Clavicle fracture plating anaesthesia
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
clavicle fracture fixation regional anaesthesia interscalene
Searching PubMed
clavicle fracture surgery regional anesthesia
Finding Sources
Loading Image
Here is a comprehensive overview of anaesthesia for clavicle fracture plating.
Anaesthesia for Clavicle Fracture Open Reduction and Internal Fixation (ORIF)
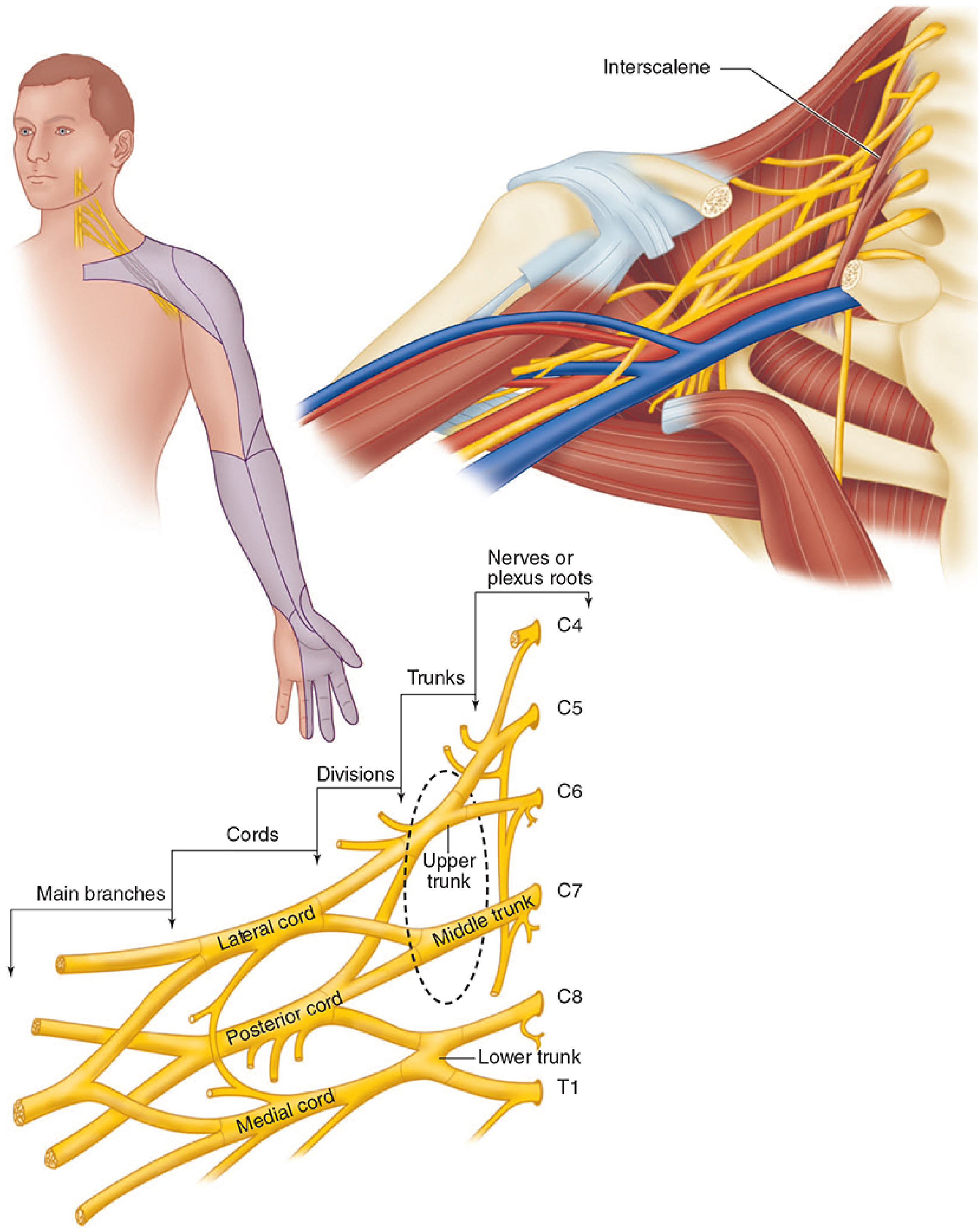
Innervation of the Clavicle — Why One Block Is Never Enough
The clavicle receives dual innervation:
- Brachial plexus (C5–C7) — deep/periosteal supply, transmitted via the supraclavicular nerves arising from the superior and middle trunks
- Cervical plexus (C3–C4) — superficial cutaneous supply via the supraclavicular nerve (cutaneous branches)
This dual supply means that no single block provides complete surgical anaesthesia. The standard approach requires combining a brachial plexus block with a cervical plexus block.
Regional Anaesthesia — Preferred Approach
1. Interscalene Brachial Plexus Block (ISB) — Primary Block
Indication: Procedures involving the shoulder, proximal humerus, and clavicle.
Mechanism: Blockade of the C5–C7 roots as they pass between the anterior and middle scalene muscles. The superior and middle trunks are the primary targets.
Technique (ultrasound-guided):
- Patient supine, head turned 30° contralaterally
- High-frequency linear probe placed transversely over the neck
- Trace the brachial plexus up from a supraclavicular view until trunks appear between scalene muscles ("stoplight" sign)
- In-plane or out-of-plane needle approach
- Volume: 10–15 mL for surgical anaesthesia; as low as 5 mL for analgesia (lower volumes reduce phrenic nerve block risk)
Limitation for clavicle surgery: Does not reliably cover the C3/C4 supraclavicular nerve. Must be supplemented.
"For complete surgical anesthesia of the shoulder as well as postoperative analgesia following clavicle surgical reduction and fixation, the supraclavicular nerve (cutaneous branch of C3 and C4) may need to be supplemented with a cervical plexus block." — Morgan & Mikhail's Clinical Anesthesiology, 7e
2. Superficial Cervical Plexus Block — Supplemental Block
Indication: Cutaneous coverage of the neck, anterior shoulder, and clavicle (C3–C4 territory).
Anatomy: All cutaneous branches of the cervical plexus coalesce posterior to the sternocleidomastoid (SCM), approximately halfway between its clavicular origin and mastoid insertion.
Technique (landmark):
- Patient supine, head rotated contralaterally
- Identify the posterior border of SCM at its midpoint
- Insert needle, direct cephalad → inject 5–10 mL subcutaneously; redirect caudally → inject further 5–10 mL
- Dilute LA (e.g., 0.25% bupivacaine) is appropriate — this is essentially a field block
Ultrasound-guided: Identify cutaneous nerves as round hypoechoic structures in the fascial plane deep to SCM; hydrodissect with 5–10 mL.
3. Alternative: Clavipectoral Fascia Plane Block (Emerging Technique)
A newer technique described for midshaft clavicle fractures. A 2024 cadaveric study (PMID: 38678917) and case report (PMID: 39056524) support feasibility for clavicle fracture surgery, though robust RCT data are not yet available.
Phrenic Nerve Block — Key Consideration
The ipsilateral phrenic nerve (C3–C5) is almost inevitably blocked with a standard ISB, resulting in hemidiaphragmatic paresis. This can cause:
- Subjective dyspnoea
- Hypercapnia and hypoxaemia in susceptible patients
- Up to ~25% reduction in respiratory function
Mitigation strategies:
- Reduce LA volume to ≤5 mL (may preserve block quality with US guidance)
- Use a superior trunk block or anterior suprascapular nerve block — these are "lung-sparing" alternatives that provide comparable shoulder/clavicle analgesia with significantly less diaphragmatic paresis
Absolute contraindications to ISB:
- Contralateral phrenic nerve palsy
- Bilateral ISB (absolutely contraindicated)
- Severe respiratory disease (consider lung-sparing alternatives)
Relative contraindications:
- Severe coagulopathy
- Local infection
- Patient refusal
- Contralateral vocal cord paralysis (recurrent laryngeal nerve block may cause distress)
Other ISB Complications to Know
| Complication | Mechanism | Notes |
|---|---|---|
| Hemidiaphragmatic paresis | Phrenic nerve (C3–C5) block | Near-universal at standard volumes |
| Horner syndrome | Stellate/cervicothoracic ganglion blockade | Benign; warn patient |
| Hoarseness | Recurrent laryngeal nerve block | Usually transient |
| Pneumothorax | Proximity to apical pleura | Reduced with US guidance |
| Bezold-Jarisch reflex | Sitting position → ↓ venous return | Hypotension/bradycardia in awake sitting patients |
| Vertebral artery injection | Inadvertent intra-arterial | Even 1 mL → seizure |
| Intrathecal/epidural spread | Proximity to neuraxis | Avoid performing under heavy sedation/GA |
"Epidural and intrathecal injections have occurred with this block, primarily when done under general anesthesia... it is recommended that interscalene blocks are placed under light sedation in adult patients." — Miller's Anesthesia, 10e
General Anaesthesia
When regional anaesthesia is contraindicated or insufficient, GA is used — typically with LMA or ETT depending on patient factors. Clavicle ORIF is often performed in the semi-recumbent or beach chair position, which carries risk of:
- Venous air embolism
- Cerebral hypoperfusion (MAP monitoring at head level is important)
- Bezold-Jarisch reflex (vagal bradycardia)
GA combined with an ISB + superficial cervical plexus block provides excellent intraoperative and postoperative analgesia and reduces opioid requirements.
Postoperative Analgesia
- Continuous ISB catheter provides potent postoperative analgesia after clavicle/shoulder surgery
- Multimodal analgesia: paracetamol + NSAID + regional block reduces opioid demand
- A 2024 study (PMID: 39269465) confirmed operatively treated clavicle fractures result in significantly more opioids prescribed than non-operative management — reinforcing the value of regional techniques
Summary
| Block | Coverage | LA Volume | Key Risk |
|---|---|---|---|
| Interscalene | C5–C7 (deep/periosteal clavicle) | 10–20 mL (surgical); 5–10 mL (analgesia) | Phrenic nerve paresis |
| Superficial cervical plexus | C3–C4 (skin over clavicle) | 10–20 mL | Mild; same precautions as ISB |
| Clavipectoral fascia plane block | Midshaft clavicle (emerging) | ~20 mL | Early-stage evidence |
The gold standard for clavicle ORIF is ISB + superficial cervical plexus block, ideally ultrasound-guided, with the block performed under light sedation before or after GA induction.
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e; Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e
This is a shared conversation. Sign in to Orris to start your own chat.