Transverse fracture of External Auditory canal in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Now I have comprehensive information from the textbooks. Let me compile the full 50-mark answer.
TRANSVERSE FRACTURE OF THE EXTERNAL AUDITORY CANAL (EAC)
A Comprehensive Essay — 50 Marks | RGUHS Standard
1. INTRODUCTION
Temporal bone fractures are significant otological emergencies, occurring in 14–22% of skull base fractures. The external auditory canal (EAC) is directly involved in virtually all temporal bone fractures — particularly the posterosuperior wall — and is a key anatomical landmark for classifying the fracture and predicting functional outcomes. The classical "transverse fracture" of the EAC is one of the two traditional fracture types, the other being longitudinal. Understanding its anatomy, mechanism, clinical features, and management forms a critical component of otolaryngology postgraduate examination curriculum.
2. SURGICAL ANATOMY RELEVANT TO EAC FRACTURES
The EAC is an S-shaped canal, approximately 24 mm in length:
- Outer 1/3: Cartilaginous — mobile, with ceruminous glands
- Inner 2/3: Bony (tympanic bone anteroinferiorly + squamous bone posterosuperiorly)
- Bounded by tegmen tympani superiorly, glenoid fossa of TMJ anteriorly, mastoid posteriorly
The bony EAC is formed by:
- Tympanic plate (anteroinferior)
- Squamous temporal bone (posterosuperior)
- It is continuous medially with the tympanic ring
The Foramen of Huschke — a residual dehiscence in the anterior tympanic plate — may be present and can permit spread of parotid infections or allow herniation of TMJ contents into the canal.
"Acquired canal stenosis can be seen after temporal bone fracture if there is a circumferential injury..." — Cummings Otolaryngology, p. 2752
3. CLASSIFICATION OF TEMPORAL BONE / EAC FRACTURES
A. Traditional (Anatomical) Classification
| Feature | Longitudinal | Transverse |
|---|---|---|
| Incidence | 70–90% (majority) | 10–20% |
| Fracture axis | Parallel to petrous ridge | Perpendicular to petrous ridge |
| Force direction | Temporoparietal blow | Occipital or frontal blow |
| EAC involvement | Posterosuperior wall torn | EAC may be completely disrupted |
| TM | Torn, bleeding | Intact (often) |
| Hearing loss | Conductive (±SNHL) | SNHL (severe/profound) |
| Facial nerve | 20% (horizontal segment) | 50% (labyrinthine/geniculate) |
| Labyrinth | Spared (labyrinthine concussion) | Destroyed |
| Vertigo | Mild/absent | Severe, prolonged |
"Transverse fracture destroys auditory and vestibular function; the patient has no hearing or vestibular response in that ear. Initially severely vertiginous with spontaneous nystagmus whose fast component is away from the injured side." — K.J. Lee's Essential Otolaryngology, p. 79
B. Modern Classification (Otic Capsule Based — Preferred for RGUHS)
Proposed by Dahiya et al. (1999) and now standard in Cummings:
| Type | Description | Complications |
|---|---|---|
| Otic Capsule–Sparing (OCS) | Fracture spares cochlea/SCCs | Conductive/mixed HL, CHL from ossicular damage |
| Otic Capsule–Disrupting (OCD) | Passes through cochlea/SCCs | Profound SNHL, 30–50% FN palsy, CSF fistula |
Key Statistics (Cummings, p. 2790):
- OCD fractures: fourfold to fivefold higher risk of facial paralysis
- OCD fractures: twofold to fourfold increased risk of CSF fistula
- OCD fractures: 25 times more likely to have SNHL
- OCD fractures: 8 times more likely to have CSF otorrhea
Most transverse fractures are otic capsule–disrupting (OCD). Most longitudinal fractures are otic capsule–sparing.
4. FRACTURE LINE IN TRANSVERSE FRACTURE — PATHOANATOMY
TRANSVERSE FRACTURE PATH
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Occipital/frontal force
↓
Foramen Magnum
↓
Petrous pyramid (perpendicular course)
↓
OTIC CAPSULE (cochlea + SCCs) — DISRUPTED
↓
Internal Auditory Meatus (IAM)
↓
Labyrinthine segment of Facial Nerve — commonly injured
↓
Foramen Lacerum / Middle Cranial Fossa
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
In pure transverse fracture, the EAC wall may be intact on otoscopy, but the tympanic membrane is typically intact (though hemorrhagic/blue). This is in contrast to longitudinal fractures, where the posterosuperior canal wall is classically torn and the drum lacerated.
EAC involvement in transverse fracture:
- The fracture line crosses medial to the EAC
- The bony annulus may be fractured
- Canal skin is preserved — no laceration seen
- Hemotympanum (blue-black TM) is characteristic
- EAC may appear normal externally but HRCT reveals medial bony disruption
5. ETIOLOGY AND EPIDEMIOLOGY
| Cause | Frequency (Cummings) |
|---|---|
| Motor vehicle accidents | 31% (largest single cause) |
| Motorcycle accidents | ~15% |
| Assault/Violence | Increasing trend |
| Falls | ~25% |
| Miscellaneous | Remainder |
- Age group: 70% in 2nd–4th decade of life
- Sex ratio: Males > Females (3:1)
- Bilateral fractures: 9–20% of cases
- 60% are open fractures (CSF leak, bloody otorrhea, or brain herniation)
"The force of lateral impact required to fracture the temporal bones of fresh cadavers is estimated at 1875 pounds" — Cummings Otolaryngology, p. 2790
6. CLINICAL FEATURES OF TRANSVERSE FRACTURE
Symptoms:
- Profound sensorineural hearing loss (ipsilateral) — hallmark
- Severe vertigo with nausea/vomiting — immediate onset
- Tinnitus (roaring or high-pitched)
- Facial nerve palsy — 50% cases, usually immediate onset
- CSF otorrhea — if dura torn (via middle ear → eustachian tube, drains as clear nasal discharge or via intact TM as clear otorrhea)
Signs:
| Sign | Finding |
|---|---|
| Battle's sign | Postauricular ecchymosis — delayed (24–48 h), pathognomonic of temporal bone fracture |
| Hemotympanum | Blue-black intact TM — most common finding in transverse fracture |
| EAC | Intact canal wall, no laceration (unlike longitudinal) |
| Raccoon eyes | Periorbital ecchymosis — anterior skull base involvement |
| Facial palsy | UMN type spared (Bell's palsy is LMN); immediate onset = poor prognosis |
| Nystagmus | Spontaneous, fast component AWAY from injured ear (irritative initially) |
| Hearing test | Weber lateralizes to NORMAL ear (SNHL ipsilateral) |
"Ecchymosis overlying the mastoid (Battle sign) is indicative of temporal bone fracture." — Cummings Otolaryngology, p. 2745
7. INVESTIGATIONS
A. AUDIOLOGICAL
| Test | Finding in Transverse Fracture |
|---|---|
| Pure Tone Audiogram (PTA) | Profound SNHL (flat or sloping) |
| Impedance Audiometry | Type A or B if hemotympanum; absent stapedial reflex |
| ABR (Auditory Brainstem Response) | Absent or markedly abnormal |
| OAEs (Otoacoustic Emissions) | Absent — cochlear damage |
| Tuning Fork Tests | Weber → normal ear; Rinne positive (SNHL) |
B. VESTIBULAR
| Test | Finding |
|---|---|
| ENG/VNG (Electronystagmography) | Canal paresis on caloric testing (affected side) |
| VEMP (Vestibular Evoked Myogenic Potentials) | Absent (saccular/utricular damage) |
C. FACIAL NERVE TESTING
| Test | Significance |
|---|---|
| Electroneuronography (ENoG) | Gold standard; >90% degeneration in 6 days → surgical exploration |
| Electromyography (EMG) | Fibrillation potentials = degeneration; voluntary MUPs = recovery |
| Hilger nerve stimulator | Used days 3–7; loss of stimulability = indication for surgery |
| Schirmer's test | Reduced lacrimation = geniculate ganglion or proximal involvement |
| Stapedial reflex | Absent = nerve involvement at or proximal to stapedius branch |
D. RADIOLOGY
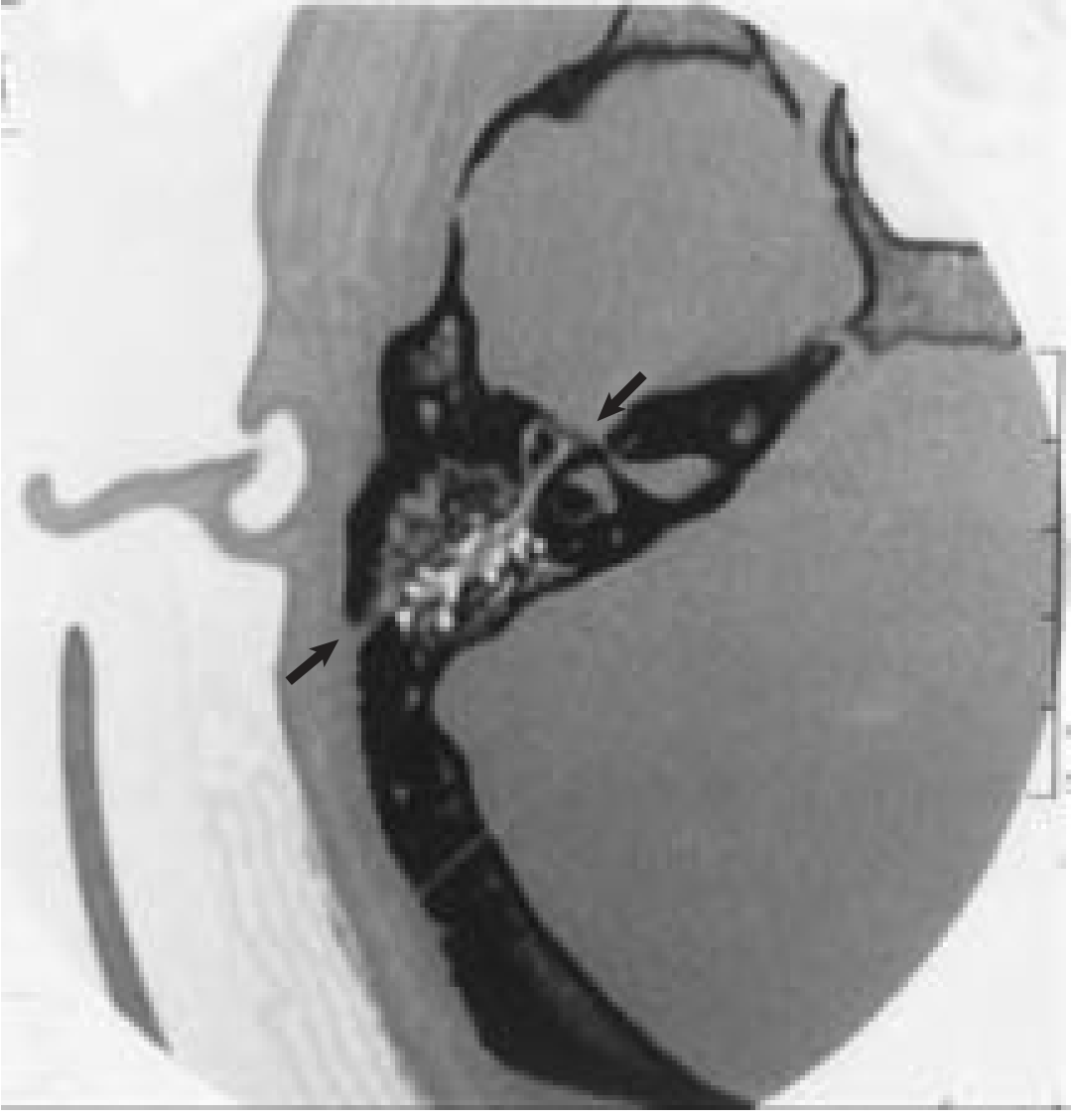
HRCT Temporal Bone — Investigation of choice
- 1 mm axial + coronal cuts
- Demonstrates fracture line, otic capsule disruption, hemotympanum
- Detects ossicular dislocation (better on coronal cuts)
- Evaluates mastoid air cells, tegmen, and carotid canal
MRI of brain and temporal bone:
- Detects intracranial complications (epidural/subdural hematoma, cerebral edema)
- Identifies dural tears and herniation
- Better for soft tissue (facial nerve enhancement, brain injury)
8. COMPLICATIONS OF TRANSVERSE FRACTURE
A. Immediate
- Profound SNHL (virtually always in true transverse = OCD)
- Severe vertigo
- Facial nerve palsy (50%)
- CSF leak (otorrhea or rhinorrhea via ET)
- Intracranial hemorrhage (epidural/subdural)
B. Early (Days to Weeks)
- Meningitis
- 1% incidence without CSF fistula
- 5–11% with CSF fistula < 1 week
- Up to 88% if CSF leak persists indefinitely
- Encephalitis
- Carotid artery injury/thrombosis
- Jugular vein injury
C. Late (Months)
- Cholesteatoma (if canal skin disrupted — more common in longitudinal)
- Persistent SNHL / total deafness
- Post-traumatic endolymphatic hydrops
- Perilymph fistula
- Ossicular discontinuity (rarely in transverse)
- Canal stenosis / atresia
"Meningitis occurs in 5% to 11% of CSF fistulas that persist for less than 1 week; the percentage increases up to 88% if left to leak indefinitely." — Cummings Otolaryngology, p. 2789
9. MANAGEMENT
A. Emergency/Primary Management
INITIAL MANAGEMENT FLOWCHART
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Head trauma → Temporal bone fracture suspected
↓
1. SECURE AIRWAY, BREATHING, CIRCULATION (ATLS)
2. Neurosurgical consultation (ICH? ICP?)
3. HRCT Head + HRCT Temporal Bone
↓
Assess:
(a) Facial nerve function — Immediate or delayed?
(b) Hearing loss — CHL or SNHL?
(c) CSF leak?
(d) Vertigo
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
General measures:
- Head elevation (30°)
- Avoid nose-blowing, straining, Valsalva
- No aural syringing or instrumentation
- Prophylactic antibiotics: controversial — not routinely recommended (Cummings)
- Steroids: High-dose methylprednisolone for SNHL (controversial but used)
- Tetanus prophylaxis if open wound
B. Management of CSF Leak
CSF OTORRHEA / RHINORRHEA
↓
Conservative management initially:
• Bed rest, head elevation
• Avoid nose-blowing
• Serial clinical observation
↓
↙ ↘
Resolves Persists > 7–10 days
in 1–2 wks ↓
(most cases) Lumbar drain or
surgical repair
(transmastoid dural repair
or middle fossa approach)
- 80% of CSF leaks resolve spontaneously within 1–2 weeks
- Persistent leak: lumbar drain → surgical repair if still persistent
- Surgical obliteration of mastoid with fat/muscle when SNHL is profound
C. Management of Facial Nerve Palsy — Key RGUHS Topic
FACIAL NERVE PALSY ALGORITHM (After Cummings / House-Brackmann system)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
Temporal Bone Fracture + Facial Palsy
↓
┌──────────┴──────────┐
DELAYED onset IMMEDIATE onset
(after lucid interval) (at time of injury)
↓ ↓
Oral steroids ENoG Day 3–7
(prednisolone 1mg/kg) ↓
+ observe ┌─────┴──────┐
↓ <90% ≥90% degeneration
Most recover degeneration within 6 days
HB Grade I–II ↓ ↓
Continue SURGICAL EXPLORATION
steroids + + DECOMPRESSION
observe
SURGICAL APPROACH:
• Otic capsule–DISRUPTING (transverse) → Translabyrinthine approach
• Otic capsule–SPARING (longitudinal) → Transmastoid/supralabyrinthine approach
(or combined transmastoid + middle cranial fossa if needed)
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
House-Brackmann (HB) Grading:
| Grade | Description |
|---|---|
| I | Normal |
| II | Slight dysfunction |
| III | Moderate — eye closes with effort |
| IV | Moderate-severe — incomplete eye closure |
| V | Severe — barely perceptible movement |
| VI | Complete paralysis |
"The most important prognostic factor in facial paralysis following temporal bone fractures is whether onset of complete paralysis is immediate upon admission to the emergency department." — Cummings Otolaryngology, p. 2789
Timing of repair:
- Within 72 hours (end-to-end anastomosis if continuity disrupted)
- Cable graft (greater auricular / sural nerve) if gap > 1 cm
- Recovery range: 1 day to 1 year; 59% recover within 1 month
D. Management of SNHL
- No proven pharmacological treatment reverses traumatic SNHL
- Oral/IV corticosteroids (early, within 72 hours) — used empirically
- Contralateral CROS hearing aid if unilateral profound SNHL
- Cochlear implantation — considered if bilateral profound SNHL (cochlear anatomy permitting)
- Ossified cochlea post-fracture is a contraindication to cochlear implantation
E. Management of Vertigo
- Acute phase: Vestibular suppressants (diazepam, prochlorperazine)
- Subacute: Vestibular rehabilitation exercises (Cawthorne-Cooksey exercises)
- Spontaneous compensation occurs: severe vertigo subsides in ~1 week; unsteadiness may persist 3–6 months (KJ Lee)
- BPPV may develop post-trauma — manage with Epley maneuver
F. Management of Cholesteatoma (Late)
- Post-traumatic cholesteatoma: more common in longitudinal; rare in transverse
- Management: tympanomastoid surgery (canal wall down or up procedure)
10. COMPARISON TABLE — TRANSVERSE vs. LONGITUDINAL FRACTURE
| Parameter | Transverse | Longitudinal |
|---|---|---|
| Incidence | 10–20% | 70–90% |
| Mechanism | Occipital / frontal blow | Temporoparietal blow |
| Fracture direction | ⊥ to petrous ridge | ∥ to petrous ridge |
| EAC wall | Usually intact | Posterosuperior wall torn/stepped |
| Tympanic membrane | Intact (hemotympanum) | Perforated/lacerated |
| Ossicular damage | Rare | Common (incudostapedial joint) |
| Hearing loss | Profound SNHL | CHL ± SNHL |
| Facial nerve palsy | ~50% (immediate) | ~20% (often delayed) |
| FN injury site | Labyrinthine/geniculate | Horizontal/tympanic |
| Labyrinth | Destroyed | Spared (labyrinthine concussion) |
| Vertigo | Severe, immediate | Mild or absent |
| CSF leak | More common | Less common |
| Otic capsule | DISRUPTED | Spared |
(Scott-Brown's Otorhinolaryngology; Dhingra's Diseases of ENT; Hazarika's ENT; KJ Lee's Essential Otolaryngology; Cummings Otolaryngology)
11. SPECIFIC CONTRIBUTIONS FROM STANDARD TEXTBOOKS
Scott-Brown's Otorhinolaryngology, Head and Neck Surgery (Stell & Maran contribution):
- Classifies fractures into longitudinal (80%), transverse (10%), and mixed (10%)
- Emphasizes that transverse fractures may cross the fundus of the IAM → total SNHL
- Facial nerve involvement at the labyrinthine segment or geniculate ganglion
- Discusses Battle's sign, hemotympanum, Rinne negative (SNHL gives Rinne positive)
- Advocates transmastoid approach for longitudinal, translabyrinthine for transverse
Dhingra's Diseases of Ear, Nose and Throat:
- Transverse fracture = "perpendicular to the long axis of the petrous bone"
- Classically: intact TM + hemotympanum + profound SNHL + facial palsy + severe vertigo
- Tuning fork: Rinne positive (SNHL), Weber to normal ear
- ENoG is the gold standard investigation for facial nerve prognosis
- CSF otorrhea: initially blood-stained → clears = CSF
Hazarika's Textbook of ENT:
- Emphasizes classification including mixed fractures (10%)
- Recommends HRCT temporal bone (1 mm cuts) for diagnosis
- Management: ABC first, then specific ENT management
- Rehabilitation: vestibular exercises (Cawthorne-Cooksey)
- Addresses medicolegal aspects relevant to head trauma cases
K.J. Lee's Essential Otolaryngology:
"Because a transverse fracture destroys the auditory and vestibular function, the patient has no hearing or vestibular response in that ear. Initially, the patient is severely vertiginous and demonstrates a spontaneous nystagmus whose fast component is away from the injured side. The severe vertigo subsides after a week, and the patient may remain mildly unsteady for 3 to 6 months." — KJ Lee, p. 79
Cummings Otolaryngology (7th ed.):
- Most comprehensive. Advocates otic capsule–based classification as primary system
- Provides statistical data on facial nerve outcomes and CSF fistula rates
- Detailed facial nerve algorithm with ENoG thresholds
- HRCT imaging evidence: fracture lines, hemotympanum, tegmen dehiscence
Zakir Hussain (ENT for Medical Students / Postgraduates):
- Concise: "transverse fracture — blow to front or back of head → fracture ⊥ petrous bone → cochlea and labyrinth destroyed"
- Emphasizes clinical differentiation using tuning fork tests (essential for bedside)
- Battle's sign timing: 24–48 hours after injury
12. DIAGRAM — FRACTURE LINES IN TEMPORAL BONE
SCHEMATIC DIAGRAM — TEMPORAL BONE FRACTURES
[ANTERIOR]
┌───────────────────────────────────┐
│ SQUAMOUS TEMPORAL BONE │
│ │
←←←←←←← │ ←←←← LONGITUDINAL FRACTURE ←←← │ ←←←←←←←
(lateral │ (parallel to petrous ridge) │ (medial)
blow) │ │
│ EAC │
│ ║ │
│ ║ ← Posterosuperior │
│ ║ wall torn in │
│ ║ longitudinal Fx │
│ │
│ ╔═══════════════╗ │
│ ║ OTIC CAPSULE ║ │
│ ║ Cochlea + SCCs║ │
│ ╚═══════════════╝ │
│ ↑↑ │
│ ↑↑↑ TRANSVERSE FRACTURE ↑↑↑ │
│ (perpendicular to petrous ridge) │
│ (passes THROUGH otic capsule) │
│ ↑↑ │
[POSTERIOR] (force from occiput)
13. FLOWCHART — COMPLETE MANAGEMENT ALGORITHM
TEMPORAL BONE FRACTURE — COMPREHENSIVE MANAGEMENT
TRAUMA / HEAD INJURY
↓
ABCs + Neurosurgical evaluation
HRCT Head + HRCT Temporal Bone
↓
├──────────────────────────────────────┐
↓ ↓
LONGITUDINAL/OCS FRACTURE TRANSVERSE/OCD FRACTURE
↓ ↓
• Conductive HL • Profound SNHL
• Torn canal wall + TM perf • Hemotympanum (intact TM)
• Ossicular dislocation? • No canal wall tear
• Facial palsy ~20% • Facial palsy ~50%
↓ ↓
┌────┴────┐ ┌────────┴────────┐
↓ ↓ ↓ ↓
Hearing Facial Hearing Facial
Loss Palsy Loss Palsy
↓ ↓ ↓ ↓
PTA + ENoG PTA + ABR ENoG
Impedance Day 3–7 Audiogram Day 3–7
↓ ↓ ↓ ↓
CHL → <90%: obs + Profound SNHL <90%: steroids
Wait 3mo steroids No treatment observe
Ossicular >90%: surgery reverses it >90% within
reconstr. Steroids tried 6 days →
(TORP/PORP) Cochlear implant TRANSLABYRINTHINE
if bilateral EXPLORATION
CSF LEAK:
• Bed rest + head elevation
• Resolves in 1–2 wk (80%)
• Persistent: Lumbar drain → Surgical repair
VERTIGO:
• Acute: Vestibular suppressants
• Subacute: Cawthorne-Cooksey exercises
• BPPV: Epley maneuver
MENINGITIS PROPHYLAXIS:
• Not routinely recommended
• Treat meningitis if it develops (culture-directed)
14. RECENT ADVANCES (RGUHS Relevant)
1. HRCT with 3D Reconstruction
- Sub-millimeter (0.5 mm) HRCT with multiplanar 3D volumetric reconstructions improve fracture line detection and surgical planning over traditional axial cuts.
2. Otic Capsule-Based Classification as Standard
- Dahiya et al. (1999) and subsequent studies have validated that OCS vs. OCD classification predicts outcomes far better than longitudinal vs. transverse classification, and is now the preferred system in Cummings (7th ed.).
3. ENoG-Guided Surgical Decision Making
- Fisch's criterion (>90% degeneration by ENoG within 6 days) remains the benchmark. Studies confirm decompression within 2 weeks yields HB I–II in 73–95% of patients when neural continuity is maintained.
4. Endoscopic Approaches
- Endoscopic-assisted middle ear exploration and ossicular reconstruction (PORP/TORP) via transcanal approach, with reduced morbidity vs. traditional post-auricular approaches. Endoscopic access to the horizontal facial nerve segment in otic-capsule–sparing fractures is an emerging technique.
5. Cochlear Implantation Post-Fracture
- After transverse fractures causing bilateral profound SNHL, cochlear implantation has become a viable option. Challenges include: obliterated/fibrotic cochlear lumen, distorted electrode insertion, and CSF gusher at cochleostomy. Imaging-guided (MRI FIESTA sequence) pre-implant workup is recommended.
6. Intratympanic Steroids for Post-Traumatic SNHL
- Emerging evidence supports intratympanic dexamethasone (IT-dexa) as rescue therapy for post-traumatic SNHL, analogous to sudden SNHL protocols. Systematic reviews suggest modest benefit when started early (< 72 hours).
7. Minimally Invasive Facial Nerve Decompression
- The supralabyrinthine approach (transmastoid without labyrinthine sacrifice) now allows decompression of the geniculate ganglion and labyrinthine segment without a middle fossa craniotomy in selected patients, reducing morbidity.
8. Post-Traumatic BPPV
- Recognized as the most common vestibular sequela after temporal bone fracture. Horizontal canal BPPV (canalith repositioning by BBQ/Lempert roll) and posterior canal BPPV (Epley maneuver) are specifically addressed in post-trauma vestibular rehabilitation protocols.
9. Virtual Surgical Planning
- Emerging role of pre-operative VR and CT-simulation for planning transmastoid and middle fossa decompression in complex fractures.
15. SUMMARY TABLE FOR QUICK REVISION
| Feature | Transverse EAC/Temporal Bone Fracture |
|---|---|
| Incidence | 10–20% of temporal bone fractures |
| Mechanism | Occipital or frontal blow |
| Fracture direction | ⊥ to petrous ridge (foramen magnum → otic capsule → middle cranial fossa) |
| Otic capsule | Disrupted |
| EAC wall | Intact (no step deformity or laceration) |
| TM | Intact — hemotympanum (blue-black) |
| Hearing loss | Profound SNHL (cochlear destruction) |
| Facial palsy | ~50%, labyrinthine/geniculate segment, often immediate |
| Vertigo | Severe, immediate; subsides 1 week; residual 3–6 months |
| CSF leak | Common (otorrhea via ET → rhinorrhea) |
| Battle's sign | Present (mastoid ecchymosis) |
| Investigation of choice | HRCT temporal bone (1 mm cuts) |
| FN assessment | ENoG (gold standard) |
| Surgical approach | Translabyrinthine (hearing already lost) |
| Prognosis (hearing) | Uniformly poor (total SNHL) |
| Prognosis (facial) | Depends on onset: delayed onset = excellent; immediate onset with >90% ENoG = surgery |
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery, 7th ed. — Chapter 147: Temporal Bone Fractures (pp. 2789–2798)
- K.J. Lee's Essential Otolaryngology, 11th ed. — Temporal Bone Fracture and Labyrinthine Concussion (p. 79)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery (Stell & Maran) — Trauma to the ear
- Dhingra's Diseases of Ear, Nose and Throat & Head and Neck Surgery — Temporal bone fractures
- Hazarika P. — Textbook of ENT and Head & Neck Surgery — Trauma
- Zakir Hussain — ENT for Medical Students/Postgraduates — Otological Trauma
- Dahiya R, Keller JD et al. (1999) — Temporal bone fractures: otic capsule sparing vs otic capsule violating — J Trauma
- Brodie HA, Thompson TC (1997) — Management of temporal bone trauma — J Trauma
- Fisch U — Facial paralysis in temporal bone fractures — J Laryngol Otol
- Tintinalli's Emergency Medicine (9th ed.) — Basilar skull fractures and CSF leaks
This answer covers etiology, anatomy, classification (traditional and modern/otic capsule-based), pathology, clinical features, investigations, complete management (including flowcharts), complications, recent advances, and multi-textbook synthesis as per RGUHS 50-mark standard.
This is a shared conversation. Sign in to Orris to start your own chat.