Clinnical and developmental anatomy of diaphragam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough response. Let me compile it.
Clinical and Developmental Anatomy of the Diaphragm
1. Overview
The diaphragm is a dome-shaped musculotendinous partition that seals the inferior thoracic aperture, separating the thoracic cavity from the abdominal cavity. It is the principal muscle of inspiration, accounting for the majority of tidal ventilation during quiet breathing. It is a composite structure - both architecturally and developmentally - with muscle fibers arising radially from peripheral bony and ligamentous attachments and converging on a central tendon.
- Gray's Anatomy for Students, p. 164
2. Gross Anatomy
2.1 Attachments
The diaphragm is attached peripherally to:
| Region | Attachment |
|---|---|
| Anterior | Xiphoid process of the sternum |
| Anterolateral | Inner surfaces of the lower 6 costal cartilages and ribs |
| Posterolateral | Ends of ribs XI and XII |
| Posterior - crura | Bodies of L1-L3 (right crus) and L1-L2 (left crus), blending with the anterior longitudinal ligament |
| Posterior - ligaments | Median, medial, and lateral arcuate ligaments |
The right crus is longer and broader, attaching down to L3; the left crus reaches only L2. The two crura are connected across the midline by the median arcuate ligament, which arches anterior to the aorta.
The medial arcuate ligament spans across psoas major (from the body of L1 to the transverse process of L1). The lateral arcuate ligament spans across quadratus lumborum (from the transverse process of L1 to rib XII).
- Gray's Anatomy for Students, pp. 198-199, 432
2.2 Central Tendon
All muscle fibers converge on the central tendon, a clover-leaf-shaped aponeurosis located slightly anterior to center. The fibrous pericardium is firmly attached to its middle part, which accounts for the flattening of the diaphragm centrally and the domed appearance of the two lateral leaflets.
2.3 The Domes
The diaphragm is not flat - it balloons superiorly on both sides to form domes:
- Right dome - higher, reaching as far as the level of rib V (pushed up by the liver)
- Left dome - at the level of the 5th intercostal space (pushed up by the stomach and spleen)
- At normal expiration these levels are a useful landmark for percussion
The domes are produced by the underlying abdominal viscera: liver and right kidney on the right; fundus of stomach, spleen, and left kidney on the left.
- Gray's Anatomy for Students, pp. 432
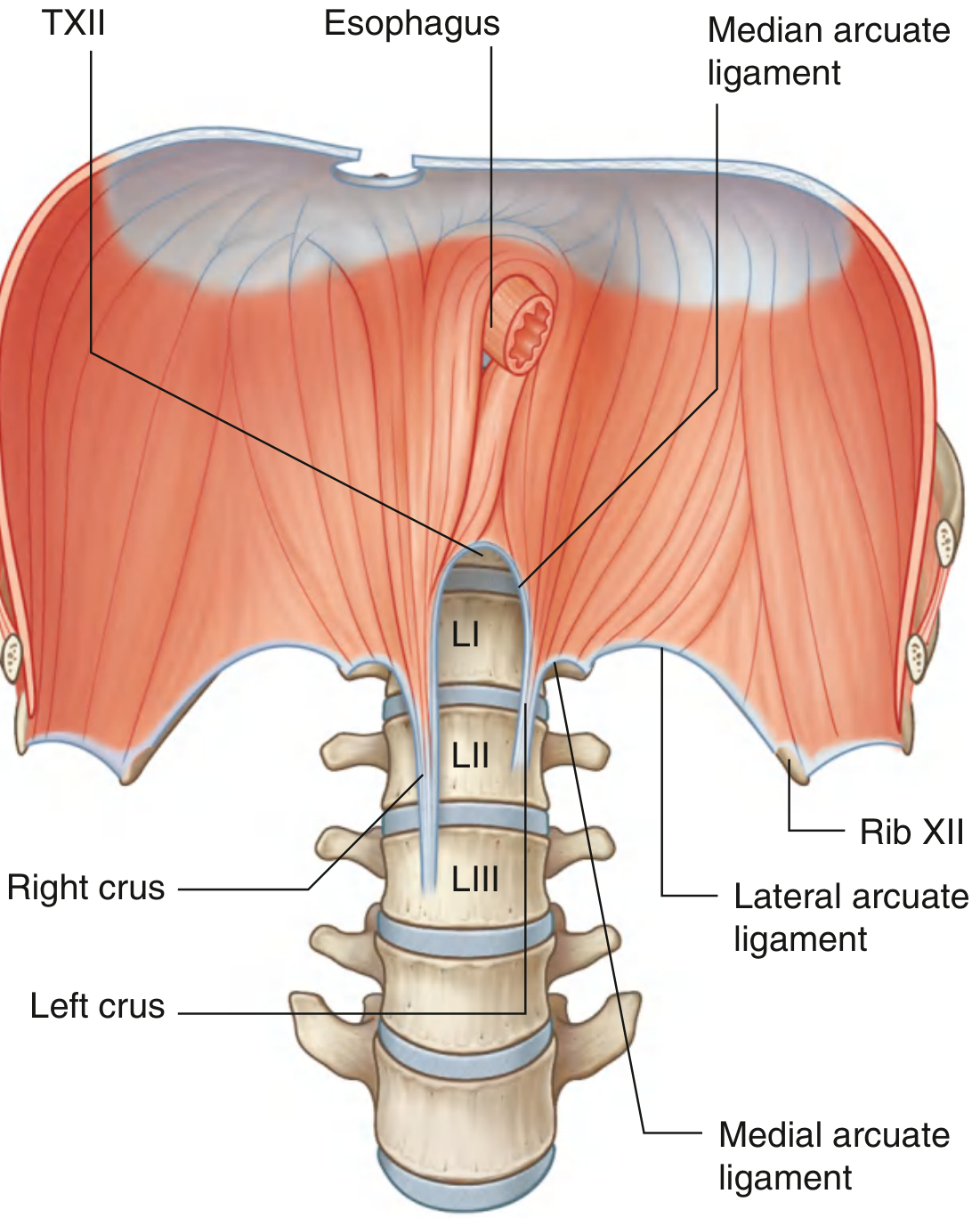
Inferior view of the diaphragm showing the right and left crura, median/medial/lateral arcuate ligaments, and vertebral levels (Gray's Anatomy for Students)
3. Openings in the Diaphragm
Three major openings transmit key structures between the thorax and abdomen:
| Opening | Vertebral Level | Structures Passing Through |
|---|---|---|
| Caval opening (foramen venae cavae) | T8 | Inferior vena cava, right phrenic nerve |
| Esophageal hiatus | T10 | Esophagus, anterior and posterior vagal trunks, esophageal branches of left gastric artery/vein, lymphatics |
| Aortic hiatus | T12 | Aorta, thoracic duct, sometimes azygos/hemiazygos veins |
Memory aid: "I eat at 10" - IVC at T8, Esophagus at T10, Aorta at T12.
Additional structures passing through or around the diaphragm:
-
Left phrenic nerve - passes through the muscular part, anterior to the central tendon on the left
-
Greater, lesser, and least splanchnic nerves - perforate the crura
-
Hemiazygos vein - through the left crus
-
Sympathetic trunks - posterior to the medial arcuate ligament on each side
-
Superior epigastric vessels - pass anterior to the diaphragm just deep to the ribs
-
Gray's Anatomy for Students, pp. 432-433
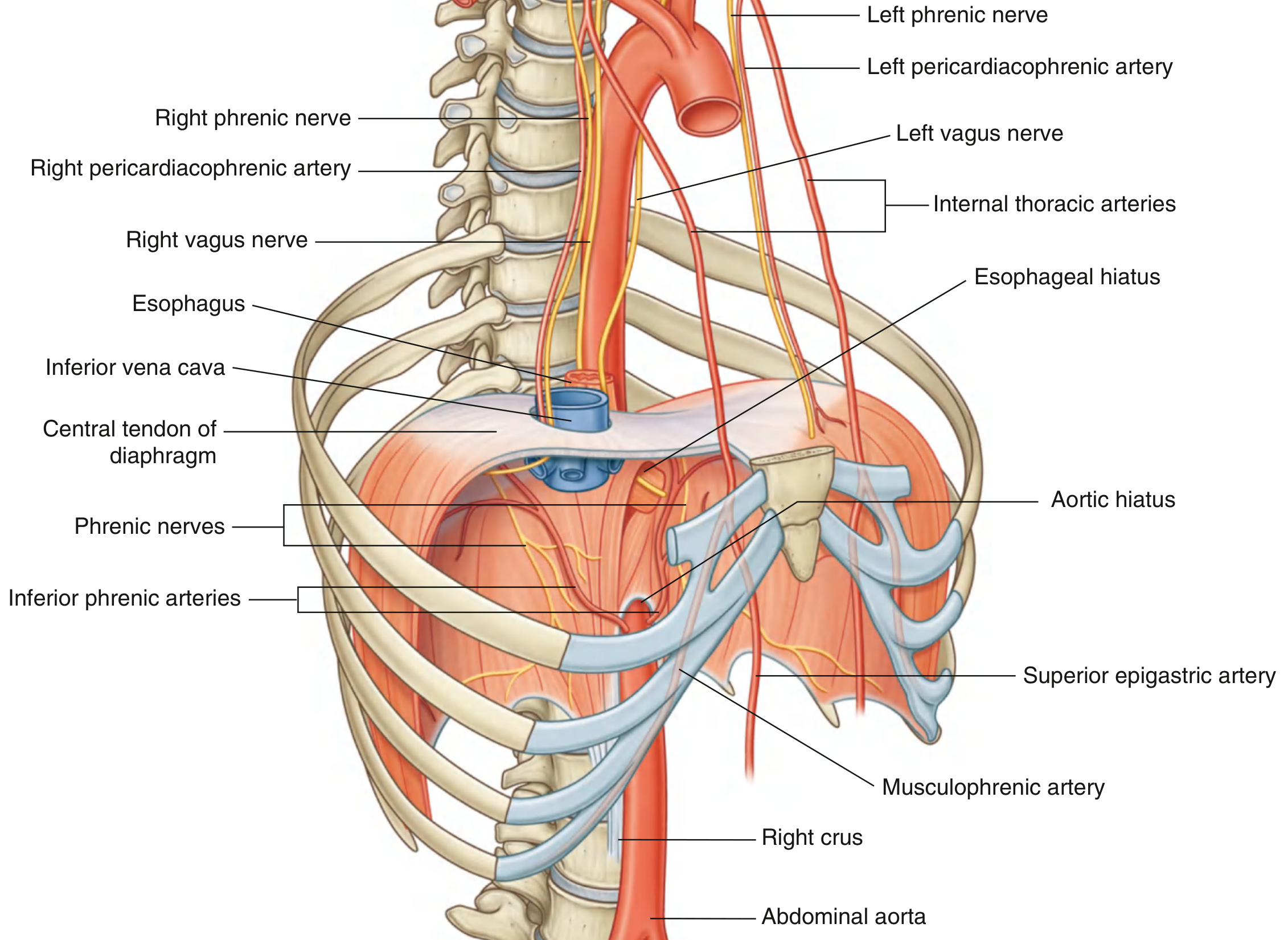
Posterior view of the diaphragm showing vascular supply, phrenic nerves, vagus nerves, and hiatal openings (Gray's Anatomy for Students)
4. Blood Supply
Superior surface (from above):
- Pericardiacophrenic arteries - branches of the internal thoracic artery (accompany the phrenic nerves)
- Musculophrenic arteries - terminal branches of the internal thoracic artery
- Superior phrenic arteries - small branches from the lower thoracic aorta
Inferior surface (from below):
- Inferior phrenic arteries - largest supply; arise directly from the abdominal aorta just below the aortic hiatus
Venous drainage parallels the arteries, draining into the brachiocephalic veins, the azygos system, and abdominal veins (left suprarenal vein, IVC).
- Gray's Anatomy for Students, pp. 198, 433
5. Nerve Supply (Innervation)
The diaphragm receives both motor and sensory innervation from the phrenic nerves (C3, C4, C5 - "C3, 4, 5 keeps the diaphragm alive"). Each phrenic nerve penetrates the diaphragm and innervates it from its abdominal surface.
- The right phrenic nerve passes through the caval opening (T8) and lies on the fibrous pericardium before reaching the diaphragm.
- The left phrenic nerve pierces the muscular part of the diaphragm just anterior to the central tendon on the left.
The peripheral parts of the diaphragm (derived from lateral body wall) also receive sensory supply from the lower intercostal nerves (T5-T12). This is clinically important - central diaphragmatic pain refers to the shoulder (C3-C5 dermatome), while peripheral irritation refers to the thoracic/abdominal wall.
- Gray's Anatomy for Students, pp. 198, 441
6. Function and Movements During Breathing
During inspiration:
- The muscular portion contracts, pulling the central tendon inferiorly
- The domes flatten (descend caudally), enlarging the thoracic cavity vertically
- This reduces intrathoracic pressure, drawing air into the lungs
- The descending diaphragm also pushes the anterior abdominal wall outward
The thorax also expands in anteroposterior ("pump handle") and lateral ("bucket handle") directions through rib cage movements.
During expiration, the diaphragm relaxes and rises passively.
The costodiaphragmatic recess - the lowest part of the pleural cavity between the thoracic wall and diaphragm - is the largest pleural recess and is of clinical importance (site for pleural effusion drainage).
- Goldman-Cecil Medicine, p. 1006
7. Development of the Diaphragm (Embryology)
The diaphragm is a composite structure developing from four embryonic components:
7.1 Septum Transversum
- A mesodermal shelf growing dorsally from the ventrolateral body wall during week 4
- Initially separates the heart from the liver, but does not completely seal the thoracic-abdominal partition
- Forms the central tendon of the adult diaphragm
- Large pericardioperitoneal canals remain on either side of the esophagus at this stage
7.2 Pleuroperitoneal Membranes
- Folds that grow medially from the lateral body walls during weeks 5-7
- Fuse with the dorsal mesentery of the esophagus and the septum transversum
- This fusion completes the partition between the thorax and abdomen, forming the primordial diaphragm
- Although these membranes form large portions of the early fetal diaphragm, they represent relatively small portions of the neonatal diaphragm
7.3 Dorsal Mesentery of the Esophagus
- The septum transversum and pleuroperitoneal membranes fuse with this structure
- Constitutes the median portion of the diaphragm
- The crura of the diaphragm develop from myoblasts that grow into the dorsal mesentery of the esophagus
7.4 Muscular Ingrowth from Lateral Body Walls
- During weeks 9-12, the expanding lungs and pleural cavities burrow into the lateral body walls
- This splits body wall tissue into an external layer (becomes the abdominal wall) and an internal layer (forms the peripheral muscular parts of the diaphragm)
- Further extension forms the costodiaphragmatic recesses, establishing the dome-shaped configuration
Candidate genes on chromosome 15q play a role in regulating this process.
- The Developing Human (Moore & Persaud), pp. 438-441; Langman's Medical Embryology, p. 122
8. Positional Changes and Innervation - Developmental Basis
At week 4, the septum transversum lies opposite the C3-C5 somites. During week 5, myoblasts from these somites migrate into the developing diaphragm, carrying their nerve fibers with them. This is why the phrenic nerves arise from C3, C4, and C5.
As the embryo grows, the dorsal body wall grows faster, causing an apparent caudal descent of the diaphragm:
- Week 6: diaphragm at the thoracic somite level
- Week 8: dorsal diaphragm at the level of L1
The phrenic nerves lengthen accordingly, reaching approximately 30 cm in adults. They pass through the pleuropericardial membranes (explaining why, in the adult, the phrenic nerves lie on the fibrous pericardium - the adult derivative of those membranes).
The peripheral costal portions retain sensory innervation from the lower intercostal nerves due to their origin from the lateral body wall.
- The Developing Human, pp. 440-441
9. Congenital Anomalies (Clinical Anatomy)
9.1 Congenital Diaphragmatic Hernia (CDH) - Posterolateral (Bochdalek) Hernia
- Most common developmental defect of the diaphragm: 1 in 2,200 neonates
- Results from failure of the pleuroperitoneal membranes to fuse with the septum transversum and dorsal mesentery
- The primary defect: fibroblasts in the pleuroperitoneal membranes fail to provide scaffolding for migrating myoblasts, resulting in a muscular deficiency
- 85% left-sided (left pleuroperitoneal canal closes later than the right)
- Abdominal contents (stomach, intestine, liver, spleen) herniate into the thorax
- Herniated viscera compress the developing lung, causing pulmonary hypoplasia (fewer airway branches, abnormal pulmonary vessels)
- Presents at birth with respiratory distress, scaphoid abdomen, mediastinal shift
- Mortality remains high; survivors risk bronchopulmonary dysplasia, persistent pulmonary hypertension, GERD
9.2 Retrosternal (Parasternal/Morgagni) Hernia
- Herniation through the sternocostal hiatus (foramen of Morgagni) - the gap between the sternal and costal parts of the diaphragm (where the superior epigastric vessels pass)
- Typically right-sided
- A small peritoneal sac containing intestinal loops may enter the chest
- Often clinically silent; occasionally detected incidentally on imaging in adults
9.3 Hiatal Hernia
- Herniation of part of the stomach through an enlarged esophageal hiatus (T10)
- Usually acquired in adult life; congenitally enlarged hiatus may be a predisposing factor
- Types: sliding (type I - most common) and paraesophageal (types II-IV)
9.4 Diaphragmatic Eventration
- Half (or part) of the diaphragm has defective musculature and balloons into the thoracic cavity as a thin membranous/aponeurotic sheet
- Results from failure of muscular tissue from the body wall to extend into the pleuroperitoneal membrane
- NOT a true hernia (no defect, no hernial sac) - but clinical presentation can mimic CDH
- Most commonly left-sided; treated by surgical plication
9.5 Accessory Diaphragm
- Rare anomaly (>30 cases reported); most often on the right side
- Associated with lung hypoplasia and respiratory complications
- Diagnosed by MRI/CT; treated by surgical excision
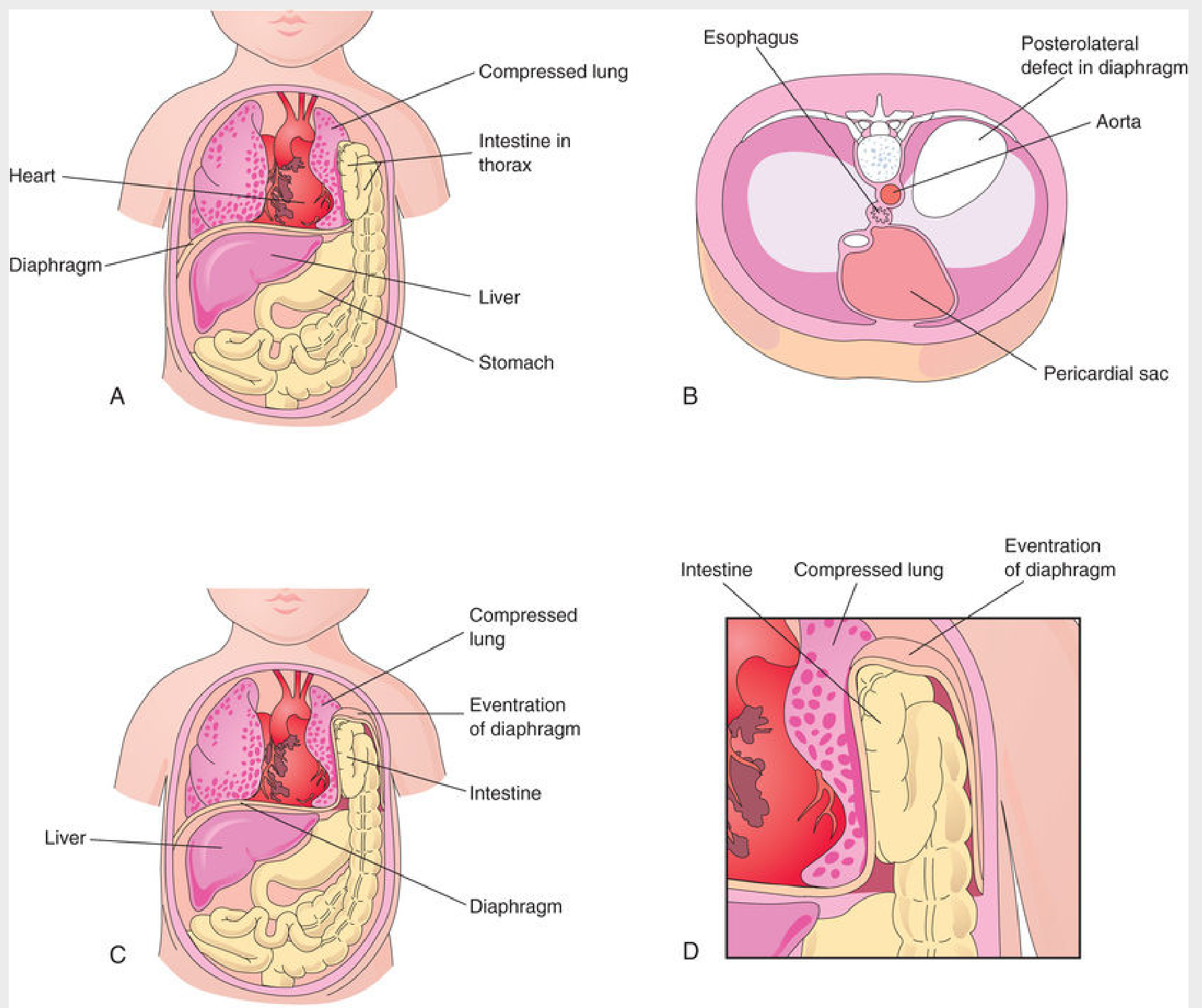
Congenital diaphragmatic hernia (A, B) and diaphragmatic eventration (C, D) - note herniation of intestine through posterolateral defect and compressed hypoplastic lung (The Developing Human)
- The Developing Human, pp. 441-449; Creasy & Resnik's Maternal-Fetal Medicine; Langman's Medical Embryology, p. 122-123
10. Clinical Correlates Summary
| Condition | Mechanism | Key Feature |
|---|---|---|
| Phrenic nerve palsy | Injury/compression of C3-C5 or phrenic nerve (e.g., lung cancer, varicella, trauma, cervical spondylosis) | Elevated hemidiaphragm on CXR; "paradoxical" movement on sniff test |
| Diaphragmatic paralysis | Bilateral phrenic nerve injury | Significant respiratory distress; orthopnea; treated by surgical plication |
| CDH (Bochdalek) | Failed pleuroperitoneal membrane fusion | Left-sided (85%), pulmonary hypoplasia, neonatal respiratory distress |
| Morgagni hernia | Sternocostal hiatus defect | Right-sided, often incidental, contains bowel/omentum |
| Hiatal hernia | Lax esophageal hiatus | GERD, chest pain, regurgitation |
| Eventration | Muscular ingrowth failure | Aponeurotic hemidiaphragm, may simulate CDH |
| Referred pain | Subphrenic inflammation irritates central diaphragm (phrenic) | Shoulder tip pain (C4 dermatome) |
| Ventilator-induced diaphragm dysfunction | Disuse atrophy during mechanical ventilation | Begins after 24-36 hours; affects both fast and slow myofibers |
Sources:
- Gray's Anatomy for Students (9780323934237)
- The Developing Human: Clinically Oriented Embryology (9780323611541)
- Langman's Medical Embryology (9781496383907)
- Goldman-Cecil Medicine (9780323930345)
- Creasy & Resnik's Maternal-Fetal Medicine (9780323828499)
This is a shared conversation. Sign in to Orris to start your own chat.