middle meatal antrostomy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"middle meatal antrostomy" OR "middle meatus antrostomy"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Middle Meatal Antrostomy (MMA), a core step in Functional Endoscopic Sinus Surgery (FESS).
Middle Meatal Antrostomy
Definition & Rationale
Middle meatal antrostomy is the surgical enlargement of the natural ostium of the maxillary sinus, performed via the middle meatus under endoscopic guidance. It is the cornerstone of FESS, aimed at restoring physiologic mucociliary drainage and ventilation of the maxillary sinus.
- Mucociliary clearance within the maxillary sinus always converges toward the natural ostium, regardless of where an antrostomy is created. This is why preserving and incorporating the natural ostium is non-negotiable.
- The natural ostium opens at a 45° angle in the floor of the ethmoidal infundibulum, anteriorly positioned and best visualized only after removal of the uncinate process.
Prerequisite: Uncinectomy
The natural maxillary ostium cannot be visualized without first removing the uncinate process. The uncinate process is identified as a sickle-shaped structure; its removal exposes the ethmoidal infundibulum and brings the ostium into view.
Surgical steps (retrograde uncinectomy — preferred):
- A ball-tipped probe is slid into the infundibulum behind the posterior free edge of the uncinate to medialize it off the lamina papyracea (reduces orbital penetration risk).
- A pediatric backbiter punch retrogradely incises the uncinate at the junction of the upper 2/3 and lower 1/3 — this level corresponds to the natural maxillary ostium and minimizes orbital risk.
- The incision extends anteriorly until the harder lacrimal bone (anterior maxillary line) is reached — do not penetrate this bone (nasolacrimal duct injury risk).
- The superior third of the uncinate may be preserved temporarily to protect frontal recess.
Identifying the Natural Ostium
- Angled endoscopes (30°, 45°, or 70°) are critical — the natural ostium cannot be adequately seen with a 0° scope.
- The ostium is elliptical, located in the floor of the infundibulum lateral to the lower third of the uncinate.
- Accessory ostia are circular and usually in the posterior fontanelle — they must NOT be confused with the natural ostium.
- If edema obscures the ostium: follow the "mucus trail" with a small curved suction; gently probe with a maxillary sinus seeker directed inferolaterally (never directly lateral — orbital injury risk).
Performing the Antrostomy
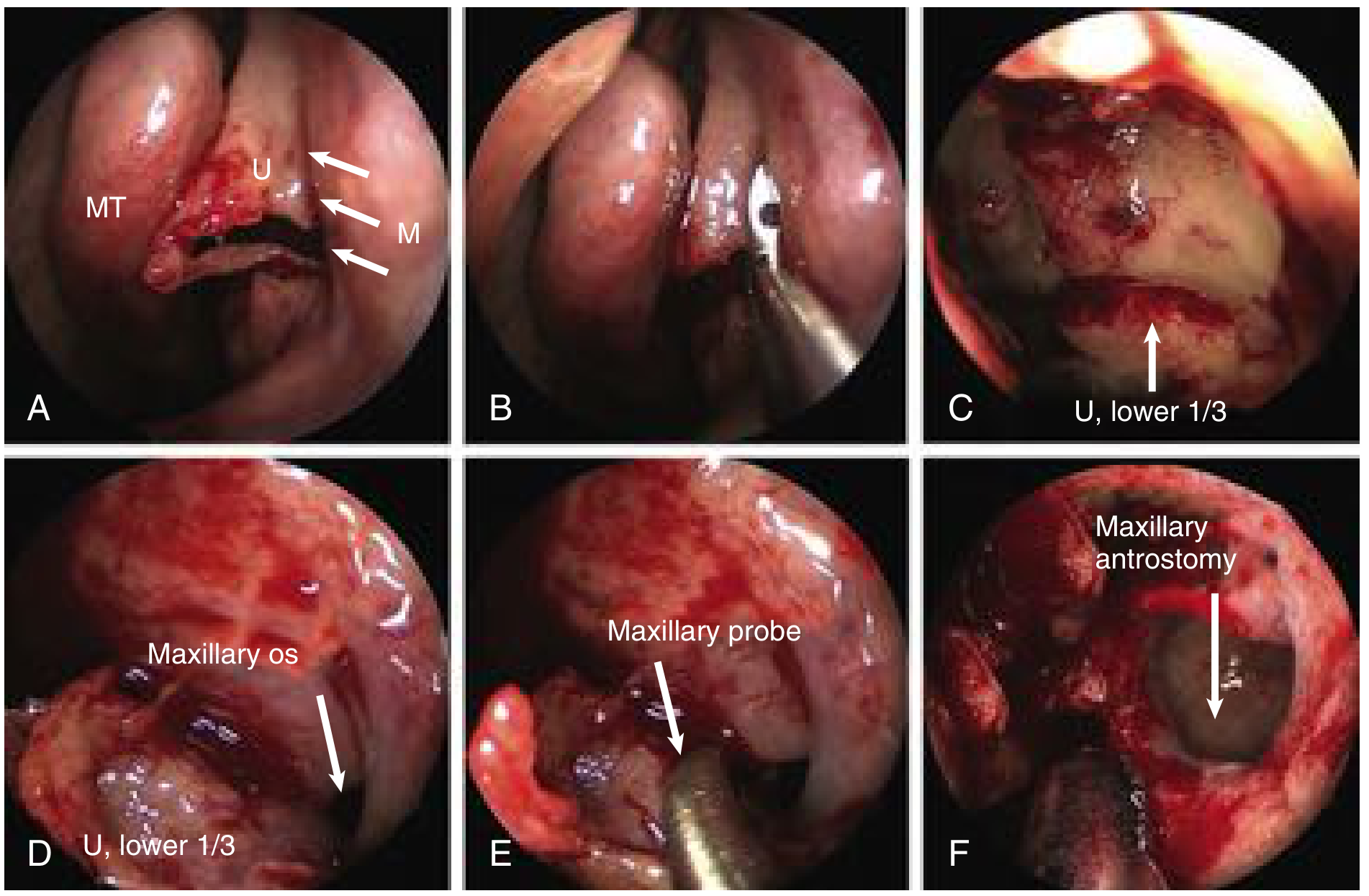
Endoscopic steps of left-sided retrograde uncinectomy and maxillary antrostomy (Cummings Otolaryngology). (A) Backbiter initiates uncinectomy at anterior maxillary line (M). (B–C) Uncinate removal. (D) Natural maxillary ostium identified. (E) Ostium dilated posteriorly with maxillary probe. (F) Completed pear-shaped antrostomy.
Step-by-step:
- A double-ball probe (or maxillary sinus seeker) is used to gently probe and dilate the natural ostium posteriorly — avoid its sharp anterior aspect to prevent circumferential scarring and stenosis.
- Do not bite anteriorly into the ostium — nasolacrimal duct injury risk.
- A straight punch can transect mucosa between medial and superior sinus walls to minimize mucosal stripping.
- Enlarge posteriorly using back-biting instruments and 90°-angled graspers (through-cutting instruments).
- Enlarge inferiorly/superiorly with side-biting antrum punches; a down-biter is useful inferiorly (avoid injuring inferior turbinate).
- Do not strip mucosa — leads to submucosal hematoma, delayed healing, and scarring/mucociliary dysfunction.
- Any accessory ostia present must be incorporated into the antrostomy to prevent mucus recirculation.
Completed antrostomy: Has a characteristic pear-shaped appearance and must include the natural ostium.
Size of Antrostomy
The appropriate size is tailored to the patient's disease:
- Standard antrostomy for straightforward CRS.
- Mega-antrostomy (maxillary mega-antrostomy): includes partial inferior turbinectomy, widening to the nasal cavity floor — indicated when mucociliary clearance is ineffective.
- Larger antrostomies are favored in CRS with nasal polyps (CRSwNP) or significant mucociliary impairment, to optimize topical drug delivery.
Extended Maxillary Sinus Procedures (Spectrum)
| Procedure | Description | Indication |
|---|---|---|
| Standard MMA | Enlarge natural ostium posteriorly ± inferiorly | CRS, localized disease |
| Mega-antrostomy | Partial inferior turbinectomy + widen to nasal floor | Mucociliary dysfunction |
| Modified medial maxillectomy | Complete inferior turbinectomy + widen to anatomic limits | Benign sinonasal neoplasms |
| Denker operation | Extension anterior to nasolacrimal duct to pyriform aperture | Far lateral/anterior disease |
| Inferior meatal antrostomy | Rarely used; risk of recirculation | Mucociliary dysfunction (select cases) |
Common Causes of Failure
(Cummings Otolaryngology, Key Points)
- Failure to incorporate the natural ostium into the MMA → mucus recirculation
- Maxillary ostium stenosis
- Lateralization of the middle turbinate
- Residual ethmoidal air cells
- Frontal recess scarring and adhesions
Post-Antrostomy Examination
After the antrostomy is complete, the sinus interior is examined with 30°, 45°, or 70° angled endoscopes. Important landmarks to identify:
- Medial and inferior orbital wall
- Infraorbital nerve (watch for infraorbital cell blocking from above)
- Any pus or debris → culture
Complications / Risks
| Risk | Related Structure | How to Avoid |
|---|---|---|
| Orbital penetration | Lamina papyracea | Keep probe inferolateral; use ball-tipped probe |
| Nasolacrimal duct injury | Anterior to ostium | Do not bite anteriorly; stop at lacrimal bone |
| Orbital injury from probe | Direct lateral probing | Always direct probe inferolaterally |
| Mucus recirculation | Missing natural ostium, separate accessory ostium | Always incorporate natural ostium |
| Scarring/stenosis | Mucosal stripping | Preserve mucosa; avoid circumferential trauma |
| Arterial bleeding | Enlarging posteriorly | Sphenopalatine artery branches posteriorly |
Sources:
- K.J. Lee's Essential Otolaryngology, pp. 616–617
- Cummings Otolaryngology: Head and Neck Surgery, pp. 882–884
This is a shared conversation. Sign in to Orris to start your own chat.