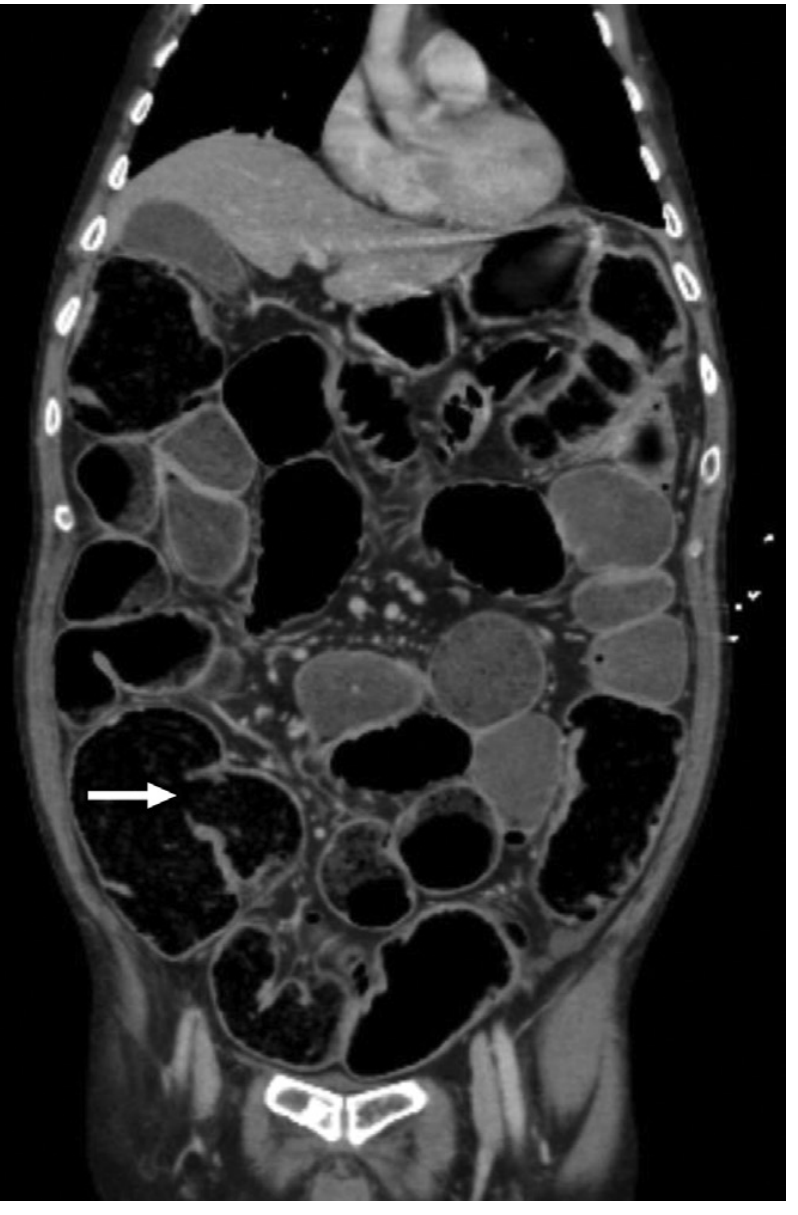
CT coronal image of complete LBO due to sigmoid adenocarcinoma, showing massive small bowel dilation from incompetent ileocecal valve (arrow)
Ultrasound
- Sensitivity >90% for dilated bowel; specificity improves with absent peristalsis.
- Can identify hernias, intussusception, free fluid; cannot reliably determine cause.
- Best as a screening tool; positive result should be followed by CT.
Small Bowel Series / Enteroclysis
- Useful for partial/low-grade SBO where CT sensitivity is <50%.
- Water-soluble contrast (Gastrografin/diatrizoate) preferred over barium if perforation is possible.
- Enteroclysis (contrast instilled via nasoenteric tube into proximal jejunum) provides superior mucosal detail.
Water-Soluble Contrast (Gastrografin) as Diagnostic + Therapeutic Agent
- High-osmolar; draws fluid into bowel lumen, may reduce bowel wall edema and resolve partial SBO.
- Appearance of contrast in colon within 24 hours: sensitivity 92%, specificity 93% for successful nonoperative management.
- Evidence for its therapeutic benefit is mixed; some meta-analyses show reduction in need for surgery and hospital stay, while a major RCT (ABOD Study) showed no benefit vs. saline.
8. Specific Causes: Clinical Features and Management
8.1 Adhesive SBO
The most common cause of SBO overall. Key clinical decisions:
- Is there ischemia? → Immediate surgery
- Will it resolve without surgery? → Trial of nonoperative management
Nonoperative management (NOM):
- NPO, IV fluid resuscitation, NG decompression
- Most patients who resolve do so within 2–3 days
- World Society of Emergency Surgery guidelines: limit NOM to 72 hours from admission
- NOM failure → surgery; earlier decision-making is associated with improved outcomes
- Recurrence is more common and occurs sooner after NOM vs. surgery
Operative management:
- Lysis of adhesions (laparoscopic or open); higher success laparoscopically for single-band adhesions
- Bowel resection if nonviable
- Creating additional adhesions is an inherent risk of surgery → future obstruction risk
8.2 Hernia-Related SBO
- Hernias are the third most common cause of obstruction after adhesions and malignancy (was the most common 100 years ago).
- Unlike adhesive SBO, partial obstruction is rare — most are complete.
- Femoral hernias: up to 45% incarcerated at presentation; frequently missed on exam → must expose groin fully.
- Management: IV resuscitation, antibiotics, urgent surgery
- At surgery: reduce hernia contents, assess bowel viability, resect if nonviable, repair hernia defect
- A CT is warranted to exclude a coincidental but non-causative hernia when another cause of SBO may exist distally
8.3 Volvulus
Sigmoid volvulus (75% of colonic volvulus):
- Common in 6th–8th decade; chronic constipation; redundant sigmoid colon
- Plain X-ray: classic "coffee-bean" or "bent inner tube" sign
- Management: Endoscopic decompression (rigid sigmoidoscopy or flexible colonoscopy) is first-line — success rate 70–85%; followed by elective sigmoid resection to prevent recurrence (~50% risk without surgery)
- Emergency surgery if peritonitis, perforation, or failed endoscopy
Cecal volvulus (22%):
- Congenital lack of cecal fixation; often younger patients
- X-ray: bean-shaped dilation in LUQ; dilated loop of cecum with absent cecal gas in RIF
- Cannot be reduced endoscopically → emergency surgery (right hemicolectomy or cecopexy)
Small bowel volvulus:
- Typically around a mesenteric adhesion band; closed-loop → rapid ischemia
- Emergency laparotomy/laparoscopy; untwist and assess viability
8.4 Intussusception
-
Proximal segment (intussusceptum) telescopes into distal segment (intussuscipiens), dragging mesentery → mesenteric venous compression → ischemia
-
Children <2 years: Most common cause of intestinal obstruction in this age group
- Classic presentation: episodic colicky pain, "currant jelly stools" (blood + mucus from mucosal necrosis), palpable "sausage-shaped" mass in RUQ
- Lead point: usually mesenteric lymphoid hyperplasia (Peyer patches, often post-viral/rotavirus)
- Diagnosis: abdominal ultrasound (target sign); confirmed by contrast enema
- Treatment: Pneumatic or hydrostatic reduction via enema under fluoroscopy — effective and non-surgical
- Surgery: if enema fails, peritonitis, perforation, or a pathological lead point is suspected
-
Adults: Account for only 1% of intestinal obstruction; subacute presentation (days to weeks)
- 80–90% have a pathological process (often malignant) as lead point
- No enema reduction attempts — primary resection without intraoperative reduction is preferred for colonic/ileocolic intussusception to avoid seeding
- Small bowel intussusception in adults: if no pathological lead point on CT, may reduce without resection
8.5 Gallstone Ileus
- A large gallstone (>2.5 cm) erodes through the gallbladder wall into the duodenum (cholecystoduodenal fistula) and impacts at the terminal ileum (narrowest part).
- Classic triad on X-ray (Rigler's triad): small bowel obstruction + ectopic gallstone + pneumobilia (air in bile ducts)
- Treatment: emergency enterolithotomy; cholecystectomy and fistula repair can be staged or simultaneous
8.6 Malignant SBO
- ~5–10% of all SBO; >90% are extraluminal (gynecologic, colorectal, carcinomatosis)
- Poor prognosis: median survival 3–4 months
- Management tailored to performance status, extent of disease, and likely etiology:
- Surgery (lysis, bypass, diverting ostomy, resection): 30-day morbidity 41–44%, mortality 18–22%
- Self-expanding metal stents (SEMS): for gastric outlet, duodenal, proximal jejunal, or colonic obstruction
- Venting gastrostomy: palliation of nausea/vomiting without surgery; allows patients to eat for pleasure
- Medical/pharmacologic: octreotide (reduces GI secretions), corticosteroids (anti-inflammatory, may resolve obstruction), opioids, antiemetics (dopamine antagonists), anticholinergics; metoclopramide only for incomplete/functional obstruction (avoid in complete obstruction)
9. Large Bowel Obstruction — Management
Clinical Assessment
- Mechanical obstruction vs. pseudo-obstruction (Ogilvie syndrome) must be differentiated, as treatments diverge.
- CT is the investigation of choice; can demonstrate the transition point, cause, and signs of ischemia.
Malignant LBO (Colorectal Cancer)
- Most obstructing cancers are distal to the splenic flexure.
- Options:
- Emergency surgery (Hartmann's procedure: resection + end colostomy; or primary resection + anastomosis in selected patients)
- Self-expanding metal stents (SEMS) as a bridge to surgery: decompress the obstruction, allow bowel prep, then elective resection with primary anastomosis — reduced stoma rate
- Palliative stenting in advanced disease
Sigmoid Volvulus — Endoscopic Decompression
- Sigmoidoscopy or colonoscopy with rectal tube placement: first-line when no peritonitis
- 70–85% success rate; recurrence without resection ~50%
- Elective sigmoid colectomy after bowel preparation within same admission
Acute Colonic Pseudo-Obstruction (Ogilvie Syndrome)
- Cecal diameter >10–12 cm = perforation risk; mortality from ischemia/perforation 40–50%
- Conditions associated: non-operative trauma, infection/sepsis, cardiac disease, pelvic/orthopaedic surgery, neurological disease, metabolic disorders
- Conservative management (first-line): bowel rest, correct electrolytes, stop offending drugs (opioids, anticholinergics), ambulate
- Neostigmine: acetylcholinesterase inhibitor; restores parasympathetic tone; highly effective (~80–90%) when conservative therapy fails; give IV with cardiac monitoring (risk of bradycardia); contraindicated in mechanical obstruction
- Colonoscopic decompression: when neostigmine fails or is contraindicated; high success but 30–40% recurrence
- Surgery: cecostomy or right hemicolectomy as last resort or if ischemia/perforation present
10. Treatment Framework
Initial Resuscitation (All Mechanical Obstruction)
- IV fluid resuscitation — isotonic crystalloid; monitor urine output (catheter)
- NPO (nil per os)
- Nasogastric (NG) decompression — removes swallowed air and succus; reduces distention; relieves vomiting
- Electrolyte correction — particularly K⁺, Na⁺, Cl⁻
- Antibiotics — only indicated when strangulation is suspected or confirmed; NOT routinely for simple SBO
- Monitoring: serial abdominal exams; watch for signs of deterioration
Indications for Immediate Surgery
| Finding | Action |
|---|---|
| Clinical strangulation (fever, tachycardia, peritoneal signs, acidosis) | Immediate operative exploration |
| Closed-loop obstruction on CT | Urgent surgery |
| Pneumoperitoneum (perforation) | Emergency laparotomy |
| Incarcerated hernia with suspected strangulation | Emergency surgery |
| Volvulus without response to endoscopy | Emergency surgery |
| Cecal diameter >10–12 cm (ACPO) not responding to neostigmine | Colonoscopy or surgery |
Nonoperative Management — Criteria and Monitoring
- No signs of ischemia
- Partial obstruction (passage of some gas/stool)
- Simple complete SBO without closed-loop features
- Maximum 72 hours per WSES guidelines before reassessment
- Failure rate ~20–30%; these patients require operative intervention
Surgical Options
| Approach | Indication |
|---|---|
| Laparoscopic adhesiolysis | First-episode adhesive SBO; single band; hemodynamically stable |
| Open adhesiolysis/lysis | Extensive adhesions, prior failed laparoscopy, instability |
| Bowel resection + anastomosis | Nonviable bowel; malignancy amenable to resection |
| Diverting ostomy (Hartmann's) | Contaminated field; unprepared colon; high-risk patient |
| Bypass | Unresectable obstruction; palliation |
| Endoscopic stent (SEMS) | Colorectal cancer; gastroduodenal obstruction; palliation |
11. Functional Obstruction — Ileus
Postoperative Ileus (POI)
- Expected after any abdominal or major surgery; NOT a diagnosis requiring workup if within normal time frame.
- Normal resolution: small intestine motility returns within 24 hours, gastric motility by 48 hours, colonic by 2–5 days.
- Bowel sounds are an unreliable indicator of recovery; passage of flatus or stool is the appropriate clinical endpoint.
- Prolonged POI: defined as persistence beyond postoperative day 4 with ≥2 of: nausea/vomiting, inability to tolerate oral diet, absent flatus, distension, radiologic confirmation; occurs in 10–15% of intestinal surgery patients.
Causes of Ileus
- Surgical stress-induced sympathetic reflexes
- Inflammatory mediators (post-surgical or septic)
- Opioid analgesics (mu-receptor mediated)
- Electrolyte abnormalities (hypokalemia, hypomagnesemia)
- Intra-abdominal sepsis/abscess
- Metabolic derangements (hypothyroidism, diabetes)
- Medications: anticholinergics, tricyclics, phenothiazines, calcium channel blockers
Strategies to Reduce/Treat POI
Intraoperative:
- Minimize handling of bowel
- Use laparoscopic approach when possible
- Restrict intraoperative fluid administration
Postoperative:
- Avoid routine nasogastric tubes
- Early enteral feeding
- Thoracic epidural analgesia with local anesthetics (reduces opioid need, enhances splanchnic blood flow, anti-inflammatory)
- Restrict IV fluid administration
- Correct electrolyte abnormalities
- NSAIDs (COX-2 inhibitors) — reduce opioid need, may increase motility
- Alvimopan (mu-opioid receptor antagonist): reduces GI recovery time and hospital stay after major abdominal surgery
- Gum chewing: may shorten ileus duration (simple and inexpensive; limited data)
- 5-HT4 agonists (mosapride, prucalopride): emerging role in resolution of POI
- Avoid NG tube unless vomiting/distention are prominent
12. Chronic Intestinal Pseudo-Obstruction (CIPO)
A long-standing functional disorder of intestinal motility with recurrent episodes of obstruction-like symptoms without a mechanical cause.
Primary Causes
- Familial visceral myopathies (types I, II, III) — degeneration and fibrosis of muscularis propria
- Familial visceral neuropathies (types I, II) — degeneration of myenteric and submucosal plexuses
- Sporadic forms of both
Secondary Causes
| Category | Examples |
|---|---|
| Smooth muscle disorders | Scleroderma (progressive systemic sclerosis), myotonic dystrophy, amyloidosis |
| Neurological disorders | Parkinson disease, Chagas disease, spinal cord injury |
| Endocrine disorders | Diabetes mellitus, hypothyroidism, hypoparathyroidism |
| Infections | CMV, Epstein-Barr virus |
| Medications | Phenothiazines, tricyclics, opioids, anticholinergics |
| Radiation | Radiation enteritis |
Diagnosis
- Clinical features: chronic/recurrent nausea, vomiting, abdominal pain, distention
- Confirmed by radiographic studies (dilated bowel without mechanical obstruction) and manometry
- May require laparoscopy/laparotomy with full-thickness biopsy to establish specific neural/myopathic cause
- Rule out mechanical obstruction with CT/contrast studies
13. Special Populations
Pediatric
- Neonates: Hirschsprung disease (aganglionic megacolon — failure to pass meconium, then obstructive constipation); meconium ileus (cystic fibrosis); intestinal atresia
- Infants <2 years: Intussusception is most common cause of obstruction; treat with enema reduction
- Children: Midgut volvulus from intestinal malrotation is a surgical emergency (risk of entire midgut necrosis)
- All congenital bowel obstructions require pediatric surgical consultation
Post-Bariatric Surgery (RYGB)
- Internal hernias (Peterson's space, transverse mesocolon, jejunojejunal mesentery) are a major cause of SBO.
- Presentation differs from typical SBO; CT findings may be subtle.
- Surgery is required >50% of the time; early reoperation (often <24 hours) is preferred.
- Laparoscopic exploration first-line when hemodynamically stable.
Malignancy (Palliative Setting)
- SBO from carcinomatosis carries a median survival of 3–4 months.
- About 25–30% of patients with known cancer and obstruction have a benign cause (adhesions, ileus from vinca alkaloids or opioids).
- Medical management: octreotide, corticosteroids, opioids, antiemetics.
- Venting gastrostomy for quality of life in inoperable cases.
- SEMS for discrete obstructions at accessible sites.
14. Summary Tables
SBO: Diagnosis Targets
| Goal | Method |
|---|---|
| Mechanical vs. ileus | CT, clinical history, bowel sounds |
| Cause | CT (adhesion vs. hernia vs. mass), history |
| Complete vs. partial | CT (collapsed colon = complete), passage of flatus/stool |
| Simple vs. strangulated | CT (ischemia signs), clinical (fever, tachycardia, peritoneal signs, acidosis) |
CT Signs Summary
| Sign | Meaning |
|---|---|
| Transition zone | Site of obstruction |
| Small bowel feces sign | Particulate matter in obstructed loop (feculization) — chronic/complete obstruction |
| Whirl sign | Twisted mesentery — closed-loop or volvulus |
| Beak sign | Fusiform tapering — point of obstruction |
| Target/halo sign | Concentric bowel wall rings — edema/ischemia |
| Pneumatosis intestinalis | Gas within bowel wall — ischemia/necrosis |
| Portal venous gas | Gas in portal/hepatic veins — severe ischemia/necrosis |
| Coffee-bean sign (plain X-ray) | Sigmoid volvulus |
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease — Chapters 123 & 124
- Schwartz's Principles of Surgery, 11e — Chapter 28
- Mulholland and Greenfield's Surgery, 7e — Chapter 72
- Robbins & Kumar Basic Pathology — Chapter 13
- Harrison's Principles of Internal Medicine, 22e
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.