
tell me about the usg with diagrammatic representation
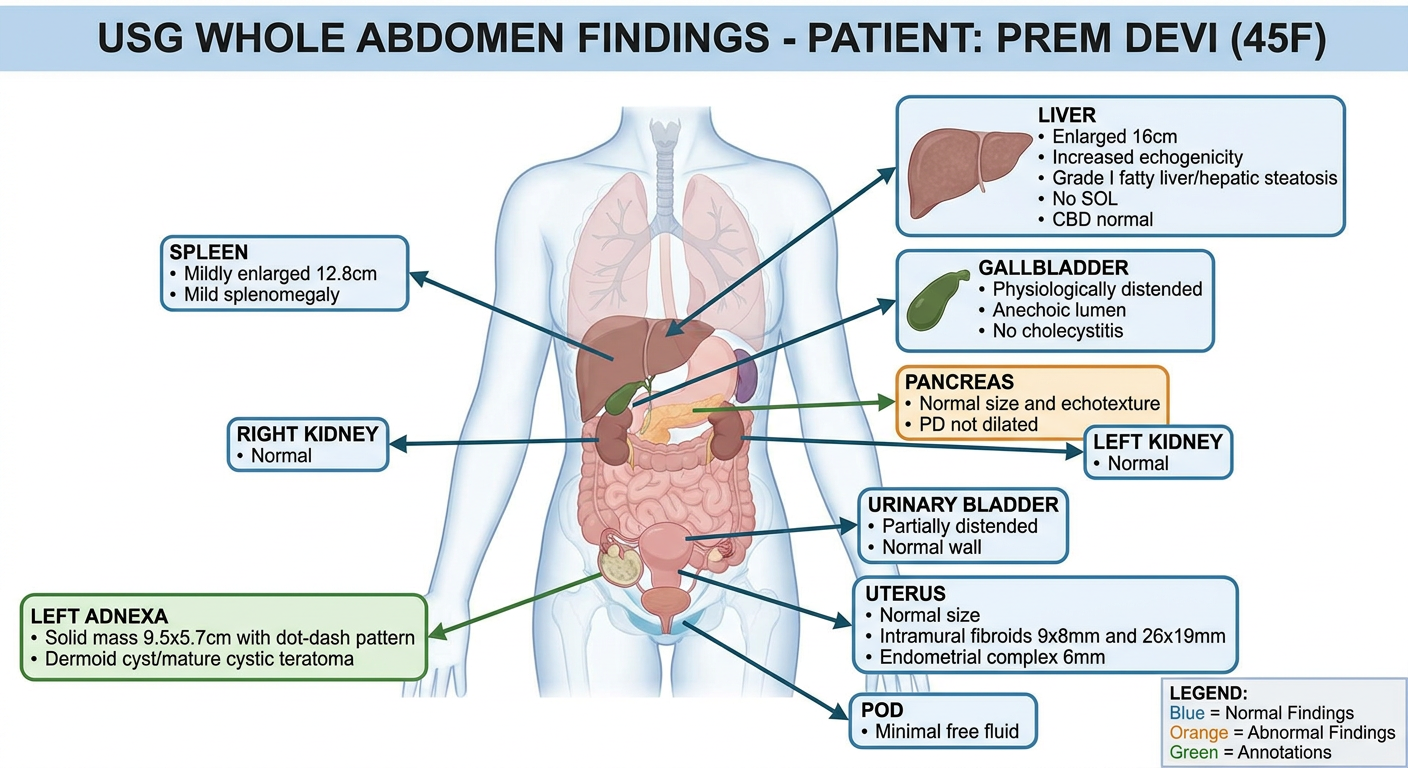
A detailed medical diagram of USG Whole Abdomen findings for a 45-year-old female patient named Prem Devi. The diagram shows a front view of the human abdomen with labeled anatomical organs and their ultrasound findings clearly annotated. Organs shown: Liver (enlarged 16cm, increased echogenicity, grade I fatty liver/hepatic steatosis, no SOL, CBD normal), Gallbladder (physiologically distended, anechoic lumen, no cholecystitis), Pancreas (normal size and echotexture, PD not dilated), Spleen (mildly enlarged 12.8cm, mild splenomegaly), Right Kidney (normal), Left Kidney (normal), Urinary Bladder (partially distended, normal wall), Uterus (normal size, intramural fibroids 9x8mm and 26x19mm, endometrial complex 6mm), Left Adnexa (solid mass 9.5x5.7cm with dot-dash pattern, dermoid cyst/mature cystic teratoma), POD (minimal free fluid). Include a color-coded legend. Clean medical illustration style with arrows and callout boxes for each finding.
Diagrammatic Representation
USG Whole Abdomen - Report Analysis
Patient Details
| Field | Info |
|---|---|
| Name | Prem Devi |
| Age/Sex | 45 Years / Female |
| Referred by | Shiv Medical Hall |
| Date | 06-Jul-26 |
| Radiologist | Dr. Shankey Garg, MBBS MD (Radio Diagnosis) |
Organ-Wise Findings
1. LIVER - ABNORMAL
- Size: Enlarged at 16 cm (normal upper limit ~15 cm in adults)
- Echogenicity: Increased (brighter than normal on USG)
- Outline: Normal
- Hepatic vasculature: Normal
- IHBR (Intrahepatic Biliary Radicles): Not dilated
- SOL (Space Occupying Lesion): None seen
- CBD (Common Bile Duct): Normal
- Impression: Mild hepatomegaly with Grade I Fatty Liver / Diffuse Hepatic Steatosis
Grade I fatty liver means mild fat deposition in the liver parenchyma causing diffuse increase in echogenicity on ultrasound.
2. GALL BLADDER - NORMAL
- Physiologically distended (fasting state)
- Anechoic lumen (no stones/sludge)
- Normal wall thickness
- No evidence of cholecystitis
3. PANCREAS - NORMAL
- Normal size, outline, and echotexture
- Pancreatic duct (PD) not dilated
4. SPLEEN - MILDLY ABNORMAL
- Size: 12.8 cm (normal upper limit ~12 cm)
- Normal outline and echotexture
- No focal solid/cystic lesion
- Impression: Mild splenomegaly
5. KIDNEYS - NORMAL (Both sides)
- Right and Left kidneys: normal in size, shape, echotexture, and outline
- Corticomedullary differentiation well maintained
- No calculi, hydronephrosis, or masses
6. URINARY BLADDER - ESSENTIALLY NORMAL
- Partially distended
- Normal wall thickness
- No vesical calculus or mass
7. UTERUS - ABNORMAL (Key Finding)
- Normal in overall size
- Heterogeneously hypoechoic lesions in the myometrium:
- Lesion 1: ~9 x 8 mm
- Lesion 2: ~26 x 19 mm
- Both show peripheral vascularity (ring of blood flow around them)
- Endometrial complex (EC): 6 mm (normal range varies by cycle phase; 6 mm is within acceptable range post-menopause borderline)
- Impression: Intramural uterine fibroids (leiomyomas within the muscle wall)
8. ADNEXA (LEFT) - SIGNIFICANT FINDING
- Solid attenuating mass, 9.5 x 5.7 cm
- Varying echogenicity with shadowing
- No obvious vascularity within the lesion
- Internal "dot-dash" pattern - this is a classic USG sign of a dermoid cyst (also called the "dermoid mesh" or "dot-dash" appearance due to echogenic lines and dots from hair/sebum)
- Impression: Dermoid cyst / Mature Cystic Teratoma - the most common benign ovarian tumor in women of reproductive age
The dot-dash pattern is pathognomonic (highly characteristic) of a mature cystic teratoma on ultrasound.
9. POUCH OF DOUGLAS (POD) - ABNORMAL
- Minimal free fluid seen in anterior and posterior POD
- This indicates a small amount of fluid in the pelvic cavity
10. OTHER FINDINGS
- Bilateral parametrial vessels: Prominent (may be reactive/inflammatory)
- Mesenteric lymph nodes: Few, subcentimetric (~6 mm short axis), non-necrotic - likely reactive
- Bowel: Excess gas noted with mild gut wall edema - suggestive of mesenteritis
Summary of Impressions
| # | Finding | Clinical Significance |
|---|---|---|
| 1 | Mild Hepatomegaly + Grade I Fatty Liver | Commonly linked to obesity, diabetes, dyslipidemia (NAFLD) |
| 2 | Intramural Uterine Fibroids | Benign smooth muscle tumors; can cause heavy periods, pelvic pain |
| 3 | Left Adnexal SOL - Dermoid Cyst / Mature Cystic Teratoma | Benign germ cell tumor; needs surgical evaluation (laparoscopic cystectomy) |
| 4 | Mild Splenomegaly | May be associated with portal hypertension (in context of fatty liver) or infection |
| 5 | Mesenteric Lymph Nodes + Gut Wall Edema | Likely mesenteritis; needs clinical and lab correlation |
Recommendations Given by Radiologist
- Clinical correlation for intestinal pathology
- Lab investigations (LFT, CBC, CA-125, etc. would be relevant)
- TVS (Transvaginal Sonography) - for detailed pelvic organ assessment
- CECT Lower Abdomen - to better characterize the adnexal mass and rule out malignancy
- Follow-up scan after treatment
What Each Term Means (Quick Reference)
| Term | Meaning |
|---|---|
| Echogenicity | Brightness on ultrasound |
| Hypoechoic | Darker than surrounding tissue |
| Anechoic | No echoes (fluid appears black) |
| SOL | Space Occupying Lesion (mass/tumor) |
| POD | Pouch of Douglas (pelvic recess) |
| IHBR | Intrahepatic biliary radicles (bile ducts inside liver) |
| CBD | Common Bile Duct |
| PD | Pancreatic Duct |
| Corticomedullary differentiation | Distinction between outer and inner kidney layers |
| Dot-dash pattern | Classic USG sign of dermoid cyst |